
ABSTRACT
A 5-year-old boy with an incidentally detected cardiac murmur was referred for evaluation. Tall R waves were noted in the electrocardiogram in leads V3 and V4. Transthoracic echocardiography suggested asymmetric septal hypertrophy with diffuse thickening of the inter-ventricular septum with normal thickness of the posterior left ventricular wall. Upon closer interrogation, a masquerading sessile cardiac mass was identified adherent to the left ventricular side of the inter-ventricular septum which appeared to contract with each cardiac cycle, mimicking hypertrophic cardiomyopathy.
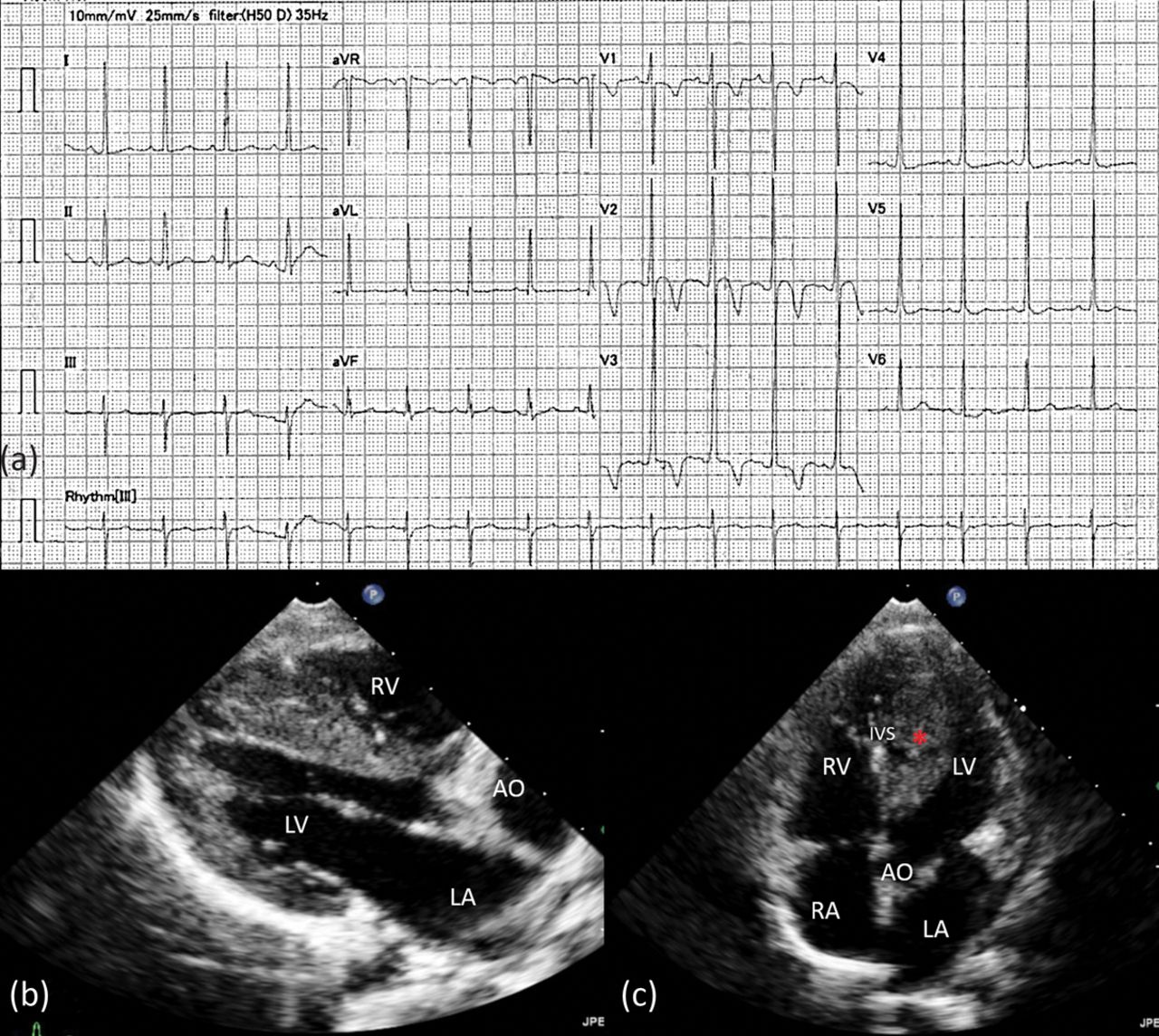
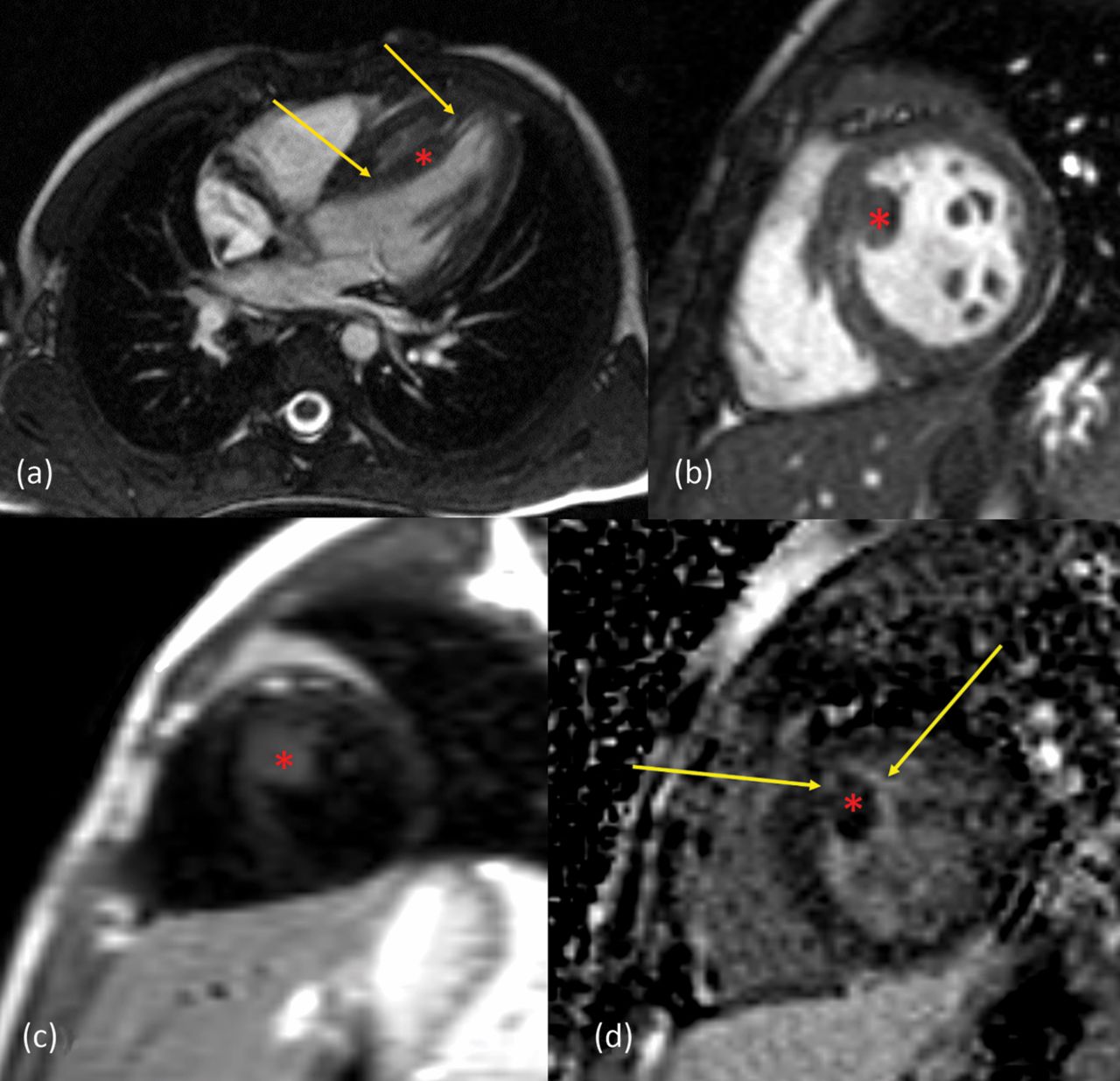
A 5-year-old boy was evaluated for an incidentally detected cardiac murmur during a dental check-up. 12-lead electrocardiogram showed tall R waves in V3 and V4 (Fig 1a). Transthoracic echocardiography suggested asymmetric septal hypertrophy with diffuse thickening of the inter-ventricular septum with normal thickness of the posterior left ventricular wall (Fig 1b-c). Upon closer interrogation, a masquerading sessile cardiac mass was identified adherent to the left ventricular side of the inter-ventricular septum which appeared to contract with each cardiac cycle. A clear plane of demarcation was identified from the inter-ventricular septum. The mass showed multiple short stalks of attachment to the septum at the apex and subaortic region. There was no inflow or outflow tract obstruction. Cardiac magnetic resonance imaging confirmed the exophytic lesion in the left ventricle, isointense on T1-imaging and mildly hyperintense on T2-weighted imaging (Fig 2). Delayed gadolinium enhancement sequences showed peripheral enhancement with gradual central enhancement suggesting a myxoma rather than a rhabdomyoma. The child was offered high-risk surgical excision after explaining the risks of incomplete excision and possible need for left ventriculotomy. However the parents preferred close medical follow-up, after explaining the risk of embolisation. There was no change in size or mobility of the mass till last follow-up at 6 months and the child remains asymptomatic.
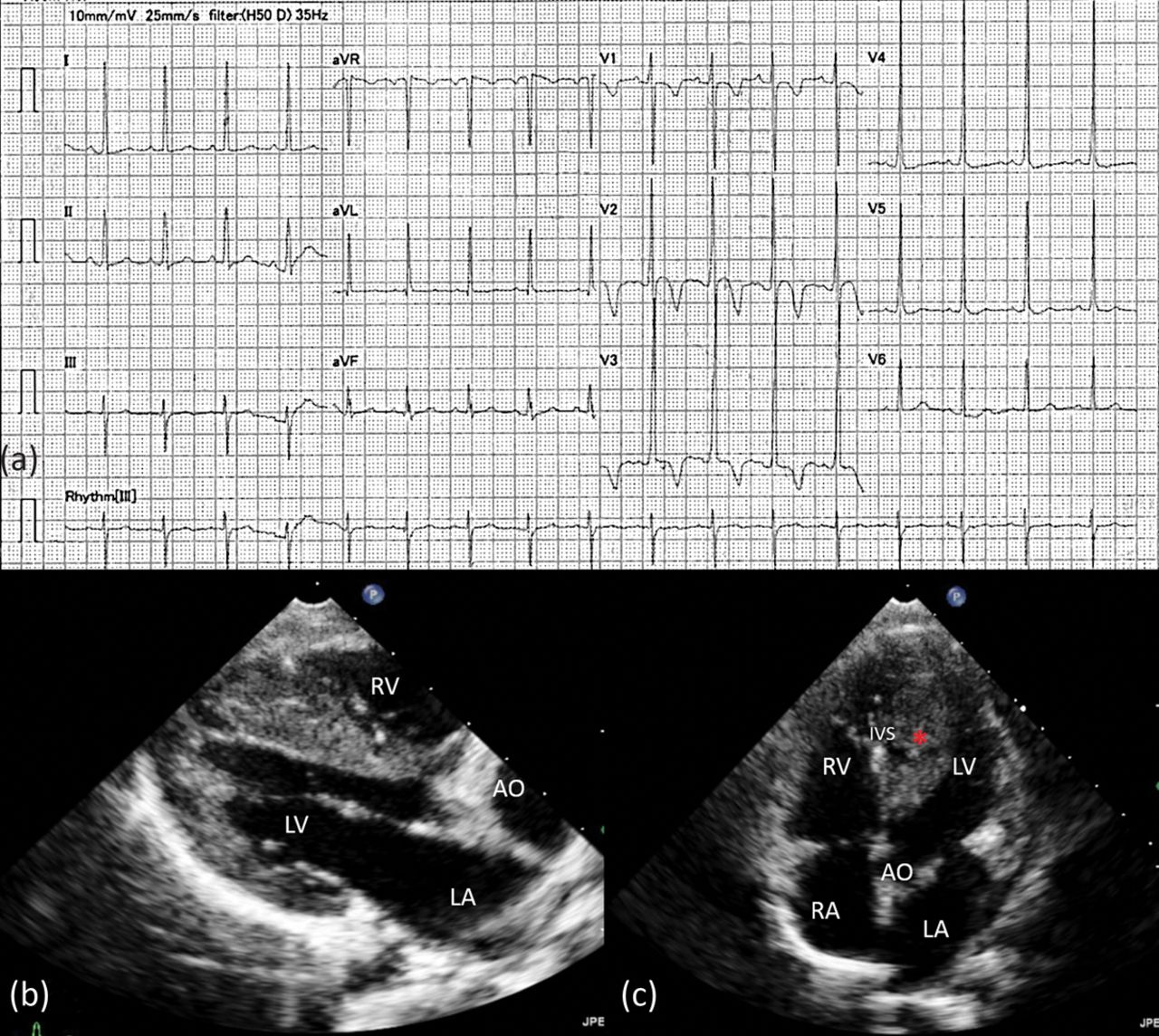
Electrocardiogram and transthoracic echocardiograms. Fig 1a is the 12-lead electrocardiogram of the patient showing sinus rhythm, normal PR interval and QRS axis but tall R waves in V3, V4. Borderline LVH is evident. Fig 1b is the transthoracic echocardiographic still frame in diastole from the parasternal long-axis projection suggesting asymmetric septal hypertrophy. The ventricular myxoma (red asterisk) is inconspicuous in this view. Fig 1c is the transthoracic echocardiographic still frame in diastole from the apical five-chamber projection showing a small plane of demarcation between the ventricular myxoma and the inter-ventricular septum differentiating the tumour from asymmetric ventricular hypertrophy.
AO = aorta; IVS = inter-ventricular septum; LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle.

Cardiac magnetic resonance imaging (MRI) images of the patient. Fig 2a is the axial section showing the cardiac mass (red asterisk) with stalks of attachment (arrows) mimicking septal hypertrophy. Fig 2b is the T1-weighted short axis MRI still image showing that the mass is isointense with the myocardium. Fig 2c shows that the mass is hyperintense on T2-weighted imaging. Fig 2d is the late gadolinium sequence of the MRI showing peripheral tumour enhancement (arrows) and mild central enhancement.
The relevance of meticulous evaluation cannot be overemphasised during clinical examination and echocardiography. Sessile left ventricular myxomas are unusual and can pose diagnostic challenges, as in the index case. The risks of incomplete excision and possible tumour recurrence need to be weighed against the risk of embolisation with medical management.
- © Royal College of Physicians 2019. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.