
ABSTRACT
Significant uncertainty surrounds the sustainability of healthcare services in which junior doctors work. It is essential that student and foundation doctors (SFDs) are actively engaged if workforce morale is rebuilt. This narrative review explores the evidence driving the individual work-streams of the Royal College of Physicians’ newly formed Student and Foundation Doctor Network. Undergraduate and postgraduate training reform has coincided with concerning feedback from newly qualified doctors. System-level efforts to address this include a focus on extra-contractual matters, where small, sustainable changes could address training and work issues.
Fewer foundation year-2 doctors are entering specialty training immediately after the foundation programme. Providing dedicated careers guidance and highlighting opportunities within traditional placements and other career paths can support doctors who undertake non-traditional career routes, including those who take time out of programme.
Disseminating these resources through an effective peer-to-peer framework and a well-established mentoring scheme could be the most appropriate way to spread good practice.
Introduction
In April 2016, the NHS in England endured the first all-out ‘junior doctor’ strikes (encompassing both elective and emergency services) in its history.1 While contractual negotiations sparked the decision to ballot junior doctors, pre-existing and longstanding problems with junior doctor morale exacerbated the dispute.2 This distinction is particularly pertinent given that the terms and conditions of service for junior doctors in England is currently being reviewed by the British Medical Association and NHS Employers.3
Undergraduate medical education in the UK is between 4 to 6 years in length. Prior to specialty training, UK medical graduates also complete a 2-year Foundation Programme (FP) that rotates trainees through placements, delivering a broad curriculum predominantly through experiential learning. While this period cements trainees’ continuing postgraduate development, these doctors represent the foundations of the profession's future.
With uncertainty around what their future professional working lives in the NHS will resemble, student and foundation doctors (SFDs) may feel justified in considering their commitment to a long-term career in healthcare. It is imperative that they are actively engaged and consulted if morale is to be rebuilt and whatever ‘fractures the relationship between physicians and the state’ is to be addressed.1
Recently the Royal College of Physicians (RCP) established its Student and Foundation Doctor Network (SFDN). Representatives from across the UK meet regularly to discuss pressing issues affecting SFDs and how the RCP could address them. There are three work-streams: working lives, to survey the challenges within the foundations of junior doctor morale; careers development, to shore up these foundations; and local engagement and communication, to strengthen them for the future.
In this narrative review, we explore the evidence behind these goals. The review will explore recent reforms, successful solutions employed locally or in other sectors. We also illustrate the value SFDs can provide to policy by outlining a SFDN project.
SFDs’ working lives
The past 15 years have seen major reforms to undergraduate and postgraduate training, including Modernising medical careers (MMC) which saw changes to specialty registrar training, first year of medical practice (pre-registration house officer) and the senior house officer system.4 The latter two changes resulted in the genesis of the FP (Table 1).
Examples of challenges of previous pre-registration house officer and senior house officer grades with relevant changes included in the Foundation Programme to address these.
Critics argue that MMC has resulted in a more inflexible training structure which contributes to trainee attrition. Many also argue that it has resulted in the weakening of informal support networks through the loss of the firm and diminishing use of the mess.6 Solutions to address this have been varied and have included placing some postgraduate responsibilities on medical schools.7 Similarly, the Shape of Training review and a subsequent General Medical Council (GMC) report draw attention to the effect of recent reforms on trainee experience, training quality and workforce retention.8–10
Undergraduate curricula and its delivery have also been progressively modified in line with sequential GMC guidance – from ‘Tomorrow's doctors’ to Promoting excellence: standards for medical education and training.11,12 Most notably, practical skills training has shifted from a ‘see one, do one’ format to initial simulation and/or clinical skills laboratory training followed by competency-evidenced skill practice. This, in part, reflects changing sector-wide approaches to safety.13
However, these reforms have coincided with concerning feedback. The GMC surveys cite that reported preparedness for practice of new doctors rose from 26% in 1999 to 58% in 2005. After the introduction of the FP, improvements stagnated, with only 49% of 2009 graduates feeling that medical school had adequately prepared them for practice. A more in-depth study found further evidence of poor self-reported preparedness. Graduates, in addition to supervisors, reported that up to 28.3% of foundation doctors (FDs) failed to cope with the transition from medical school.14 Trainers also have concerns regarding graduates’ competence in several areas, including prescribing, interpersonal skills, and diagnosis and management of acutely unwell patients.15 The newly introduced burnout questions within the GMC's national training survey 2018 reveal that FDs report the highest work intensity and feelings of burnout along with feeling that they were on a ‘training treadmill’ of continuous ‘tick box’ assessments.16
This highlights the difficulty of the sharp transition from medical student to practising physician with frequent rota gaps and often scarce senior availability.17 These findings also demonstrate that training reforms often fail to take a holistic view of the pressures experienced by FDs, with recent reports identifying that these are linked to worsening workforce retention.9,10 Curricula and programme design would be enriched by a greater awareness of these pressures, some of which are outlined in Table 2.
Current challenges to the wellbeing and morale of student and foundation doctors
Recent system-level efforts to address these challenges include the 2016 terms and conditions of service in England and the ongoing FP review.42 Key stipulations, including improved limits on safe working hours, a system to report deviations from planned rostering arrangements as well as the creation of the ‘guardian of safe working hours’ role, are designed to address issues surrounding overtime and missed breaks.
Provision of hot and cold sustenance and facilitating rest breaks for doctors on long shifts are examples of the eight high-impact actions published by NHS Improvement, recommended as enhancements to the working environments of junior doctors in line with the widespread recognition of the benefits of such provisions in other sectors.43
Recognising these challenges and the efforts to address them, the SFDN established a working lives work-stream focusing on extra-contractual matters, where small, sustainable changes could address training and work issues. The work-streams’ activities have all been mapped to documented issues that SFDs face, solutions for each of which are supported by evidence and/or membership feedback. These are outlined in Table 2.
SFD career development
Only 37.7% of foundation year-2 doctors who completed their FP in 2018 immediately commenced specialty training; down from 66% in 2012.44 Reflecting this, unfilled vacancies increased by 31% since 2016.45 This trend results in increasing NHS agency staff spend and risks providers’ ability to provide sustainable, good-quality care.
Discussions with FDs have revealed that the likely reasons to delay formal training include gaining experience in different specialties and overseas healthcare systems, and acquiring qualifications not possible in structured training programmes. Interestingly, FDs also placed importance on developing ‘soft’ skills such as time management and networking, as well as being able to pursue elements of a portfolio career which they felt enabled to do outside training.10
FDs are typically expected to apply for specialty training programmes shortly after beginning their second year of postgraduate training, often not experiencing their specialty of interest due to limited control over rotation selections. In order to demonstrate commitment to a highly competitive specialty, trainees must plan their application and tailor their curriculum vitae (CV) years in advance. This can result in significant time and financial pressures at a career stage where financial resources are already limited.
Contributing to this issue is the fear of significant difficulties induced by choosing the ‘wrong’ specialty, and eventually needing to switch training programme via a system that does not comprehensively recognise transferrable skills.9 This is heightened by an increasing rigidity in medical career paths, new contractual terms in England decreasing the potential to receive pay-protection, and the disadvantage that may face candidates with a CV focused on a different specialty. This is also an issue which the GMC is attempting to resolve.9,46
To address these issues, the SFDN established a careers development stream to compile resources to facilitate informed career decisions for SFDs.
This includes ‘How to…’ guides to plan electives – an undergraduate placement, often abroad, with the aim of giving students a different experience of medical practice from their medical school; and ‘taster weeks’ – short postgraduate placements offering insight into specialties outside of an FD's allocated rotations. Further guides will focus on topics often not formally taught at medical school, such as conference presentations, peer-reviewed research and undertaking quality improvement projects. These resources are aimed to help SFDs to realise their professional and personal goals while contributing to a system-wide effort to tackle unfilled vacancies.
Year-out-of-training: more than a ‘gap year’
A major contributor to NHS service provision, the insight that FDs provide goes beyond morale and career issues. One of the SFDN's focuses is to address a growing workforce challenge – FDs taking time out of training (TOT), often informally named an ‘F3 year’.
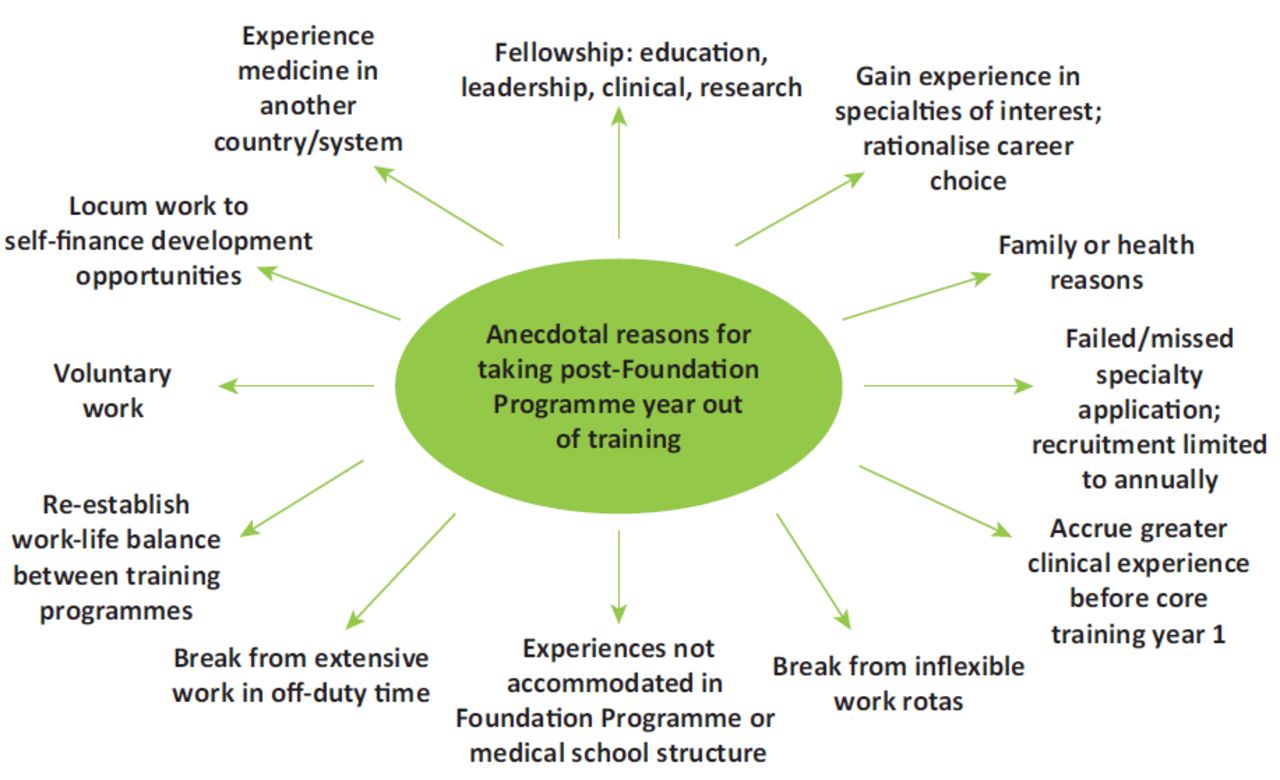
The number of FDs taking TOT increases year upon year. At present, the majority of these FDs eventually return to take up specialty training posts in the UK.47,48 There is little research-based evidence to explain the underlying reasons for this, but theorised reasons are outlined in Fig 1.8,10,47,49 The richest source of data thus far highlights three broad groups of motivating factors for deciding on a TOT/F3 year; health and wellbeing, specialty and future career, and training environment dissatisfaction.10

Proposed underlying reasons for foundation doctors to take a year out of training.
Junior doctors highlighted lack of autonomy, inability to explore future specialty careers, a need to develop non-technical skills and qualifications they felt unable to do in a formal training programme as additional driving forces for taking TOT.50
A recent Scotland-wide survey of FDs examined factors that affected the likelihood of FDs pursuing an F3 year. This study identified five factors that influenced the decision to continue to further formal training:
geographical location
supportive working and learning environment
good working conditions
opportunities for professional development
familiarity with specialty.
Potential earnings did not affect the decision to continue formal training; however, quality of professional development opportunities was a significant factor. FDs who opted for an F3 year placed greater weight on supportive culture and good working conditions than those who applied for further training.51
In the interests of workforce planning, it is imperative to examine how the NHS can utilise TOT doctors and facilitate their return to training as well as how to enhance the development of these doctors.52
As outlined in Fig 1, many motivations for TOT are pastoral. Enabling these doctors to return to training with enhanced skills and broader experience upskills the workforce and reduces future deficits in middle grade and senior rotas while preventing additional delays in training progression.
More than half of post-FP doctors chose to undertake TOT. Over 90% return to UK training within 3 years.50,52 More guidance and advice to enhance the developmental value of this time is in the interests of both FDs and the NHS.10
Through signposting and tailored guidance, the SFDN can support easier access to personal and professional development opportunities which are not possible while in full-time training such as research or education qualifications and fellowships, leadership roles or developing new clinical competencies (eg ECHO qualifications). This would allow FDs to pursue professionally enriching experiences without detriment.
In acknowledgement of this, the SFDN is working to address some of these key issues. Actions and outputs include:
case studies of previous F3 experiences to reflect the diverse possibilities available, particularly valuable to doctors who undertake TOT for pastoral reasons
guidance for how an F3 year can enhance a doctor's portfolio and illustrate how these experiences benefit the health service on return to training
advice on planning an F3 year that incorporates personal and professional development, including the appraisal process.10
The SFDN will highlight the unmet needs of these doctors, open discussions about the professional development of doctors who undertake TOT and provide informative, accessible resources. This project should make a tangible and directed difference to those FDs aspiring to improve their experience and development through an F3 year.
Local engagement and communication with SFDs
There is growing evidence of how different teaching methods are more appropriate for different learning requirements.53 To help improve the influence of the SFDN's work and engage SFDs with the RCP's services, activities and work, the local engagement and communications work-stream will be drawing on this evidence pool to deliver its content to members.
Outside the clinical settings, most notably through Schwartz rounds and action learning sets, sharing of ideas and learning with each other in a safe environment helps address the non-clinical demands of working and studying in the NHS, such as emotional and social stress.54 As discussed earlier, these elements of medical practice are often overlooked despite being a significant contribution to poor morale and burn-out.
Previously, SFDs relied on word of mouth within a close-knit medical firm for extra-contractual and non-clinical information. With the loss of firm-based working, junior colleagues are now more likely to seek advice from unverified online sources. Even with advances in information sharing, reputable, evidence-based answers to key questions are challenging to locate. Historically, the royal colleges have provided professional guidance and the SFDN will offer a natural extension of that role by signposting SFDs to credible relevant resources.55
Original content is written by current SFDs using a peer-to-peer framework, a model with a burgeoning amount of evidence, particularly for topics within the ‘unwritten curriculum’.56 Near-peer and peer-to-peer training supports both engagement and promotion of effective learning.57–59 Peers and near-peers have had recent experience of the challenging situations and aspects of training so can offer realistic advice, without the conflict of being involved in the SFDs’ assessments.
As these services are joined by others provided by the SFDN, the value of a dedicated local engagement and communications work-stream will continue to increase. Integrating this from the outset of the network's activities ensures a clear strategy on both the production and dissemination of resources for SFDN members.
Conclusion
SFDs are faced with an increasing number of challenges across domains including training, career progression and morale. Many of these are based on long-standing problems although some have been exacerbated by recent trends within healthcare and wider society.
As the group that will face the greatest impact from future training and healthcare reforms, it is important that SFDs are involved as partners in future change and that their unique insights are integrated as part of holistic solutions. Furthermore, as a major component of current and future NHS service provision, it is imperative that measures to improve their engagement, morale and retention within the NHS are considered seriously and given sufficient resources.
Multiple bodies already have dedicated groups for addressing SFD issues. However, recent junior doctor industrial action has shown that the royal colleges can play a different role in brokering constructive solutions to workforce problems. As part of the RCP, the SFDN with dedicated work-streams for working lives, career development and local engagement and communication can offer positive, informed solutions.
- © Royal College of Physicians 2019. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.