
Introduction
Secondary prevention medications following ST-elevation myocardial infarction (STEMI) have been established with NICE and European Society of Cardiology guidelines.1,2 In practice, while most patients with STEMI are discharged with the correct secondary prevention medications,3 titration advice to primary care physicians can be lacking and the dosage of ACE inhibitor and beta blocker at discharge may be subtherapeutic.4
Medication titration is essential post-MI to prevent future cardiac events. Prognostic benefits have largely been shown in studies which used these medications in high doses.4-6 As such, NICE1 gives a five-point guideline on the information to be included in every discharge summary.
We set up a three Plan, Do, Study, Act (PDSA) cycle quality improvement project in Lancashire Cardiac Centre by using a combination of education and a new unified STEMI discharge letter form.
Materials and methods
Data was collected from the coronary care unit (CCU) STEMI primary percutaneous coronary intervention (PPCI) list, with the following inclusion criteria:
Admitted through PPCI pathway
Confirmed STEMI on discharge
Admission <5 days
Discharged alive
Discharge summaries of patients within the inclusion criteria were reviewed. For the purpose of this QIP, a correct discharge of STEMI patient following PPCI included the following:
Beta blocker including dose and dose titration advice
ACEi/ARB including dose and dose titration advice
Aldosterone antagonist – where clinically appropriate
Statin – unless contraindicated
Dual antiplatelet therapy (DAPT)
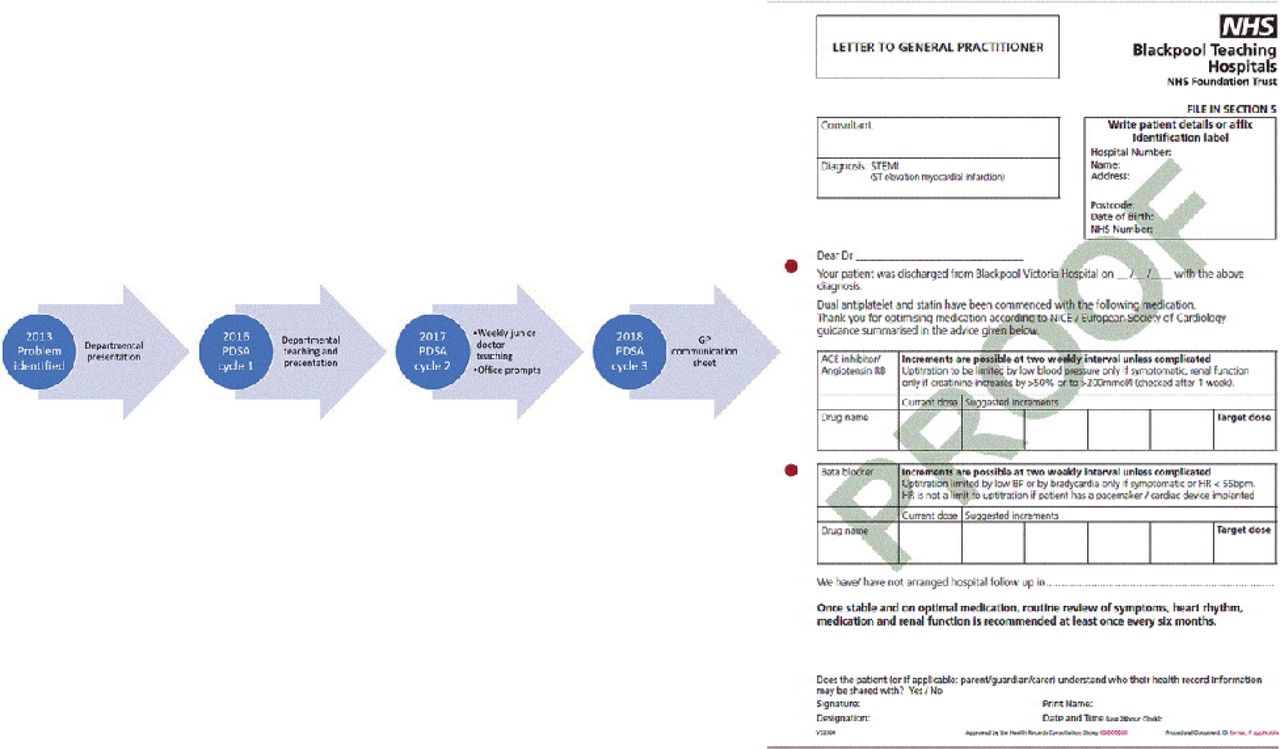
Baseline data was collected in 2013 when 42 consecutive patients fitting the inclusion criteria were reviewed. Three separate PDSA cycles (Fig 1) were then implemented between 2017 and 2018. Consecutive patients’ notes were reviewed 2 weeks after the introduction of each change. Each cycle was completed only after the previous’ data had been analysed and discussed with senior nurses and doctors.

PDSA cycles with ST elevation myocardial infarction (STEMI) discharge GP letter
Results and discussions
PDSA cycle 1 (n=33)
Percentage number of discharges with appropriate secondary prevention planning improved from 26% to 33% when compared with 2013. However, this was not statistically significant (p=0.513).
PDSA cycle 2 (n=26)
There was a vast improvement to 70% adherence with national guidelines (p=0.005).
PDSA cycle 3 (n=32)
This general practitioner letter strategy (see Fig 2) achieved a 75% correct discharge. Compared with PDSA cycle 2, the improvement is statistically insignificant (p=0.684). However, when compared with baseline 2013 data, the improvement is clearly significant (p=<0.001).

Percentage of patients admitted through the PPCI pathway and with a final diagnosis of ST-elevation myocardial infarction (STEMI) that were correctly discharged, according to NICE guidelines
Conclusion
PDSA cycles 2 and 3 appeared most successful in achieving correctly discharged patients. Compared with the educational week for PDSA cycle 2, the STEMI discharge letter was less labour intensive. Furthermore, it is clearer for patients and primary care practitioners. Its introduction requires only a 5-minute presentation and its supply was maintained by the ward clerk, costing around £30 for a booklet of 50. The information is easily reproducible and requires reduced senior input for its maintenance, making it more sustainable as a long-term quality improvement. As such, the STEMI GP letter was unanimously accepted by the cardiology department to be introduced for new teams to use.
- © Royal College of Physicians 2019. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.