
ABSTRACT
A 73-year-old man presented with bilateral leg pain and swelling, and no history of trauma or bleeding disorders. Clinical examination, biochemistry and magnetic resonance imaging of the thighs were suggestive of muscle haematomas. These progressed significantly during the admission, requiring blood transfusion. Normal vascular anatomy on computed tomography, renal and liver function, and absence of infection made a bleeding diathesis more likely. This may be caused by coagulation defects, platelet disorders and vascular fragility. An undetectable serum ascorbic acid level confirmed the clinical suspicion of scurvy, and administration of vitamin C resulted in rapid improvement. Our case provides a structured approach to the diagnosis of bleeding disorders and scurvy, a treatable and potentially fatal disease which is often forgotten.
Case history
A 73-year-old man of Asian origin with a background of ischaemic heart disease, hypertension and type 2 diabetes presented to our London hospital complaining of severe bilateral thigh and leg pain. He described a dull ache throughout the lower limbs, which was of gradual onset and deteriorated over a period of 5 months. This was exacerbated by movement rendering him unable to walk. There were no constitutional symptoms, history of trauma or alterations to his medications in the past year. He took no non-steroidal anti-inflammatory drugs (NSAIDs), anticoagulant or antiplatelet agents, and there was no family history of any bleeding disorders. The patient lived alone, was previously fully independent, a non-smoker and did not drink any alcohol. Physical examination on admission revealed bilateral swellings across the medial aspects of both thighs, with overlying bruising and purpura (Fig 1a). He was haemodynamically stable and respiratory, abdominal and neurological examinations were unremarkable. There was no palpable lymphadenopathy. His dentition was poor, with the majority of teeth absent.

Clinical signs. (a) Haematomas on admission and (b) as they progressed during hospital stay with tracking distally and purpura.
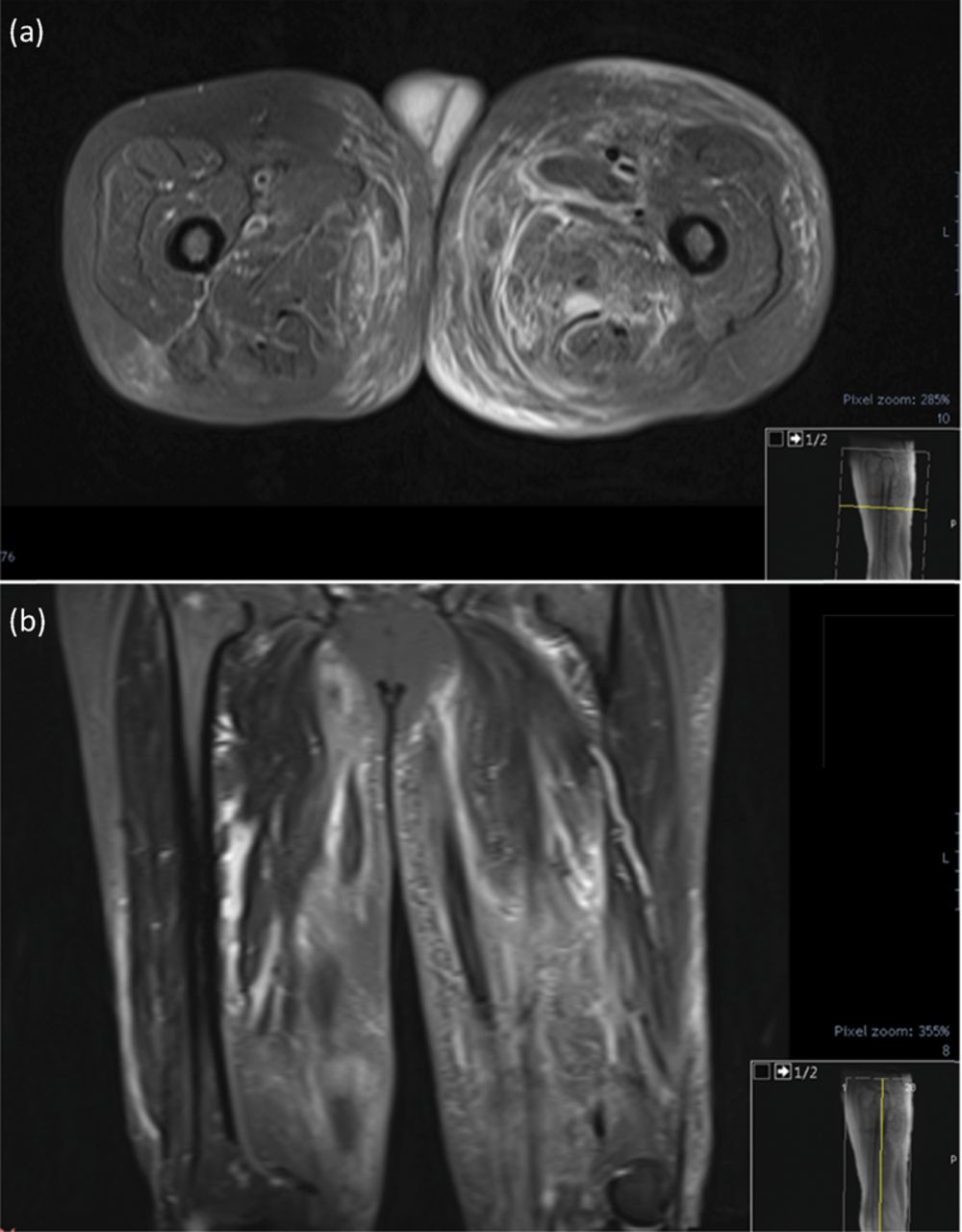
Blood tests showed a normocytic anaemia (haemoglobin [Hb] 7.8 g/dL, mean corpuscular volume [MCV] 87.4 fL, white cell count [WCC] 7.3x109/L, platelets 254x109/L), elevated inflammatory markers (C-reactive protein [CRP] 51.9 mg/L, erythrocyte sedimentation rate [ESR] 73 mm/h), and normal coagulation studies (prothrombin time [PT] 11.7 seconds [s], activated partial thromboplastin time [APTT] 31.4 s, fibrinogen 4.30 g/L), haematinics (folate 4.1 ng/mL, vitamin B12 455 pg/mL, ferritin 74 ng/mL), renal (urea 7.2 mmol/L, creatinine 92 μmol/L) and liver function (albumin 37 g/L, bilirubin 17 μmol/L, alkaline phosphatase [ALP] 80 IU/L, alanine transaminase [ALT] 13 IU/L), and creatinine kinase (92 IU/L). Raised reticulocytes (5.1%, range 0.38–2.64%) and haptoglobins (3.3 g/L, range 0.5–2 g/L), red cell anisopoikilocytosis, and a negative direct antiglobulin test were consistent with active bleeding. Serum and urine electrophoresis was negative. A computed tomography (CT) of the chest, abdomen and pelvis only showed incidental cholelithiasis, with no additional bleeding, vascular abnormality or signs of solid malignancy. A magnetic resonance image (MRI) of the thighs showed diffuse enlargement and oedema of the adductor musculature bilaterally, with appearances suggestive of haemorrhage (Fig 2).
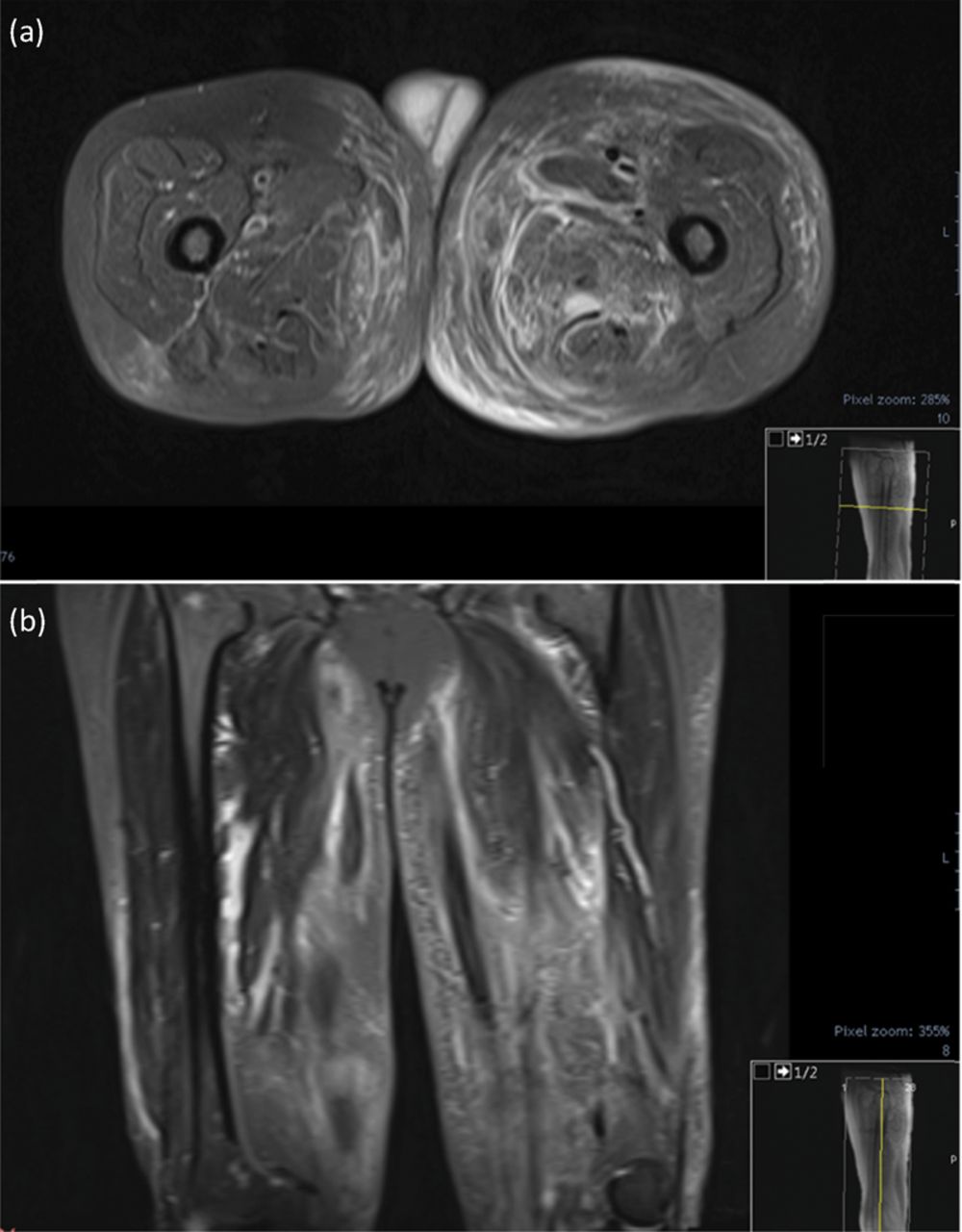
MRI of the patients’ thighs. Oedema affecting, in particular, the adductor compartment bilaterally with appearances suggestive of muscle haematoma. Axial (a) and coronal views (b). MRI = magnetic resonance imaging
New haematomas developed during the admission (Fig 1b) with an associated decrease in haemoglobin (6.5 g/dL), mandating red cell transfusion on two separate occasions and morphine for analgesia.
The clinical presentation was suggestive of a bleeding diathesis, in the absence of any significant infection, renal or liver disease. Bleeding disorders are typically a consequence of coagulation defects, platelet disorders or vascular fragility. Normal PT, APTT, factor VIII, and von Willebrand factor levels excluded significant acquired haemophilia and von Willebrand disease, while milder acquired coagulation factor deficiencies would not be expected to manifest alone with this severity. Platelet function disorders may occasionally present with normal coagulation studies, and can be secondary to medications (eg ibrutinib and NSAIDs), paraproteinaemia, herbal supplements, uraemia, and antibody-driven platelet dysfunction (eg acquired storage pool disease and Glanzmann's thrombasthenia). If clinically suspected, platelet function testing including bleeding time, PFA-100, aggregometry, platelet nucleotides, and flow cytometry for membrane glycoproteins may be helpful. More rarely, fibrinolytic system defects including alpha-2-antiplasmin deficiency can cause significant bleeding despite normal baseline clotting screen. Further causes of bleeding to consider include disorders of vascular fragility such as Ehlers-Danlos syndrome, small vessel vasculitides, drug reactions and scurvy.
In view of the clinical presentation and patient demographic, an ascorbic acid level was requested and returned undetectable (<2.8 μmol/L, range 26.1–84.6 μmol/L), leading to a diagnosis of scurvy. Administration of vitamin C 500 mg four times a day resulted in rapid improvement in pain, resolution of the haematomas and stable haemoglobin levels thereafter.
The patient had initially described his diet as healthy, but on further questioning declared omitting meals other than dinner, which consisted of poultry and rice, and never consuming fruit or vegetable products.
Discussion
The effects of vitamin C deficiency are largely attributed to its role in collagen synthesis.1 It is a cofactor for the hydroxylase enzymes that contribute to the assembly of the triple helix structure of collagen. Its absence affects tissues which are particularly dependent on collagen, such as vascular layers and connective tissue scaffolding. This results in a host of symptomatology which includes perivascular oedema, bleeding, perifollicular haemorrhages, gum disease and impaired wound healing. Non-specific constitutional features such as fatigue and weakness may be linked to anaemia which commonly accompanies scurvy, whereas myalgia can arise from decreased carnitine production.2 Ascorbic acid is also implicated in disulfide bond formation during hair shaft synthesis, which leads to a corkscrew hair appearance occasionally observed in scurvy.
Untreated, scurvy can be fatal and has indeed claimed many victims throughout human history. This is possibly as a result of refractory hypotension due to impaired vascular response to adrenergic stimuli,1 and intracranial or cardiac haemorrhagic complications.
Epidemiological data is somewhat lacking for this disease, which is considered by most a memory of days past. A report by the British Health and Social Care Information Centre on so-called ‘Victorian diseases’ in modern England found a rise in scurvy presentations to secondary care, up to 113 documented hospital cases in 2015.3 It also highlighted a peak in primary diagnoses of malnutrition, responsible for a mean hospital stay of almost 21 days.
Conclusion
Traditionally, extremes of age are thought to be at greatest risk of vitamin C deficiency, and in the case that we described social isolation may have contributed to this.
A diagnosis of scurvy is typically based on clinical grounds with resolution of symptoms within 1–2 weeks of treatment. Even in the absence of more classic features, an atypical presentation of bleeding with normal clotting studies and vascular anatomy should prompt physicians to consider scurvy. In the literature, cases of scurvy in metropolitan areas are occasionally reported, yet this illness is usually labelled as forgotten. With an ageing population that society often struggles to appropriately care for, it is perhaps time we rescue this diagnosis from the sea of history we have banished it to.
Author contributions
FF, LB, HH, AJ, and SH cared for the patient. RA provided haematology advice. YB provided pathology advice and did biochemistry analyses. FF wrote the first draft, and all authors contributed to writing of the report.
Consent
Written informed consent was obtained from the patient to publish the clinical details and images in this article.
- © Royal College of Physicians 2018. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.