
ABSTRACT
Haemolysis is a rare but serious complication of cytomegalovirus (CMV) infection, described mostly in immunocompromised patients, the pathogenesis of which is yet to be fully elucidated. We describe a case of Coombs-positive haemolytic anaemia in an older Caucasian immunocompetent woman after polytrauma, resulting from suspected reactivation of CMV infection and secondary cold agglutinin disease. Clinicians should consider CMV infection in the differential diagnosis of haemolytic anaemia in immunocompetent older adults who are admitted with significant musculoskeletal trauma. Early treatment with B-cell depletion therapy to halt cold agglutinin production can be life-saving.
Case presentation
An 81-year-old woman, with good baseline cognition and mobility, was found in the hallway of her home following a fall from standing with an unknown length of lie. Her past medical history was significant for hypertension and idiopathic ataxia. Current medications included indapamide 2.5 mg once daily, doxazosin 1 mg once daily, lacidipine 4 mg once daily and prochlorperazine 10 mg twice daily.
On presentation she was complaining of right shoulder and right trochanteric pain and was unable to bear weight. On examination, her core temperature was 37°C, she was alert and coherent and her vital signs were normal. There was extensive bruising of the right upper and lower limbs. Her right shoulder was deformed, swollen and painful to palpation. Both lower limbs were symmetrical and resting in the anatomical position.
Initial laboratory investigations revealed haemoglobin (Hb) 88 g/L (reference range 115–165 g/L), mean corpuscular volume (MCV) 91 fL (76–98 fL), total bilirubin 68 μmol/L (<21 μmol/L), C-reactive protein (CRP) 47 mg/L (0–4 mg/L), sodium 108 mmol/L (133–146 mmol/L), creatinine 78 μmol/L (45–84 μmol/L) from a baseline of 25 μmol/L and urea 16.6 mmol/L (2.5–7.8 mmol/L). The remaining haematological and biochemical parameters were normal. Chest radiograph demonstrated a right clavicle fracture with nothing else of note. Pelvic X-ray showed no overt fracture.
The patient was observed to have an isolated episode of large-volume haematemesis. She was transfused 2 units of packed red blood cells, given crystalloids, pantoprazole 40 mg, tranexamic acid 1 g and metoclopramide 10 mg intravenously, and a urinary catheter was inserted for fluid balance monitoring. She subsequently had an oesophago-gastro-duodenoscopy (OGD), which showed altered blood but no bleeding source.
Over the next 72 hours, she complained of neck pain and developed an oxygen requirement of 3 L/min via a nasal cannula in order to maintain oxygen saturations >94%. Her anaemia worsened, with Hb dropping to 62 g/L, MCV increasing to 98 fL and bilirubin rising to 71 μmol/L, with a conjugated bilirubin level of 16 μmol/L (0–5 μmol/L). The urea decreased to 3.8 mmol/L at the same time as her creatinine returning to baseline of 25 μmol/L, resolving the acute kidney injury. Extended anaemia screen and thyroid function tests were normal.
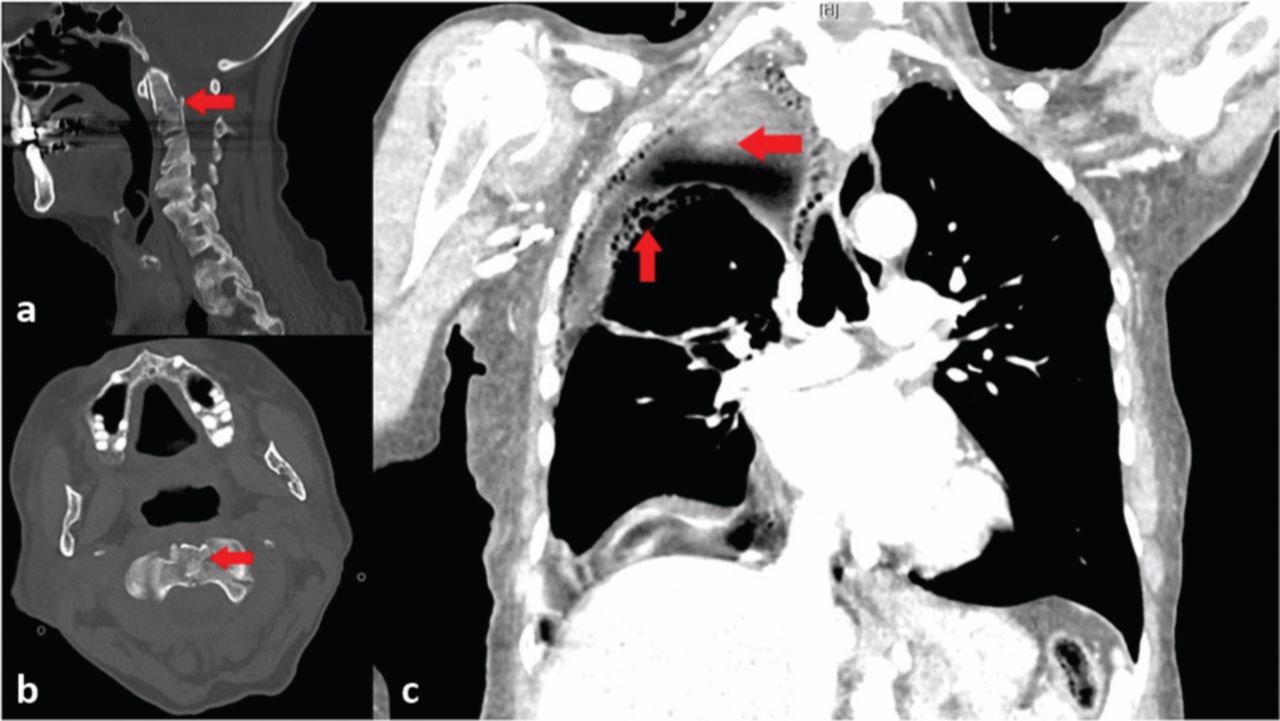
A computed tomography (CT) of the neck discovered an angulated comminuted displaced fracture at the base of the odontoid process involving the left lateral mass, superior articular process and extending into the left transverse foramen (Fig 1a, b). A right haemopneumothorax and left lung upper lobe consolidation was noted. The patient's neck was immobilised with a Miami J collar.
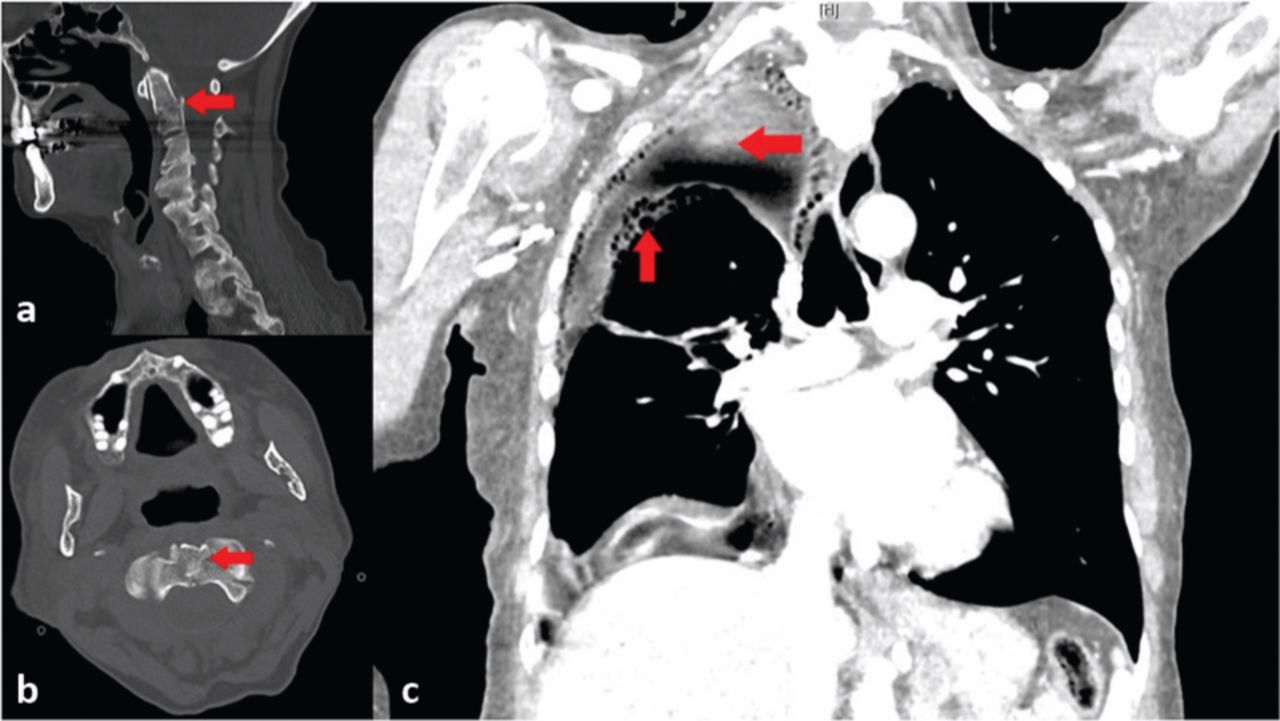
Computed tomography of neck in sagittal (a) and axial (b) planes, demonstrating odontoid peg fracture (arrow), and CT of the chest demonstrating a large right-sided haemothorax with air bubbles in the pleural cavity (arrows) (c).
A CT of the chest, abdomen and pelvis (Fig 1c) showed a large right-sided haemopneumothorax with air bubbles due to a slow air leak, a right sided mid-clavicular fracture, a solitary left-sided, and multiple right-sided, rib fractures and complex comminuted pelvic fractures involving the right pubis, inferior pubic ramus, anterior column of the right acetabulum and the lateral aspect of the right sacral ala.
A surgical chest drain was placed, which passed 500 mL of frank blood initially. After 3 days, the haemothorax was resolved on chest X-ray and the chest drain was removed, draining a total of 1.93 L.
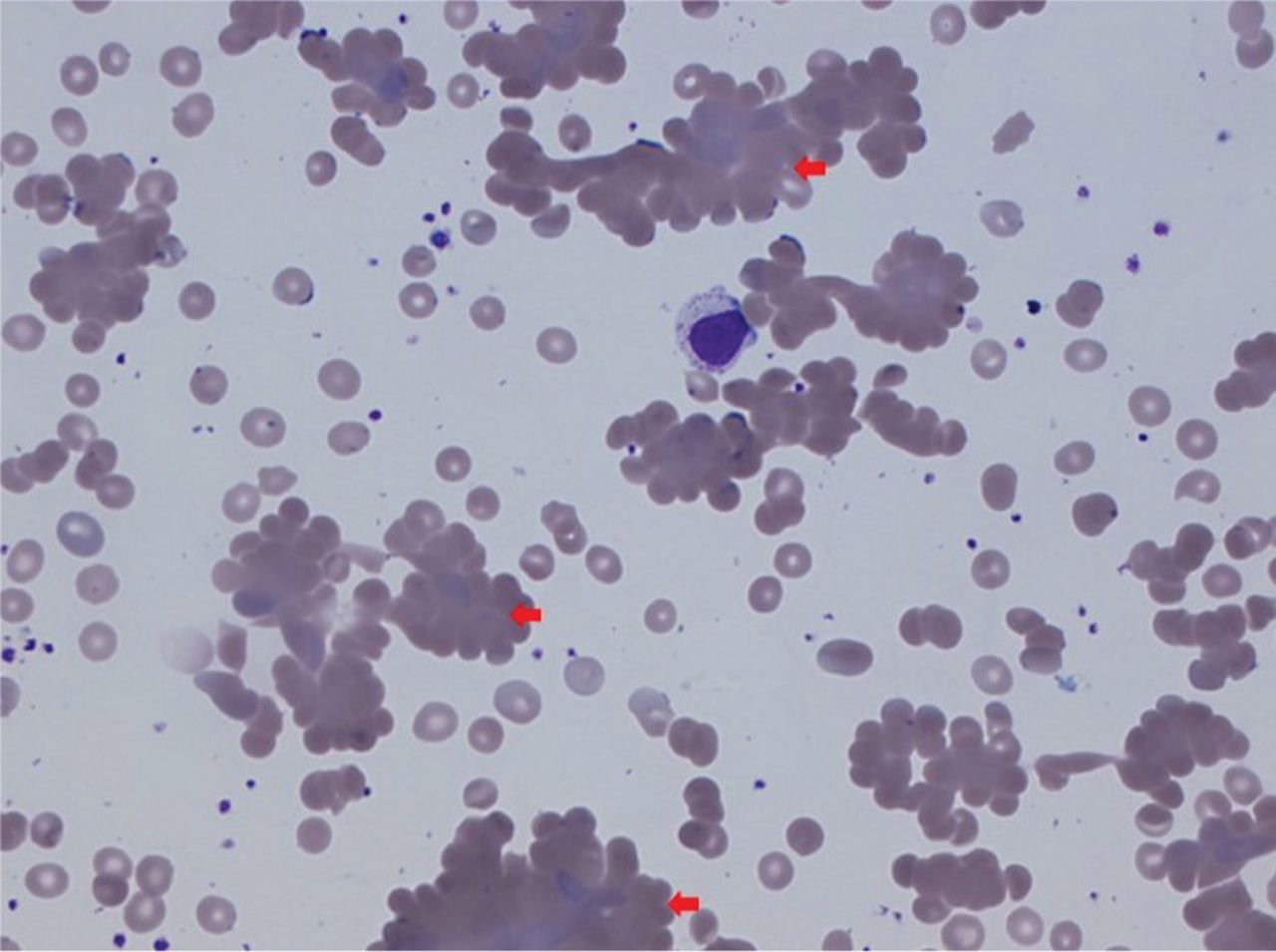
A blood film showed moderate macrocytosis and cold agglutinins (Fig 2). Direct Coombs test was positive for C3d. Protein electrophoresis showed immunoglobulin M (IgM) kappa paraproteins, with an IgM titre of 2.43 g/L (0.5–2.0 g/L). Haptoglobin level was <0.2 g/L (0.3–2.0 g/L), complement C4 level of 0.06 g/L (0.14–0.54 g/L), lactate dehydrogenase (LDH) 399 IU/L (135–214 IU/L) and an absolute reticulocyte count of 144.3×109/L (25–85×109/L) with a reticulocyte percentage of 7.8% (0.5–2.5%). Serology was positive for cytomegalovirus (CMV) IgG and IgM, and negative for Mycoplasma pneumoniae, HIV, Epstein–Barr virus, influenza virus, hepatitis C virus, legionella and syphilis. A diagnosis of CMV-induced secondary cold agglutinin disease (CAD) was now made.
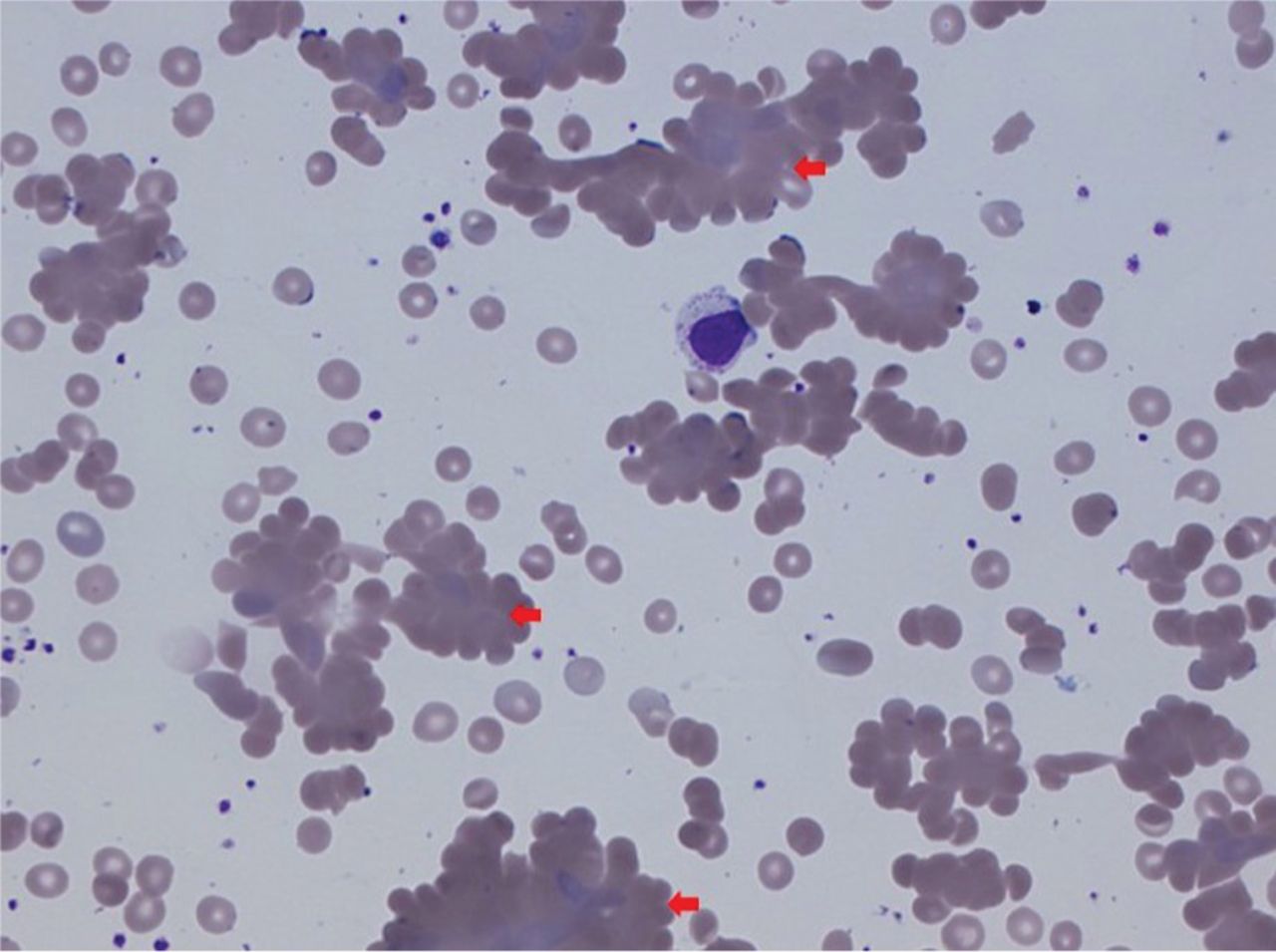
Blood film demonstrating clumps of erythrocytes (arrows), typical of aggregates seen in cold agglutinin disease.
Post-chest drain insertion, the patient continued to haemolyse, and her initial post-transfusion Hb of 92 g/L dropped to 76 g/L after 48 hours. She was initially treated with prednisolone 60 mg for 1 week before starting a reducing regime, but haemolysis continued. She was therefore given rituximab 500 mg once weekly for a planned 4 weeks. The Hb recovered from 70 to 95 g/L within 2 weeks without further transfusion.
Discussion
Haematemesis acted as a red herring, distracting clinicians from significant polytrauma. The coffee-ground vomit was likely due to stress-induced gastritis. The rush to perform OGD could have easily resulted in tetraplegia or death.
Falls are one of the most common hospital presentations in older people. Complacency can easily result in missed injuries. It has been predicted that up to 39% of injuries are missed or have delayed diagnosis, with approximately 15–22.5% of these being clinically significant.1 Odontoid peg fractures have an overall mortality of 14.6% at 30 days and 34.1% at 1 year.2 A separate study suggests that geriatric polytrauma has an overall mortality as high as 65%, with patients who suffer major blood loss (Hb <8 g/dL) having a mortality three times higher than those with moderate or minor blood loss (Hb ≥8 g/dL).3
Cryoglobulinaemia accounts for nearly 25% of autoimmune haemolytic anaemia4 and is important to rule out in cases of suspected haemolytic anaemia. The patient's haemodynamic stability is key to survival in polytrauma, with an Hb level <8 g/dL conferring a three times greater mortality than those with an Hb level ≥8 g/dL.3 It has been demonstrated in surgical cases that CAD-induced haemolysis can be triggered within less than 60 minutes of sedation under general anaesthetic, and therefore, in our patient, we speculate that the cascade may have been triggered after a relatively short lie following a fall, and it is likely that there was clinically silent CAD.5
Severe haemolysis is a rare but potentially life-threatening complication of CMV infection described mostly in immunocompromised adults.4 However, up to 33% of critically ill patients can suffer from reactivation of CMV,6 and trauma victims have the second highest rate of CMV reactivations in an intensive care setting.6 This is likely due to acquired immunological deficiencies that occur after trauma.7 The risk of CMV reactivation increases with the total number of red blood cells transfused,8 and CMV can act as an independent cause of haemolytic anaemia, in addition to precipitating CAD and exacerbating cold agglutination.9
The acute phase reaction following trauma can act to raise complement C3 and C4 levels, activating C5, leading to complement-induced intravascular haemolysis and a decompensation of CAD.10 It is notable that foreign bodies, such as a plastic chest drain, can activate the alternative complement pathway when plastic comes into contact with blood.4 This would partially explain why our patient continued to haemolyse for so long, despite a normal body temperature.
Prednisolone should rarely, if ever, be used in the treatment of CAD. Evidence suggests that prednisolone has poor efficacy even at high doses, as seen in our patient, and that drugs such as rituximab, which show an overall response rate of 45–66%, should therefore be used as first-line therapies in patients with symptomatic CAD and significant haemolysis.11 Rituximab is an anti-CD20 monoclonal antibody that depletes B cells and thereby interferes with the production of cold agglutinins. In acute severe intravascular haemolysis, the C5 inhibitor eculizumab is recommended, because it blocks the terminal complement pathway and acts quicker than rituximab.5,12
Conclusion
Our patient suffered a perfect storm. We postulate that trauma triggered an acute phase reaction to raise complement C3 and caused an immunocompromise, allowing reactivation of dormant CMV. This likely led to decompensation of previously undiagnosed CAD, triggering severe haemolysis in an already critically ill patient. This is the first documentation of polytrauma in a geriatric patient resulting in reactivation of CMV infection and secondary CAD-induced haemolytic anaemia. At time of writing, 4 months after presentation, our patient has been discharged from hospital, and is stable from a haematological perspective (Hb 107 g/dL) with a Miami J collar still in place. The factors that likely contributed to her survival so far include: firstly, she suffered an Anderson and D'Alonzo type III odontoid peg fracture, which has a higher survival rate than the more unstable type II fractures. Secondly, she was transfused early when her anaemia was discovered. Thirdly, treatment with rituximab was initiated within the first week and, finally, the haemopneumothorax developed slowly, allowing time for diagnosis and treatment.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.