
A 50-year-old woman affected by an ovarian cancer (Figo IV) was referred to our Radiotherapy Department. She had a history of a slow disease progression for over 6 years as a result of several adjuvant chemotherapy regimens. During the last chemotherapy session, she developed a gastric outlet obstruction caused by peritoneal metastases around the antrum and, as a result, she underwent a laparotomy with a Roux-en-Y side-to-side gastroenterostomy of the gastric fundus. After 2 months, multiple cerebral metastases were diagnosed and in order to treat them palliative whole brain radiotherapy was started. During this phase, the patient developed increasing abdominal and chest pain over a period of 3 days. Physical examination revealed sparse bowel sounds and constipation as well as a progressive decline in blood pressure. A blood sample showed an increase in C-reactive protein and a slight reduction in kidney function. A computed tomography scan (CT) of the chest and abdomen detected a transperitoneal communication between the stomach and the pericardium as well as a pathological air collection in the pericardial sac. The patient was transferred to the intensive care unit where a gastroscopy confirmed the diagnosis of gastropericardial fistula (Fig 1). Even though the possibility of a surgical closure of the fistula was discussed with the patient, she refused all treatment owing to the poor prognosis associated with such an advanced cancer. All therapies were consequently halted and the patient was discharged to home, where she died a week later.
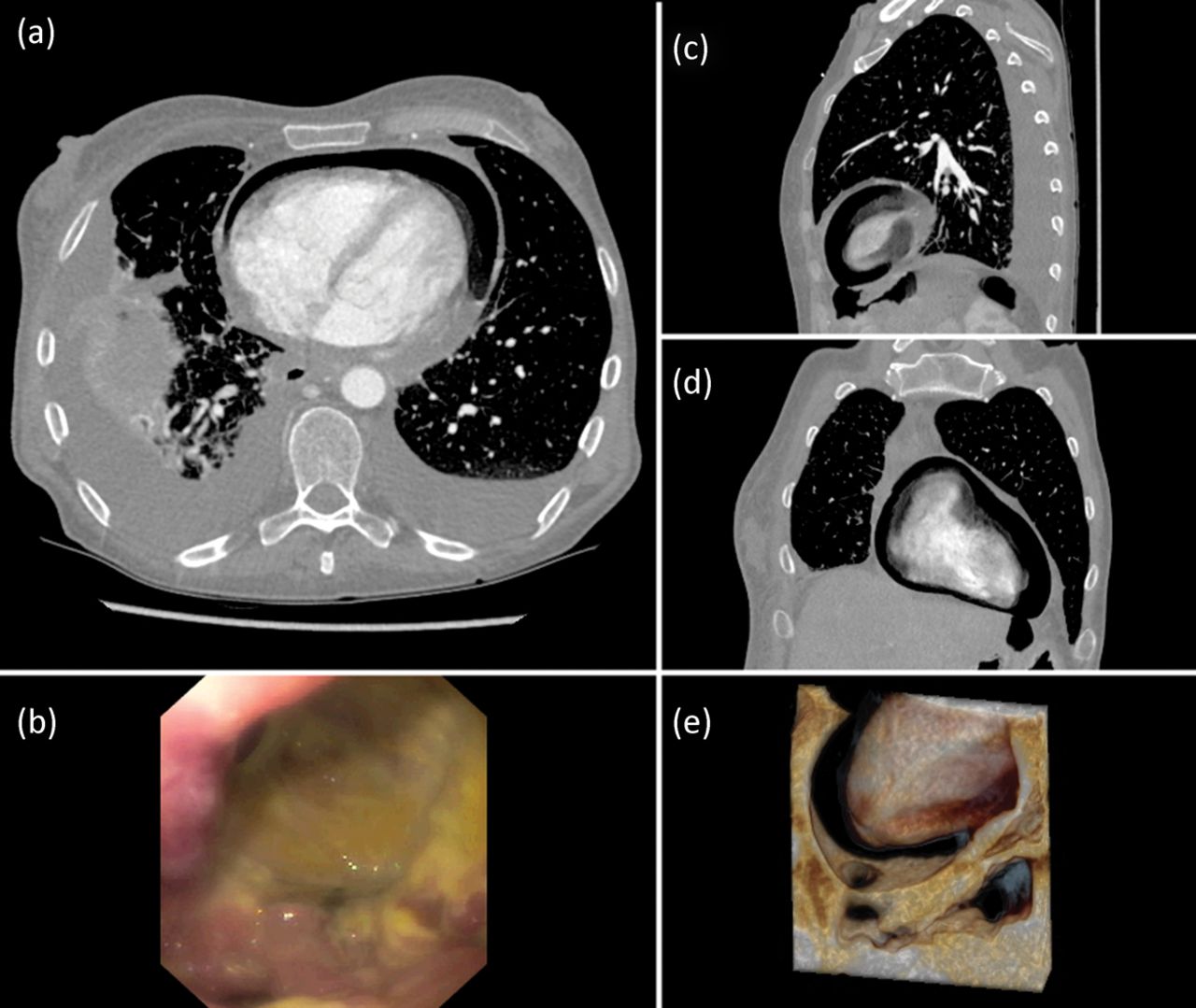
Computed tomography (CT) scan of chest and abdomen: axial (a), sagittal (c) and coronal (d) views demonstrating air in pericardial sac due to a fistula between the stomach and the pericardium. The CT scan shows in addition bilateral pleural effusions and right lung dystelectases. Endoscopic image of the fistula, view from the gastric antrum (b). Three dimensional CT reconstruction with depiction of the communication between the stomach and the pericardium (e).
Gastropericardial fistula is a rare condition associated with a high mortality rate and characterised by a direct communication between the stomach and the pericardium. Its etiology includes previous gastrointestinal surgery, perforating gastric ulcer and perforating cancer.1–2 In this case the perforation was due to an ulcerated peritoneal metastasis around the antrum and duodenal bulb. Although it is uncommon, gastropericardial fistula should be considered alongside pulmonary embolism and ileus in patients affected by peritoneal metastasis whenever they present with unexplained insidious chest and abdominal pain with hypotension. In these patients, a CT of the chest and abdomen can be helpful in providing the diagnosis.
Consent to publish
Consent to publish was obtained from the patient's next of kin.
- © Royal College of Physicians 2018. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.