
Abstract
Introduction Mortality from chronic kidney disease (CKD) is increasing. Most patients die from cardiovascular disease and management of cardiovascular risks is key to prevent both mortality and progression to end-stage renal disease. In 2014, the National Institute of Health and Care Excellence (NICE) introduced guidance to help general practitioners (GPs) manage CKD patients.
Aim We aimed to determine the impact of the updated CKD guidance on CKD/cardiovascular risks optimisation and the timeliness of referral from the primary care.
Methods All new GP referrals to the Regional Renal Service in 2012 and 2016 were analysed. Data were collected on patient age, estimated glomerular filtration rate (eGFR) at referral, blood pressure (BP), smoking, body mass index, glycated haemoglobin (HbA1c; in diabetic patients) and lipid assessment.
Results A total of 486 new GP referrals were received in 2012, and 574 in 2016 (18% increase post NICE CKD guideline). Post NICE, fewer stage 4 and 5 CKD patients were being referred. But late referrals (eGFR <20 mL/min/1.73 m2) were not improved. BP control had improved. More patients had cholesterol-levels checked. The number of smokers and obese patients had not improved.
Conclusion Post NICE guidelines, GPs are better in optimising BP. Diabetes management and lifestyle modifications need further improvement.
Introduction
Mortality from chronic kidney disease (CKD) is increasing worldwide and is currently ranked 14th commonest cause of death.1 Management of cardiovascular risk in CKD patients is the key to prevent both death and decline of renal function to the point of end-stage renal disease (ESRD). In the UK, 14% of men and 13% women have CKD, the majority being managed in primary care. In 2014, the National Institute for Health and Care Excellence (NICE) introduced guidance to help general practitioners (GPs) manage patients with CKD, focusing on cardiovascular risk and prevention of late referral of patients likely to require renal replacement therapy.2
The study was aimed at determining the impact of the updated CKD guidance on CKD/cardiovascular risk optimisation and the timeliness of CKD referrals from the primary care.
Methods
All new GP referrals to the Regional Renal Service in 2012 and again in 2016, 2 years after the introduction of NICE CKD guidance in 2014, were analysed. Data were collected on patient age, CKD stage and estimated glomerular filtration rate (eGFR) at referral, renal imaging pre-referral, blood pressure (BP), smoking, body mass index (BMI), glycated haemoglobin (HbA1c; in diabetic patients) and lipid assessment.
Results
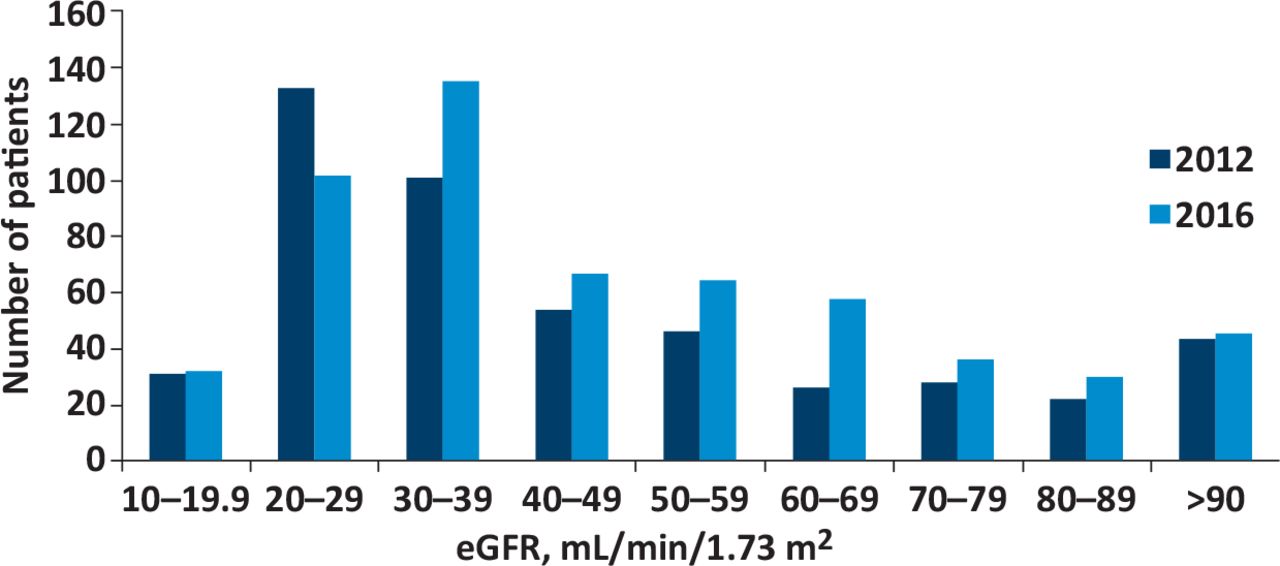
A total of 486 new GP referrals were received in 2012, compared with 574 in 2016. Data completion was 100% for renal imaging pre-referral, BP, BMI, diabetic status and lipid assessment at referral. Nearly one-third of referrals in 2012 (29.01%) and one-quarter in 2016 (24.39%) were aged >80 years (see Fig 1). The distribution of eGFR of the referred patients is shown in Fig 2. Two patients in both cohorts did not have eGFR/renal stage assessments due to age (<18 years), and one patient in the 2016 cohort refused blood testing.
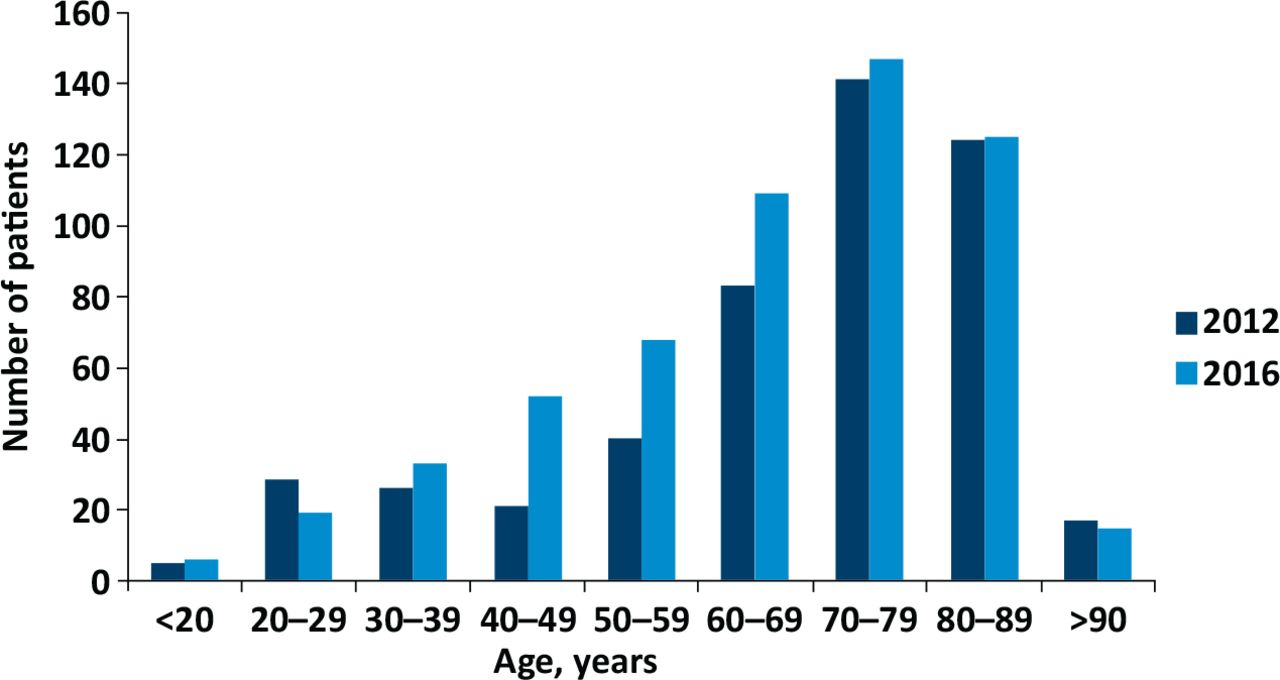
Distribution of new patients referred to renal clinic from general practitioners based on age before and after the introduction of National Institute of Health and Care Excellence guidelines CG182.

Distribution of referred patients based on estimated glomerular filtration rate at the time of referral before and after the introduction of National Institute of Health and Care Excellence guidelines CG182. eGFR = estimated glomerular filtration rate.
In 2012, 27.8% and in 2016, 30.7% of referrals were diabetic. Of the patients with diabetes, 60/134 (44.8%) in 2012, and 82/176 (46.6%) in 2016 had HbA1c of greater than 58 mmol/mol. With 11/134 (8.2%) of diabetic patients in 2012, and 13/176 (7.4%) diabetic patients in 2016 having HbA1c greater than 86 mmol/mol. HbA1c was not measured in one of the 2012 diabetic patients.
In 2012, 167 patients had a systolic blood pressure (SBP) less than 140 mmHg compared with 245 in 2016. 402/486 (82.7%) patients referred in 2012 and 509/573 (88.8%) patients referred in 2016 had cholesterol levels checked. Of those tested, 14.9% patients in 2012 and 15.9% in 2016 had a serum total cholesterol of 6.3 mmol/L or greater.
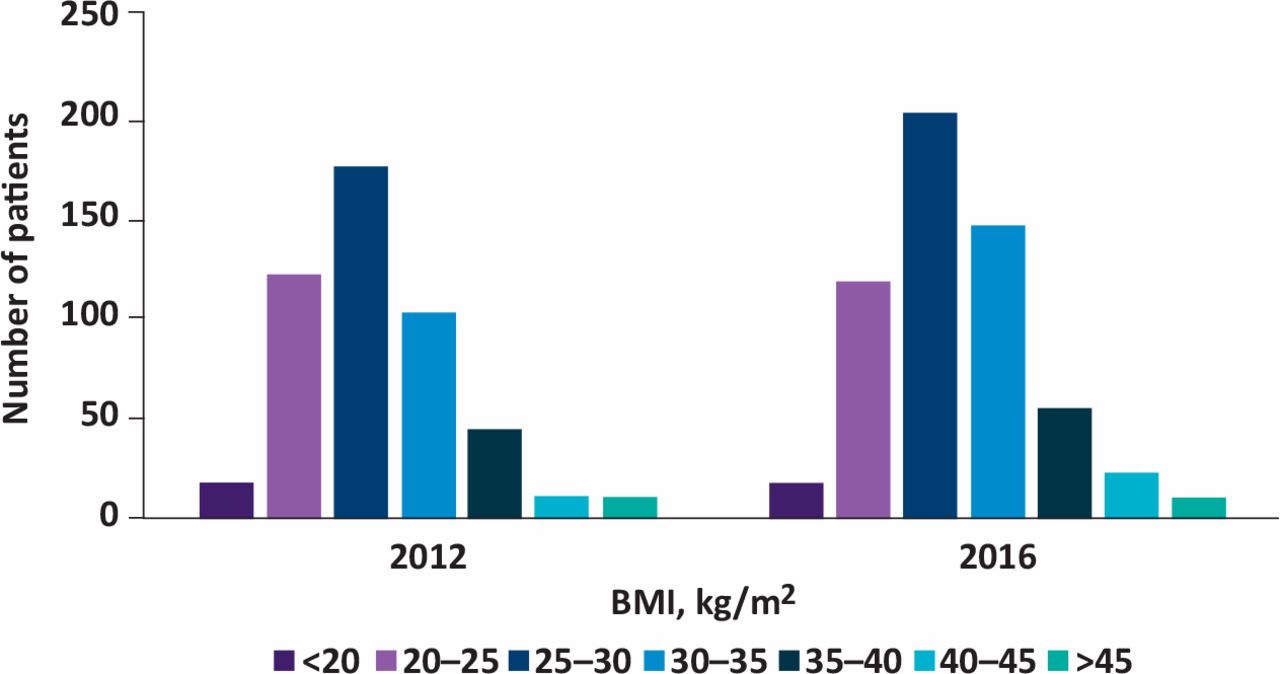
The proportion of obese patients referred is shown in Fig 3. In 2012, 11.7% and in 2016, 12.6% of referred patients were current smokers at the time of referral. Pre-referral, renal ultrasound was done only in 206/438 patients in 2012 and 252/529 patients in 2016; renal imaging was not required from 48 in 2012 and 45 in 2016.
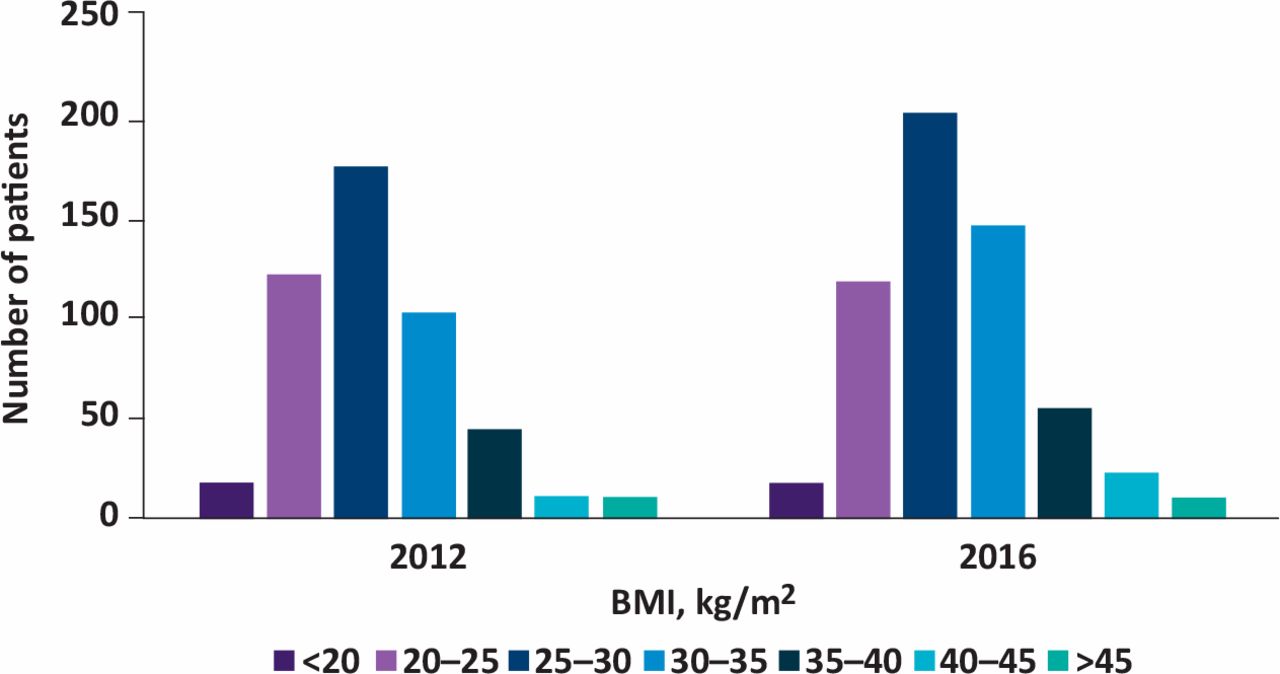
Distribution of patients based on body mass index before and after the introduction of National Institute of Health and Care Excellence guidelines CG182. BMI = body mass index.
The change in the proportion of cardiovascular risk factors post NICE guidelines is shown in Table 1. Post NICE guidelines, there has been an 18% increase in GP referrals. The number of smokers and obese patients in the referred population have not changed. Comparatively, a lesser proportion of patients had SBP >140 mmHg and significantly fewer patients had diastolic BP >90 mmHg post NICE guidance. Significantly more patients have had cholesterol levels checked (p=0.004). Post NICE guidelines, although significantly fewer stage 4 and 5 CKD patients are being referred (p<0.001), there is no statistically significant improvement in late CKD referrals (eGFR <20 mL/min/1.73m2, p=0.272)
Comparison of cardiovascular risk factors in general practitioner referred patients before and after the introduction of National Institute of Health and Care Excellence guidelines CG182
Discussion
CKD is associated with an increased risk of cardiovascular disease and related mortality.3,4 Impaired kidney function and raised concentrations of albumin in urine also increase the risk of cardiovascular disease by two to four times and are independent predictors of mortality risk.5,6 Stroke risk also increases linearly and additively with declining GFR and increasing albuminuria.7
The prevalence of CKD stages 3–5 increases with age, especially in those above 80 years of age.8 Among patients of all ages, there is an inverse association between eGFR and the proportion of deaths from a cardiovascular cause.5,7 However, among those with comparable levels of eGFR, older patients are more likely to die than reaching ESRD requiring renal replacement therapy.9
High BMI is a common, strong, potentially modifiable and independent risk factor for CKD progression and death.10,11 A meta-analysis concluded from smaller, short-duration studies in patients with CKD that nonsurgical weight loss interventions reduce proteinuria and BP and seem to prevent further decline in renal function.12
Poorly controlled diabetes is associated with greater risk of microvascular complications in both type 1 and type 2 diabetics.13,14 Diabetes is now the most common cause of ESRD in developed countries and diabetic patients are more likely to require dialysis and less likely to be transplanted.15
Hypertension is a well-established risk factor for cardiovascular disease (CVD) and a major promoter of CKD progression in both diabetic and nondiabetic kidney disease.16,17 The reduction in BP significantly reduces the risk of death and cardiovascular disease in general population18–21 and is markedly reno-protective in CKD population, regardless of the type of drug administered.22–25 NICE recommends aiming a systolic BP of less than 140 mmHg in CKD patients and less than 130 mmHg in CKD patients with diabetes and/or proteinuria.
Reduction of low-density lipoprotein, cholesterol, with medications safely reduces the incidence of major atherosclerotic events in patients with less advanced chronic kidney disease.26
Risk of death is higher in CKD patients who are current smokers compared with non-smokers and the risk increases with increase in number of daily cigarettes.27
Conclusion
In this single centre audit of new GP referrals to the renal outpatient department, the impact of NICE CKD guidance published in 2014 was better control of BP pre-referral, and increased testing of lipid levels. There was a worrying trend towards increased prevalence of diabetes and increased patient obesity. Managing obesity and smoking as risk factors for the development of renal disease remain challenging for both GPs and renal physicians.
- © 2019 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.