
ABSTRACT
The Royal College of Physicians (RCP) recently published the National Early Warning Score 2 (NEWS2), aiming to improve safety for patients with hypercapnic respiratory failure by suggesting a separate oxygen saturation (SpO2) parameter scoring system for such patients. A previously published study of patients (n=2,361 admissions) with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) demonstrated alternative scoring systems at admission did not outperform the original NEWS. Applying NEWS2 SpO2 parameters to this previously described cohort would have resulted in 44% (n=27/62) of patients who scored ≥7 points on the original NEWS and subsequently died being placed in a lower call-out threshold. NEWS2 loses the benefits of a unified, standardised scoring system and we suggest prospective research in this area before applying this adjustment.
Introduction
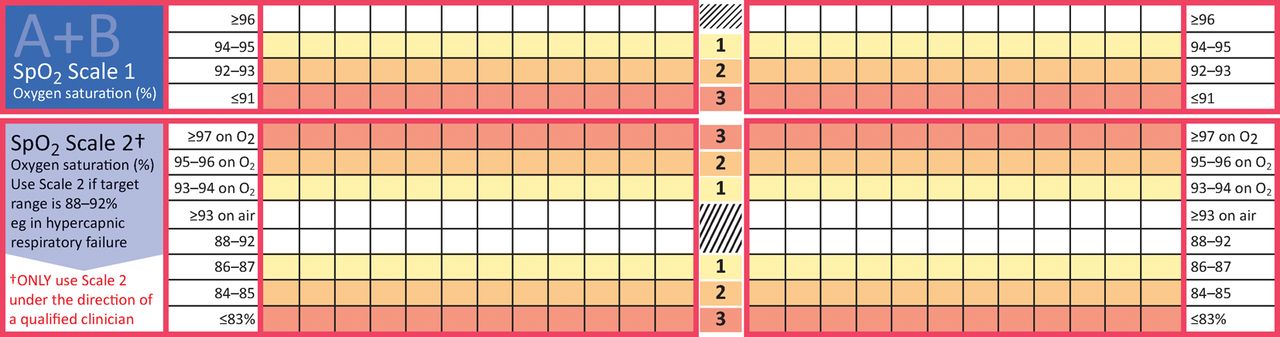
The National Early Warning Score (NEWS) is a validated mortality predictor, recommended and used as a track and trigger score in acute hospitals across the NHS.1 Due to significant concerns of NEWS over-alerting in patients with chronic respiratory conditions, two groups proposed adjusted scores for this patient subgroup.2,3 Our previous study reported the first validation of the NEWS in patients with an acute exacerbation of COPD (AECOPD) (n=2,361). The NEWS values of AECOPD patients was significantly higher than in a large contemporaneous group (n=37,109) of acute medical unit admissions (median NEWS 4 vs 1 respectively, p<0.001) despite both groups having a mortality of 5%.4 However, NEWS demonstrated similar discrimination to predict mortality compared to the alternative scores, with the CREWS and Salford-NEWS providing increased specificity at the cost of sensitivity. NEWS2, published in December 2017, aims to improve safety for patients with hypercapnic respiratory failure by suggesting an alternative scoring system for oxygen saturation (SpO2), similar to the Salford-NEWS (Fig 1).5 We aimed to assess the performance of NEWS and NEWS2 using the previously described AECOPD cohort.
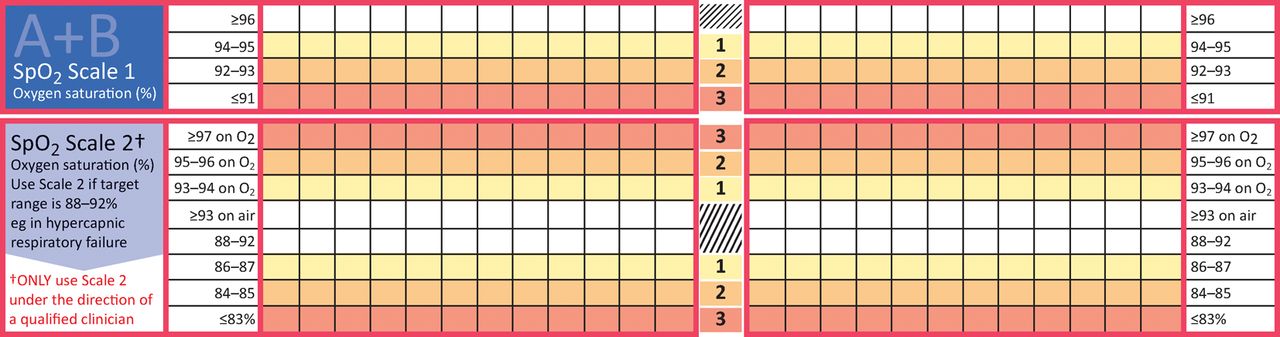
RCP NEWS and NEWS2 SpO2 scoring. Top panel – original NEWS; bottom panel– NEWS2. Reproduced with permission from the Royal College of Physicians, London.
Methods
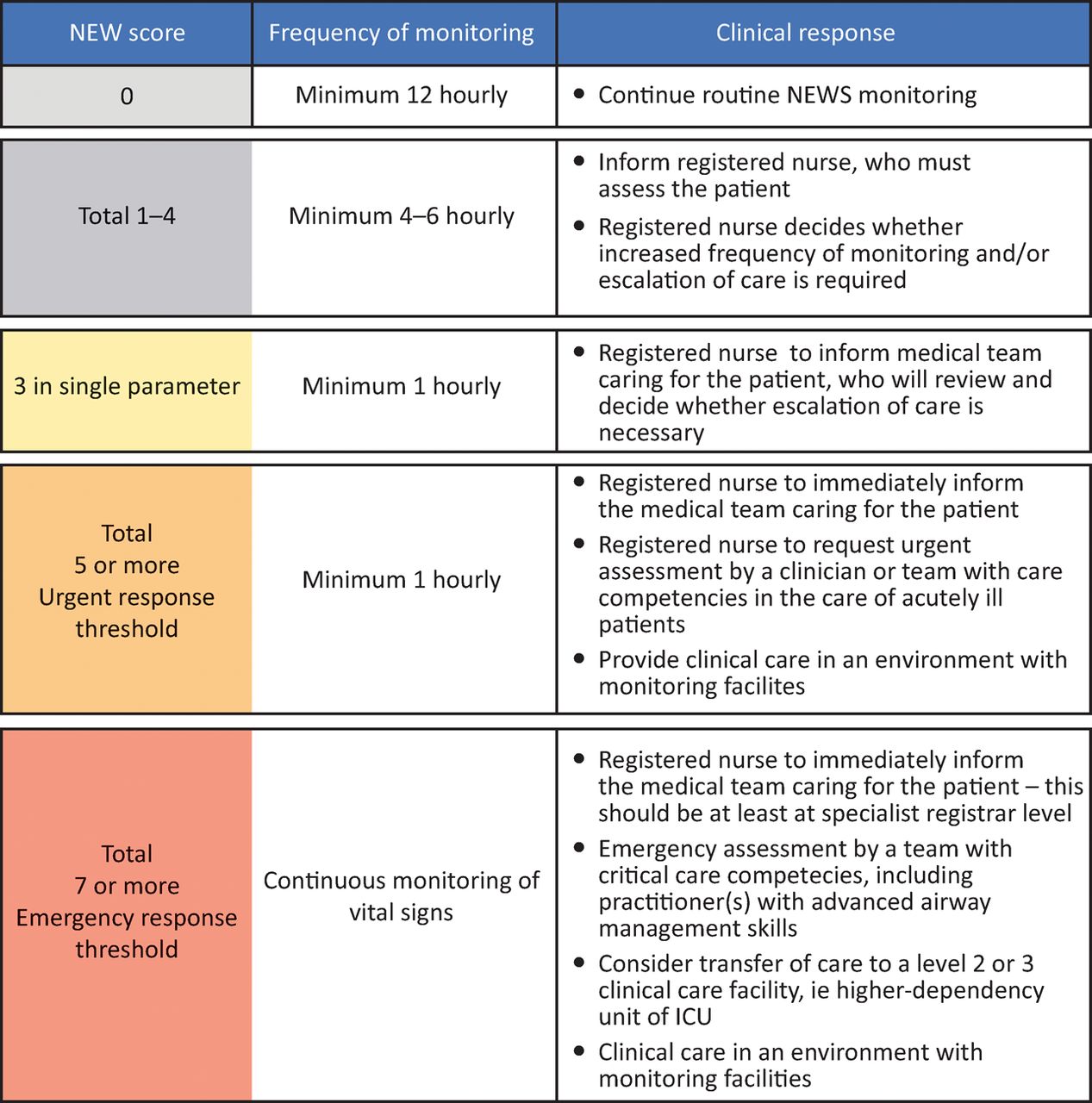
The database of a retrospective cohort study from 2012–14 was interrogated.4 Ethical approval was previously given by NHS Research Ethics Committee London-South East (REC reference 13/LO/0884) and the study followed the TRIPOD guidance for reporting of validation studies of prediction models.6 As this involved anonymised data, patient consent was not deemed necessary. NEWS has three thresholds: low (0–4 points) medium (5–6) and high (≥7) that determine, for example, subsequent frequency of observations and whether an urgent clinical response is required (Fig 2). We assessed the number of patients reclassified to lower risk groups by NEWS2 both in those who survived and in those who died during their hospital admission. Results are presented with median and interquartile ranges. Median scores were compared using Wilcoxon signed ranks test. Predictive values were also calculated at suggested NEWS call-out thresholds, to inform on the way model performance could impact on clinical workload including sensitivity, specificity, positive and negative predictive values with associated 95% confidence intervals. Statistical analysis was carried out using IBM SPSS Statistics 24.
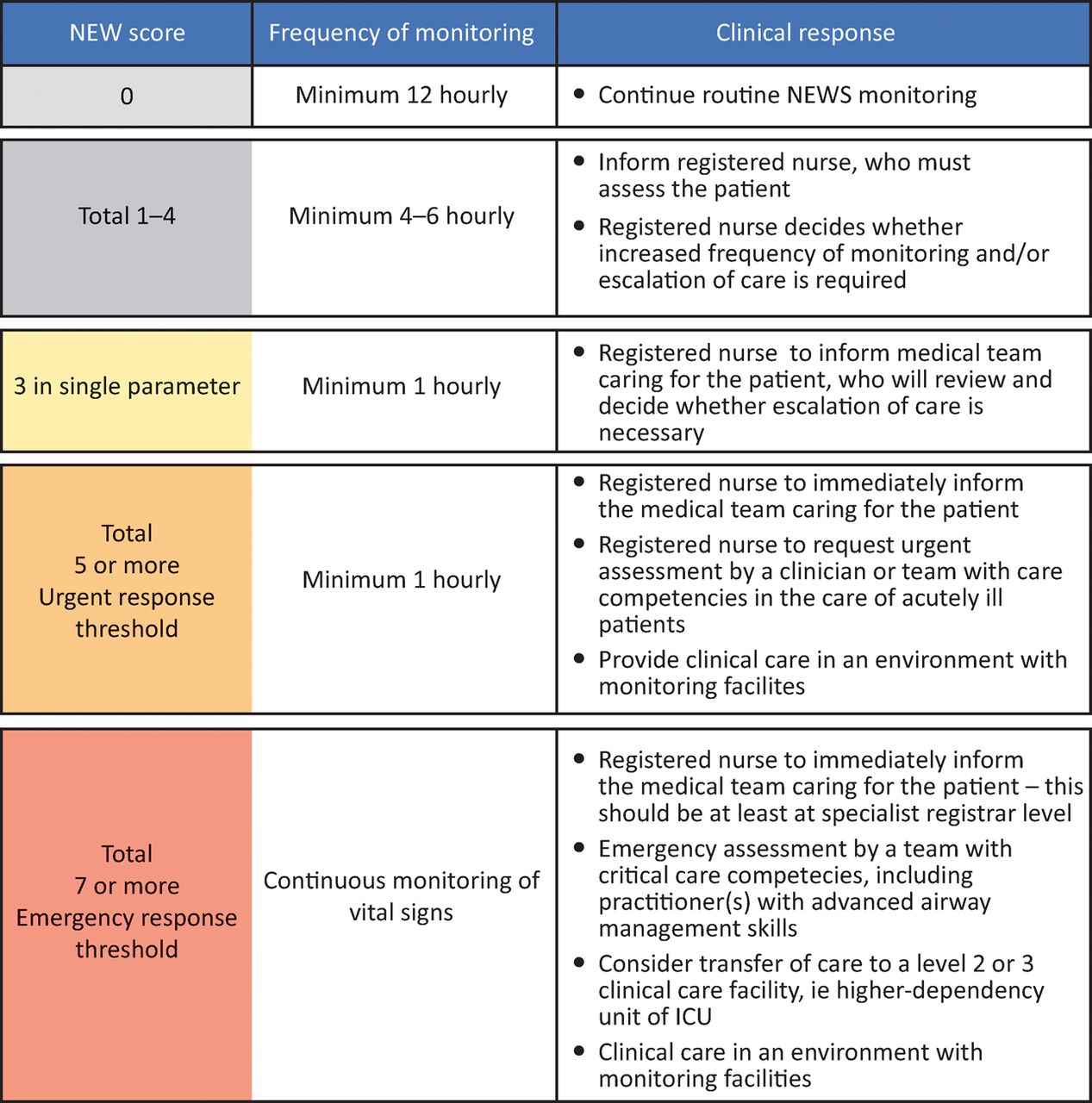
Call-out thresholds and frequency of observations and suggested seniority of responder. Reproduced with permission from the Royal College of Physicians, London. ICU = intensive care unit
Results
Over the 2-year study period there were 39,470 admissions of which 2,361 were AECOPD. The AECOPD cohort had a median age of 74 (interquartile range [IQR] 67–82), inpatient mortality was 5% (n=123). Median admission NEWS was 4 (IQR 2–6) and median NEWS2 was 3 (IQR 2–4), p<0.001 (Table 1). In the 123 patient deaths median NEWS was 7 (IQR 3–9) compared to 4 (IQR 2–8) using NEWS2 (p<0.001). Of patients who died, 62 (50%) had an admission NEWS ≥7 points; rescoring using NEWS2 SpO2 parameters 44% (n=27) of these patients would have been placed in a lower call-out threshold, reducing sensitivity. Of cases with NEWS>7 who survived (false positives for mortality) 66% (n=291/440) would have been similarly placed in a lower threshold, increasing specificity (see Table 2).
NEWS and NEW2 admission scores in the AECOPD cohort
Performance of NEWS and NEWS2 at a threshold of ≥7points.
Discussion
NEWS2 SpO2 adjustments aim to improve safety for patients with hypercapnic respiratory failure who would normally have a recommended SpO2 range of 88–92%.5,7 There are potential drawbacks to such an approach. NEWS is well validated in multiple patient settings providing standardisation with all the benefits that go with this approach. Indeed, respiratory patients were included in the NEWS derivation study and in a similar previous early warning score.8,9 A recent large Danish study found similar drops in sensitivities for 48-hour mortality and intensive care unit (ICU) admission and found that records downgraded by NEWS modifications into a lower call-out threshold were more frequently followed by 48-hour mortality or ICU admission than records with an unmodified NEWS in the same scoring threshold; this suggests that the purpose of NEWS, detecting deterioration, may be compromised by modifications.10
In our original validation paper we suggested maintaining the NEWS with its advantages of a unified approach, while emphasising the need to have patients looked after by the right specialty who understand the score in the context of that condition and can deliver optimal care, rather than adjusting a national track and trigger score. This point remains valid and links into the current RCP COPD secondary care audit in which being promptly reviewed by a respiratory specialist within 24 hours is part of the best practice tariff.11 Crucially, the NEWS score is not dependent on an accurate diagnosis, which is often revised during the initial period of an acute medical admission. We would argue that introduction of different scorings for subsets of patients is counter-intuitive to the reasoning behind the NEWS. Suggesting an adjustment for a minority of acute admissions may compromise, rather than improve, the safety of respiratory patients. For example, the 2014 BTS National Audit of AECOPD found of those who had an arterial blood gas performed (only 78% of the COPD patients), 22% were acidotic, 44% were hypercapnic and 36% were hypoxic.11 The NEWS2 report suggests blood gas analysis be performed prior to instituting the adjusted score by a competent decision maker; however, there is a risk this will be applied to all patients with AECOPD, many without a blood gas analysis. In our cohort of AECOPD admissions, we found that NEWS2 would have placed a significant number of high-risk patients who went on to die (score ≥7 points) into a lower risk call-out threshold compared to the original NEWS. While this strategy would undoubtedly lower ‘false-alarms,’ this is not without clinical risk.
Concluding remarks
Before widespread implementation of this adjustment to NEWS we would suggest utilising a large national dataset to answer a number of questions such as:
what are the best parameters to predict mortality or clinical deterioration (such as requirement for non-invasive ventilation or escalation of care) for patients with hypercapnic respiratory failure and
what are the best parameters to predict mortality for patients with AECOPD without hypercapnic respiratory failure, to answer whether lower SpO2 points weightings should be applied to all COPD admissions rather than a subgroup of a subgroup of acute hospital admissions.
Even after the above questions are addressed we would suggest serious thought is given to the proposal that a unified approach to a track and trigger score is abandoned without robust evidence to support this change.
Author contributions
LH contributed to study design, data analysis, writing up of the paper and final approval of the submitted version. JC contributed to study design, interpretation of the data, writing up of the paper and final approval of the submitted version. RV contributed to study design, data analysis, interpretation of the data, writing up of the paper, and final approval of the submitted version. LF contributed to study design, interpretation of the data, writing up of the paper, and final approval of the submitted version. PR contributed to study design, data analysis, writing and final approval of the submitted version.
- © Royal College of Physicians 2018. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- NEWS2, patient safety and hypercapnic respiratory failure
- Ability of the National Early Warning Score and its respiratory and haemodynamic subcomponents to predict short-term mortality on general wards: a prospective three-centre observational study in Finland
- COPD exacerbations: 2 much NEWS?
- Comparison of early warning scores in patients with COPD exacerbation: DECAF and NEWS score
- The National Early Warning Score 2 (NEWS2)
- The inclusion of delirium in version 2 of the National Early Warning Score will substantially increase the alerts for escalating levels of care: findings from a retrospective database study of emergency medical admissions in two hospitals
- The National Early Warning Score 2 (NEWS2) in patients with hypercapnic respiratory failure
- The challenge of change: evidence, culture and expertise