
Aetiology/pathophysiology/pathology
Hypertrophic cardiomyopathy (HCM) is defined by the presence of increased left ventricular (LV) wall thickness (for adults, >15 mm in one or more LV myocardial segments) that is not solely explained by abnormal loading conditions (eg hypertension).
Up to 60% of the cases are due to mutations in genes that encode sarcomeric proteins, such as the beta-myosin heavy chain, the myosin-binding protein C, troponin I and T (autosomal dominant). Five to ten per cent of the cases are due to other genetic disorders including inherited metabolic and neuromuscular diseases (eg Friedreich’s ataxia, amyloidosis and mitochondrial diseases). The degree and distribution of hypertrophy is very variable (eg septal, apical, mid-cavity). Depending upon the severity and extent of the hypertrophy, patients with HCM can develop LV outflow tract obstruction (LVOTO), diastolic dysfunction, myocardial ischaemia or mitral regurgitation.
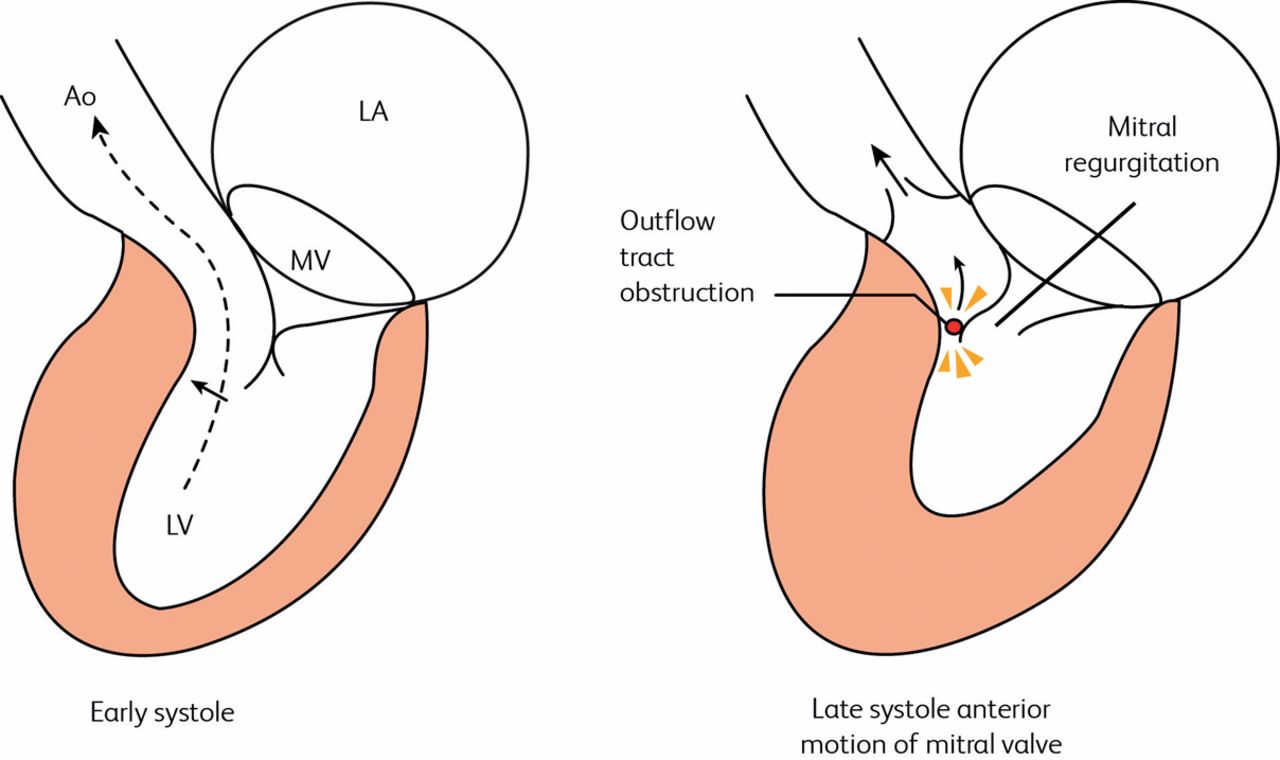
In the classic form of obstructive HCM, the obstruction occurs at the level of the LVOT by a combination of septal hypertrophy and systolic anterior movement of the anterior mitral valve (Fig 1) (Venturi effect due to the high velocities in the LVOT). In other morphologic variants of HCM, obstruction at the mid-cavity can also occur.

Effect of asymmetrical septal hypertrophy in HCM. In late systole the septum contracts down on the outflow tract, obstructing flow and generating a gradient. This generates a negative pressure (Venturi effect) just proximal to the obstruction, sucking the MV anteriorly (systolic anterior motion) and producing mitral regurgitation. Ao, aorta; LA, left atrium; LV, left ventricle; MV, mitral valve.
Epidemiology
The prevalence of hypertrophic cardiomyopathy (HCM) is one in 500 and it is the most common single-gene cardiac disorder.
Clinical presentation
Common
exertional chest pain and breathlessness
palpitations
asymptomatic murmur
abnormal ECG on screening
Uncommon
syncope
Rare
sudden death
Physical signs
There may be no abnormal findings.
Common
jerky pulse
prominent apical impulse
systolic murmur at left lower sternal edge/apex
Uncommon
fourth heart sound: often easier to feel (as a double apical impulse) than hear.
Investigations
The ECG and echocardiogram must be interpreted together because they provide complementary information.
ECG
The ECG is sensitive but not very specific. It varies from T wave inversion to overt left ventricular hypertrophy (LVH).
Echocardiography
Echocardiography is specific but less sensitive than the ECG. Classically, there is asymmetrical septal hypertrophy with systolic anterior motion of the mitral valve leaflet, LVOTO and secondary mitral regurgitation. Alternative patterns include apical, free wall or concentric LVH. LVOTO is defined as a peak instantaneous Doppler LVOT gradient of >30 mmHg, but the threshold for invasive treatment is usually >50 mmHg.
Ambulatory monitoring
This is used to identify the cause of palpitations or detect asymptomatic arrhythmia.
Exercise ECG
This is used to provoke arrhythmia and assess the BP response (important for prognosis or for vocational driving licence).
Magnetic resonance imaging
MRI may confirm the diagnosis if echocardiographic images are not clear (Fig 2).
Hazard
It is possible to have HCM without any hypertrophy. The diagnosis may be made on the family history plus an abnormal ECG.

MRI of the heart in the short axis, showing asymmetrical hypertrophy of the interventricular septum in HCM (indicated by arrow). LV, left ventricular cavity; RV, right ventricular cavity.
Differential diagnosis
Hypertensive cardiac hypertrophy: a concentric pattern of hypertrophy with documented hypertension.
Athlete’s heart: differentiation may be difficult because some highly trained athletes, especially weight-lifters, rowers and cyclists, have an identical pattern of physiological hypertrophy. However, this will regress if training is discontinued. A septal thickness of >1.6 cm is likely to be pathological.
Treatment
Patients with LVOTO
By consensus, symptomatic patients with LVOTO should be treated with non-vasodilating beta-blockers. If beta-blockers are not tolerated or ineffective, then disopyramide, verapamil or diltiazem can be used.
Low-dose loop or thiazide diuretics can be considered with caution to improve breathlessness but remember that avoiding hypovolaemia is very important.
Patients who remain symptomatic with LVOTO >50 mmHg, NYHA class III–IV and/or recurrent exertional syncope despite maximum tolerated medical therapy should be considered for invasive treatment. The main invasive methods for relieving LVOTO are surgical myomectomy or septal alcohol ablation.
Surgical septal myomectomy (Morrow procedure): a rectangular trough is created from the basal septum below the aortic valve until beyond the point of the mitral leaflet–septal contact. At the same time realignment of the papillary muscle or mitral valve repair can also happen. The mortality rate is 1–2%.
Septal alcohol ablation (Fig 3): a localised septal scar is created following selective injection of alcohol into a septal perforator artery. This relieves the LVOTO but potential issues with the papillary muscles or the mitral valve cannot be addressed. The mortality rate is similar to surgical myomectomy with the main complications being atrioventricular (AV) block (7–20%).

Septal ablation in hypertrophic obstructive cardiomyopathy. (a) A wire is passed through a coronary guide catheter into the target septal artery, indicated by arrow. A balloon catheter is passed, the wire is removed and the balloon inflated to occlude the artery. (b) Dye is injected down the lumen of the balloon catheter into the distal septal artery to confirm correct positioning. (c) Absolute alcohol is then injected to destroy selectively the septal artery, leaving a stump. Simultaneous pressure recordings reveal a left ventricular outflow tract gradient (peak ventricular minus peak aortic pressure) of approximately 100 mmHg (d) before the procedure, falling to (e) 15 mmHg afterwards.
Patients without LVOTO
The main therapy includes beta-blockers, verapamil or diltiazem to improve symptoms. Symptoms of heart failure should be treated according to standard guidelines. ACE inhibitors (ACEIs) and mineralocorticoid receptor antagonists are indicated if ejection fraction (EF) <50%.
All patients should be assessed for risk of sudden cardiac death (SCD) according to the HCM Risk-SCD calculator. The variables needed to assess the risk are: age, family history of SCD, unexplained syncope, LV outflow gradient, maximum LV wall thickness, left atrial diameter and non-sustained ventricular tachycardia (NSVT). The general advice is that:
implantable cardioverter defibrillator (ICD) is not indicated if the 5-year risk is <4%.
ICD may be considered if 5-year risk is 4–6%.
ICD should be considered if 5-year risk is >6%.
Complications
Common
Atrial fibrillation (AF): always anticoagulate because there is a high risk of thromboembolism. Do not use the CHA2DS2-VASc score as these patients were not included in the clinical trials. Patients with HCM and AF have high incidence of stroke and should be anticoagulated (in general lifelong, even if sinus rhythm has been restored). Atrial fibrillation (AF) is often poorly tolerated, so consider cardioversion along with antiarrhythmic drugs to maintain sinus rhythm. Note that digoxin is contraindicated if there is significant LV outflow tract (LVOT) gradient (>30 mmHg), so use a beta-blocker or calcium antagonist for rate control.
Uncommon
Ventricular tachycardia (VT): sustained VT is associated with high risk of sudden death and requires an implantable cardioverter defibrillator (ICD).
Progression to dilated cardiomyopathy: documented in up to 15% of early series, but certainly less common than this in modern practice.
Sudden death.
Rare
endocarditis.
Prognosis
Risk of premature death associated with the following:
cardiac arrest or sustained VT
syncope (especially when recurrent or associated with exertion)
strong family history of sudden early death
diagnosis of HCM in childhood
VT on 24-hour ECG monitoring
BP drop on exercise
presence of certain high-risk mutations
extreme LVH (>3 cm)
Disease associations
Friedreich’s ataxia and the Wolff–Parkinson–White syndrome.
Important information for patients
Occupational aspects
Patients should not be professionals in sports requiring vigorous physical exertion. They may still hold vocational driving licences if they meet the Driver and Vehicle Licensing Agency (DVLA – UK) criteria.
- © Royal College of Physicians 2019. All rights reserved.








{kind=link}
{kind=link}
{kind=link}