
Detecting paroxysmal atrial fibrillation (PAF) is challenging given the intermittent and often asymptomatic nature of the condition. Stroke secondary prevention guidelines acknowledge that longer duration of monitoring (>24 hours) after an ischaemic stroke is likely to yield a higher frequency of PAF, but are unable to provide precise guidance on ‘how long’ to monitor after stroke.1,2 A recent systematic review suggested increased AF detection among unselected acute ischaemic stroke patients with prolonged methods of monitoring (>24 hours) but the precise method, duration and time to intervention following a stroke remains unknown.3
In the absence of robust evidence-based guidelines and the existence of advanced cardiac monitoring devices, the main objective of the survey was to explore cardiac monitoring strategies to detect PAF after an acute ischaemic stroke among stroke specialists. A questionnaire (nine questions) was created using SurveyMonkey and sent through a mailing list of the British Association of Stroke Physicians (BASP). The questionnaire included questions on demographic data of the respondents, physician perception and current practice in cardiac monitoring after an acute stroke.
A total of 101 completed responses (71 UK hospitals) were obtained accounting for about 16% of BASP membership. The majority of the respondents (84%) were consultants. Of respondents, 49% perceived that PAF is likely to be detected early after an acute stroke (<72 hours). The majority preferred non-invasive cardiac monitoring (84%), most commonly with either inpatient telemetry (33%), 7 day Holter or event recorder (ER) (23%) as opposed to invasive monitoring (16%). In actual practice, if no prior history of AF or new AF was detected on 12-lead electrocardiogram, 94% of responders used non-invasive cardiac monitoring, most commonly with inpatient telemetry (27%), 24 hour Holter (20%) or 72 hour Holter (15%). Six percent do not use any form of cardiac monitoring (Fig 1a). The interval from stroke onset to initial monitoring was most commonly >14 days (30%), while only 22% of respondents felt there was no delay or <24 hours delay. Eighty percent would repeat monitoring if PAF was not detected (Fig 1b), most commonly with a 7 day Holter (28%).
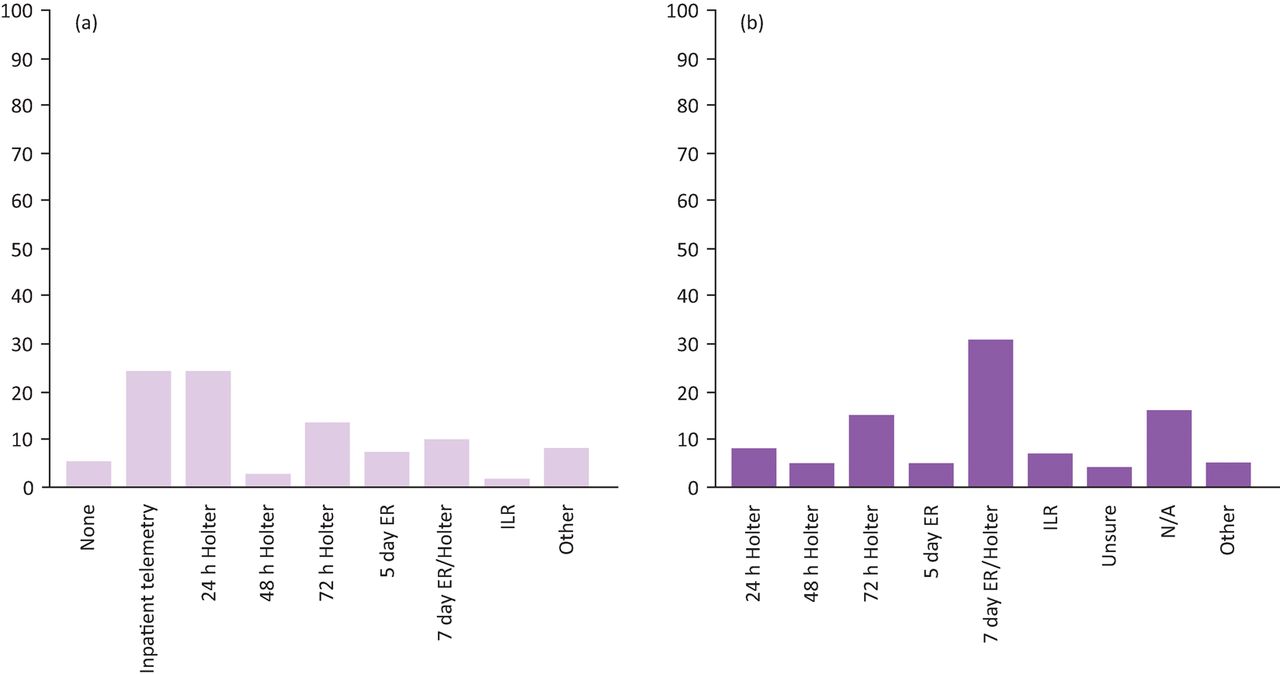
(a) Clinician practice: monitoring methods used immediately after an acute stroke (%); (b) Clinician practice: repeat cardiac monitoring used after an acute stroke (%). ER = event recorder' ILR = implantable look recorder
The results of the survey and evidence from existing research suggests it is still unclear as to ‘when’, ‘where’, ‘how’ and ‘how long’ to monitor stroke patients. There appears to be wide-spread variation in approach to cardiac monitoring immediately after an acute stroke with non-invasive cardiac monitoring (≥24 hours) the preferred method. The lack of consensus seen reflects the relative absence of research in this area and therefore lack of robust national or international guidelines on prolonged cardiac monitoring after an acute ischaemic stroke. Two studies which applied early cardiac monitoring within 48 hours4 and 7 days5 of stroke symptom onset reported new PAF in 18% and 14% respectively, suggesting PAF could perhaps be ‘front-loaded’, emphasising the importance of early cardiac monitoring. In the context of current financial constraints in the NHS, and absence of robust guidelines in AF detection strategies after an acute stroke, there is an urgent need for further research in this area and a consensus-based approach on how best to monitor patients after an acute stroke.
- © Royal College of Physicians 2018. All rights reserved.








{kind=link}