
ABSTRACT
Intracerebral haemorrhage causes 1 in 10 strokes, but has the worst overall outcomes of all stroke subtypes. Baseline haematoma volume is a key prognostic factor and early complications – such as haematoma expansion, obstructive hydrocephalus and perihaematomal oedema – may worsen outcome. There is evidence that withdrawal of care may occur more often in intracerebral haemorrhage than ischaemic stroke independent of premorbid health and stroke severity. However, recent evidence shows that reversal of anticoagulants, intensive blood pressure lowering and surgery in carefully selected cases may improve outcomes. Ongoing research may also provide evidence for new medical treatments and minimally invasive approaches to surgery. Effective implementation of evidence-based care to intracerebral haemorrhage patients can be difficult but quality improvement methodology can help to achieve maximal benefit.
Introduction
Intracerebral haemorrhage (ICH) is caused by spontaneous bleeding into the brain parenchyma and accounts for 10–15% of strokes in western populations, with a higher incidence reported in Asia.1 Survival after ICH differs from ischaemic stroke with a much higher early case fatality in ICH (34% at 1 month versus 12% for ischaemic stroke in a recent UK study2). Despite only causing 1 in 10 strokes, this high case fatality combined with a higher incidence in Asia results in ICH being responsible for a similar proportion of all global deaths as ischaemic stroke (5.8% versus 6.0%, respectively3). The majority of survivors are left with significant disability and there has been little improvement in these poor outcomes over the last 30 years.1 Unsurprisingly, combined with a relative lack of proven acute therapies, this has led to pessimism among those caring for acute stroke patients. Using routinely collected stroke audit data from the Sentinel Stroke National Audit Programme (SSNAP) in the UK, we have shown that after adjusting for key demographic, premorbid and baseline characteristics, ICH patients are far more likely to have palliative care commenced on the day of admission than ischaemic strokes (odds ratio: 7.27, 95% CI: 6.31–8.37, p<0.001).2 However, there has been a growing interest in ICH in the stroke research community and findings from recent studies suggest that a more active approach to this patient group is now warranted. We will focus this review on evidence for key interventions in the hyperacute phase of ICH management, that is, the first 24 hours after symptom onset.
Early neurological deterioration
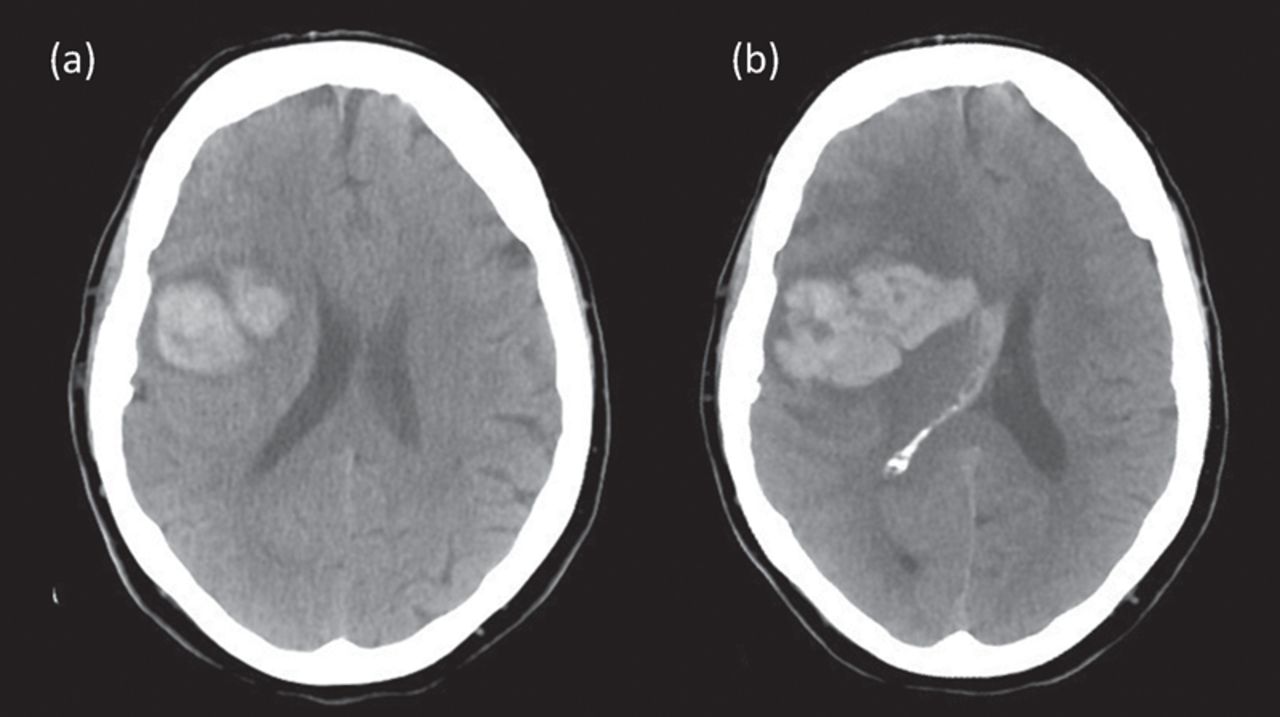
In ICH, a key pathophysiological difference from ischaemic stroke is the presence within the fixed volume of the cranium of a space-occupying lesion, initially composed of the haematoma and subsequently, an increasing volume of vasogenic oedema.4 Should the reserve of space within the cranium be exhausted (Monro-Kellie doctrine), intracranial pressure will begin to rise and fatal brain herniation syndromes may then occur. Baseline haematoma volume is an important predictor of survival and functional outcomes but subsequent early complications that increase intracranial pressure can cause early neurological deterioration in up to half of patients, depending on how it is defined and study duration.5,6 Haematoma expansion (Fig 1) is a principal cause of deterioration in the first 24 hours after onset, with studies indicating that up to 30% of patients demonstrate significant haematoma expansion within hours of onset, which worsens prognosis.7 Obstructive hydrocephalus may occur with occlusion of cerebrospinal fluid flow, either by occlusion of the ventricular system by intraventricular haemorrhage or extrinsic compression, especially at the third and fourth ventricles. Finally, for larger haematomas in the subacute phase, the addition of a significant component of perihaematomal oedema may also worsen prognosis.4 Management in the hyperacute phase is aimed at reducing the risk of (or treating) these common, early complications.

Computerised tomography brain scans from an acute intracerebral haemorrhage patient at presentation (a) and 12 hours later (b) that demonstrate early hematoma expansion.
Acute management
A minority of patients with ICH will be critically ill on presentation and standard procedures to stabilise such patients should be immediately instituted, ensuring a protected airway and adequate respiration and circulation. Following this, management should focus on identification and rapid reversal of anticoagulation, intensive lowering of blood pressure (BP) in eligible patients and referral of appropriate patients to neurosurgery to be considered for surgical intervention. Early recognition and treatment of complications, such as pneumonia and seizures, are important and patients should be monitored in an environment appropriate to their needs. There is clear evidence that patients with ICH benefit at least as much as ischaemic stroke patients from good stroke unit care,8 so all ICH patients should be admitted to an acute stroke unit as standard, unless critical care is required for airway management, respiratory support, measurement and management of intracranial pressure or other organ support.
Anticoagulants
Anticoagulant-associated ICH accounts for 10–20% of acute ICH admissions.9 While previously the great majority of these patients were taking vitamin K antagonists (such as warfarin), the picture has become more complex in recent years, with a growing proportion of patients presenting on the newer direct oral anticoagulant drugs (DOACs), including the direct thrombin inhibitor dabigatran and the factor Xa antagonists (apixaban, rivaroxaban and edoxaban). At our UK hyperacute stroke centre, 48% of anticoagulant-associated ICH occurred in patients taking a DOAC in 2016, while in the prior 2 years (2014–15) this figure was only 6% (unpublished audit data). Four-factor prothrombin complex concentrate (PCC) combined with vitamin K has been the standard reversal therapy for vitamin K-associated ICH for at least a decade in the UK, but recent randomised controlled trial evidence suggesting the superiority of PCC over fresh frozen plasma (FFP) in this setting has been provided by the INCH (International Normalized Ratio [INR] Normalization in Coumadin Associated Intracerebral Haemorrhage) trial.10 Although only small numbers were recruited (54 patients in total) the trial demonstrated a superior reduction in the INR to <1.3 by 3 hours with PCC (67%) versus FFP (9%). More haematoma growth was seen in FFP-treated patients between baseline and both 3 hours and 24 hours when compared with PCC-treated patients.10 Recent studies have further underlined the importance of rapid reversal of anticoagulation in ICH. A large multicentre observational study demonstrated a reduced odds of haematoma enlargement with reversal to INR levels <1.3 within 4 hours from admission, with the reduction in the odds of expansion being greater the sooner reversal treatment was given.11 We have demonstrated at our centre that door-to-needle times for commencement of PCC were halved by three key measures that included a stock of PCC being immediately available in the Emergency Department (ED), a point-of-care INR machine in the ED to avoid any wait for a result and an agreed protocol to allow discussion with the resident haematologist to be omitted in vitamin K-associated ICH.12
Observational evidence suggests that ICH on DOACs presents similarly to ICH on vitamin K antagonists with a similar risk of death.13 For patients on DOACs, options for reversal recommended in the Royal College of Physicians’ (RCP) stroke guideline include PCC for apixaban, rivoraoxaban and edoxaban and idarucizumab for dabigatran.14 Idarucizumab is a humanised monoclonal antibody fragment that binds to dabigatran with very high affinity, and offers rapid and complete reversal.15 There is some evidence for partial reversal of factor Xa antagonists with PCC in healthy volunteers16 and animal models17 and specific antidotes are being developed.18
Finally, there has been interest in administering platelets to patients with ICH taking antiplatelet drugs, but a recent randomised controlled trial (PATCH – Platelet transfusion in cerebral haemorrhage) has clearly shown that this is harmful and should no longer be considered in clinical practice.19
Intensive blood pressure lowering
INTERACT2 (Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial 2) was a large, randomised controlled trial of a management strategy of intensive BP lowering to a target of 130–140 mmHg within 1 hour of commencing treatment in ICH patients presenting with systolic BP >150 mmHg within 6 hours of symptom onset. This intervention was shown to reduce disability on a pre-specified ordinal shift analysis of the modified Rankin scale at 90 days; it improved quality of life measures and was shown to be safe, with no significant increase in adverse events.20 Investigators were free to use local protocols to achieve the BP targets and agents used included urapadil, calcium channel blockers, labetalol and nitroglycerin. The ATACH-II (Antihypertensive Treatment of Cerebral Hemorrhage II) trial was published 3 years later and compared a systolic BP target of 110–139 mmHg with 140–179 mmHg in 1,000 patients (treatment was with nicardipine). ATACH-II was neutral on all outcomes, with an increase in renal adverse events in the intensive treatment group. However, it is important to note that the ‘standard treatment’ group (target 140–179 mmHg) in ATACH-II had a BP profile compatible with even more intensive lowering that that seen in the ‘intensive’ group of INTERACT2. The ATACH-II standard group started out with a mean systolic BP of 201.1 (SD 26.9) mmHg, had it lowered to around 160 mmHg before randomisation, then had it lowered further to a mean of 141.1 mmHg within the first 2 hours, thus an average drop of around 60 mmHg in the first 6 hours. The INTERACT2 intensive arm went from 179 mmHg at baseline to 150 mmHg at 1 hour, so a drop of around 30 mmHg in the first 6 hours. The ATACH-II intensive group went from 200 mmHg pre-randomisation to around 156 mmHg at randomisation and then down to 128.9 mmHg at 2 hours. This represents a drop of over 70 mmHg, over twice that achieved in INTERACT2. Combining the two trials, one may interpret this as showing that the intervention tested in INTERACT2 should be recommended as it was safe and reduced disability, but more intensive lowering beyond this (as tested in ATACH-II) is of no overall benefit and may lead to renal adverse effects. The INTERACT2 intervention is therefore recommended in the latest RCP guidelines.14
Neurosurgery
Bleeding in the infratentorial compartment carries a high risk of brainstem compression, herniation syndromes and development of hydrocephalus, and therefore procedures such as posterior fossa decompression, external ventricular drain insertion and haematoma evacuation are offered by neurosurgeons, most often for haemorrhage within the cerebellum. For hydrocephalus from supratentorial ICH, treatment with external ventricular drain insertion may be offered. However, evidence so far has shown that additional clot lysis with thrombolytic agents reduces mortality without improving functional outcome so this intervention requires further investigation before it might be considered beneficial.21 An individual patient data meta-analysis of trials where early haematoma evacuation was tested for supratentorial ICH suggests certain patient characteristics may be associated with benefit from early haematoma evacuation, including age 50–70 years old, a Glasgow Coma Scale score of 9–12 or an ICH volume of 20–50 mL.22 Minimally invasive surgery with or without clot lysis is in late stage investigation. The MISTIE III (Minimally Invasive Surgery Plus Rt-PA for ICH Evacuation Phase III) trial is nearing completion and should report in 2019. The trial is testing whether minimally invasive catheter evacuation followed by thrombolysis for clot removal improves patient outcomes in a randomised trial of 500 patients (NCT01827046, ClinicalTrials.gov). The MISTIE phase II trial importantly showed no significant increase in symptomatic bleeding or infections in the surgical group and a trend towards improved functional outcomes with the surgical intervention.23 For now, only conventional surgery is offered in the UK and existing data can help to guide patient selection.
Implementation in UK practice
We have used quality improvement methodology at our hyperacute stroke unit (Salford Royal NHS Foundation Trust) in 2015–16 to consistently and effectively implement the evidence outlined above into practice. We used a care bundle approach with process targets for anticoagulant reversal, BP lowering and referral to neurosurgery and used the ‘Model for improvement’ to achieve these. This approach was associated with a significant reduction in 30-day case fatality for patients admitted after commencement of the care bundle from 35.3% to 25.3%, which was independent of case mix and national temporal trends (unpublished data). We are currently scaling up this approach across the whole centralised stroke pathway in our large urban area (Greater Manchester, UK).
Conclusions
Despite only representing 15% of all strokes, ICH is the most devastating stroke subtype with little improvement in outcomes in recent years. Studies have suggested benefit from prompt reversal of anticoagulation, intensive lowering of BP and surgical intervention in certain cases with the promise of further novel therapies in the near future. We have shown that effective implementation of this evidence as an acute care bundle may have a major impact on patient outcomes and further studies are warranted to robustly assess the clinical and cost effectiveness of this approach.
Conflicts of interest
The authors have no conflicts of interest to declare.
- © Royal College of Physicians 2018. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.