
Introduction
Risk scoring for acute upper gastrointestinal bleeding (AUGIB) is key when assessing patients for requiring oesophagogastroduodenoscopy (OGD). The Rockall score utilises age, comorbidities and shock. The Glasgow-Blatchford score (GBS), in addition, utilises haemoglobin, melaena and blood urea levels.
Raised blood urea levels can represent digestion of blood from the upper gastrointestinal tract giving rise to melaena; the presence of both gives a high GBS. However, inexperienced healthcare professionals can misinterpret the absence/presence of melaena, raised urea levels may be due to kidney injury. Nevertheless, gastroenterologists may use urea to diagnose AUGIB if patients haven't had overt/witnessed/reliably reported haematemesis or melaena.
It has been shown that a raised urea:creatinine ratio (URCR) can be associated with AUGIB and may be superior to urea alone as it mitigates for kidney injury.1 However, URCR is not widely used in the UK in the assessment of AUGIB. We aim to assess the association of urea and URCR levels with AUGIB.
Methods
A retrospective review at three UK centres (Kettering General Hospital, Queen Elizabeth Hospital Birmingham and University Hospital Coventry & Warwickshire) was undertaken. Endoscopy reports and blood tests were reviewed of patients undergoing inpatient OGD for suspected AUGIB within 2017/8; data were recorded in an Excel spreadsheet. URCR was calculated by dividing urea by creatinine, and multiplying by 1,000 (abnormal ≥100). Statistics were analysed using SPSS.
Results and discussion
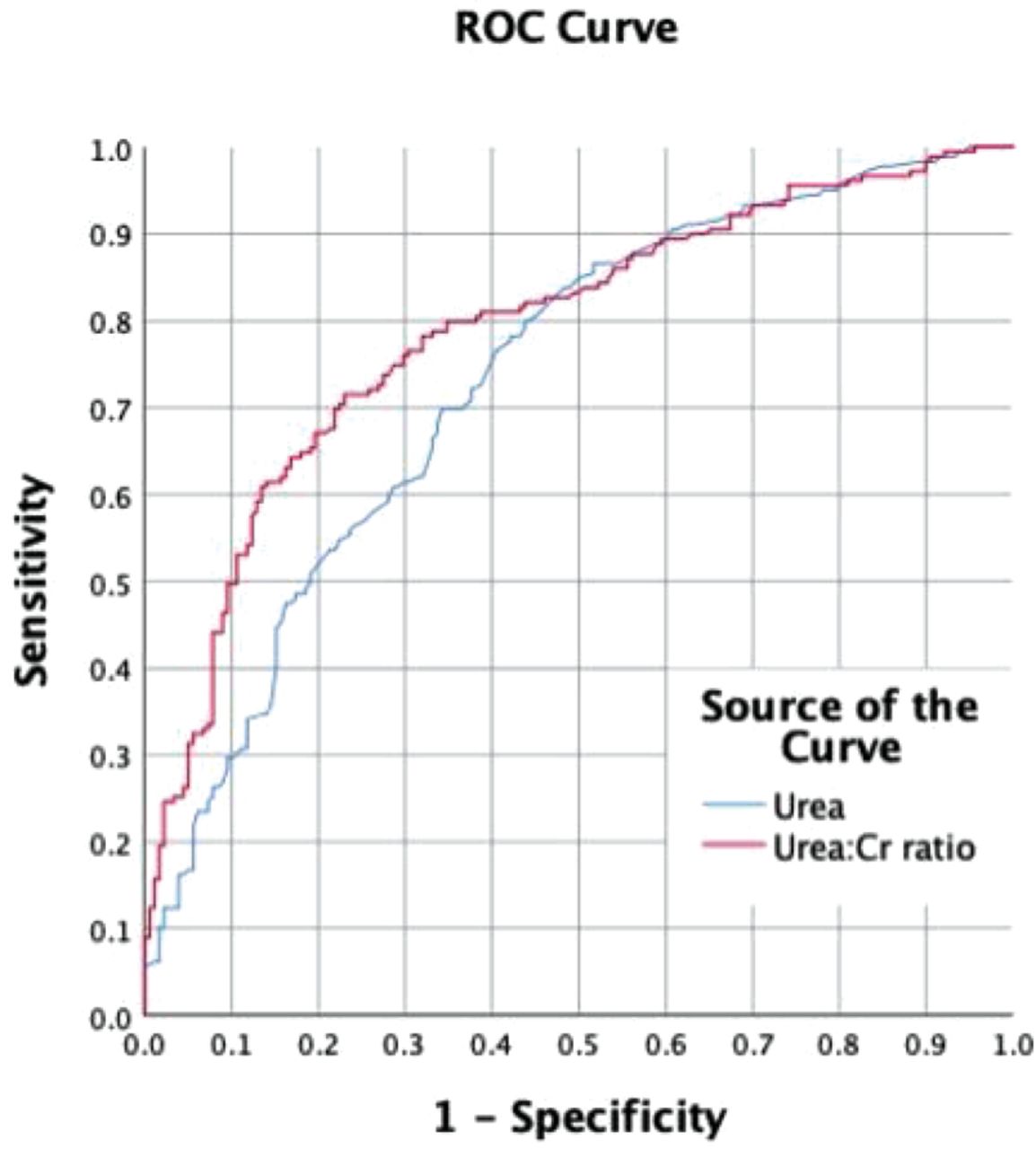
Three-hundred and fifty-seven patient records were reviewed (median age, 68); 179 had a plausible AUGIB (50.1%). Receiver operator characteristic (ROC) curves for urea gave an area under the curve (AUC) of 0.733. For URCR, AUC was 0.789 (Fig 1).
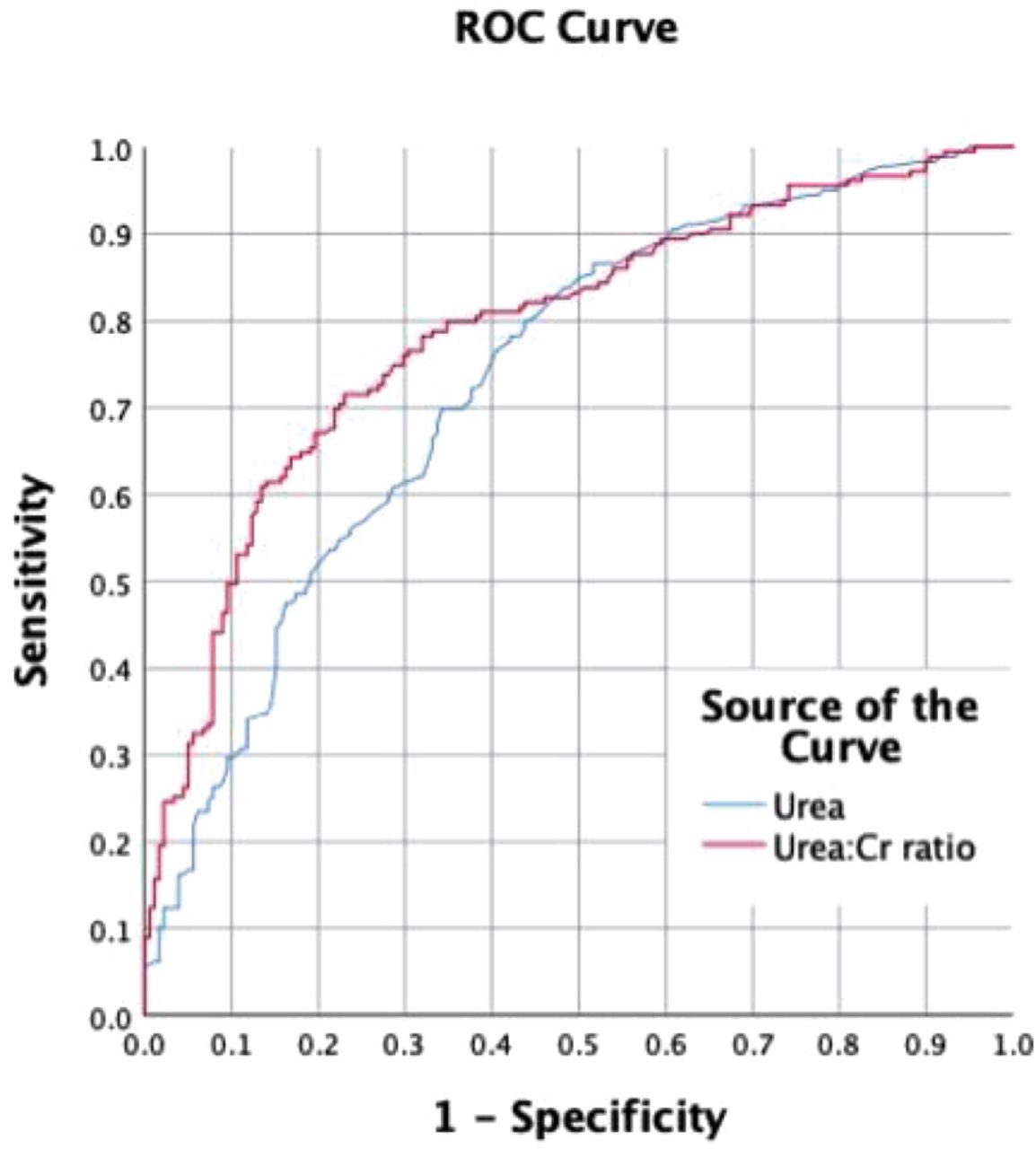
ROC curve
Binary logistic regression modelling was performed using age, urea and URCR. χ2 (3, n=357) = 102.92, p<0.001. 25–34% of the variance in AUGIB is explained by the model.
The model URCR value of 97.7 can be used to predict AUGIB, applying this to our data set correctly identifies 124/179 patients with AUGIB (69.3%), and is predicted to correctly identify 74.5%.
Conclusion
This pilot study has limitations as bleeding lesions may have not been identified at OGD. Urea and URCR have AUCs of 0.733 and 0.789. Logistic regression modelling suggests a URCR level of 100 would correctly identify ∼70% of AUGIB in patients with suggestive symptoms. Outside of firm indications for OGD in suspected AUGIB (shock, previous/suspected variceal bleed), a raised URCR appears to be a useful marker to predict AUGIB: a larger study would be able to test this robustly.
Conflict of interest statement
None declared.
- © Royal College of Physicians 2019. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.