
ABSTRACT
We describe a case of an 82-year-old man who developed an anterior ST-elevation myocardial infarction (STEMI) and left ventricular thrombus while an inpatient following a diagnosis of severe COVID-19 infection (SARS-CoV-2). His D-dimer was significantly elevated at 12,525 ng/mL (normal range <243). He unfortunately died despite management with thrombolysis, warfarin and non-invasive ventilation. This case provides an example of a likely arterial thrombotic complication of severe COVID-19 infection. Clinicians should be aware of this possibility in such patients, with a severely prothrombotic state as a possible underlying aetiology. Further research is required to establish any causative link, pathophysiological mechanisms and whether modification to existing venous thromboembolism prophylaxis strategies may also reduce arterial thrombotic complications of severe COVID-19 infection.
Case presentation
An 82-year-old man was admitted following a 10-day history of a productive cough of green sputum, accompanied by fevers. He had also become increasingly short of breath over the 2 days prior to admission. He did not experience any chest pains prior to admission.
He had a background of a total knee replacement. He was not hypertensive and had recent normal glycated haemoglobin (HbA1c) and total cholesterol levels, with no history of ischaemic heart disease. He had a 10 pack-year smoking history and drank 10 units/week of alcohol. There was no significant family history. Prior to admission he lived at home independently, his Rockwood Clinical Frailty Scale score was 2 and he had a good exercise tolerance of approximately 1 mile.
On arrival he was hypoxic (oxygen saturations were 71% on room air and 96% on 40% oxygen via Venturi mask) and tachypnoeic (26 breaths/minute). His heart rate was 71 beats/minute, blood pressure 132/81 mmHg and temperature 36.5°C. Examination revealed increased work of breathing and bilateral fine inspiratory crepitations to the mid-zones on auscultation.
His arterial blood gas showed type 1 respiratory failure on 60% fraction of inspired oxygen (FiO2). Blood tests revealed a significantly raised C-reactive protein (CRP) of 412 mg/L (normal range 0–5). His chest X-ray demonstrated severe diffuse bilateral infiltrates (Fig 1) and his admission electrocardiography was unremarkable. COVID-19 infection with SARS-CoV-2 was highly suspected and a naso-pharyngeal polymerase chain reaction swab confirmed this diagnosis.
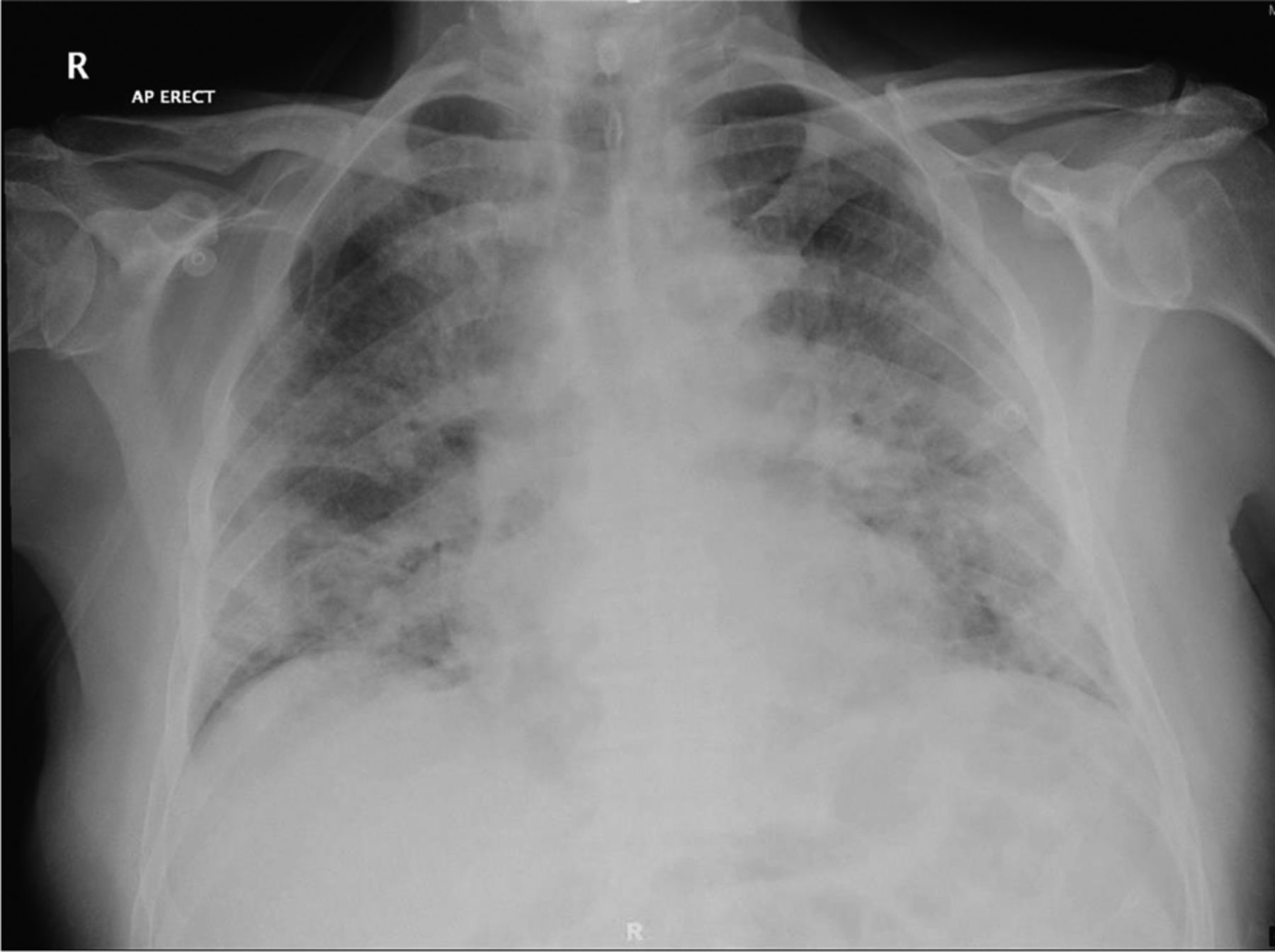
Chest X-ray demonstrating severe diffuse bilateral infiltrates.
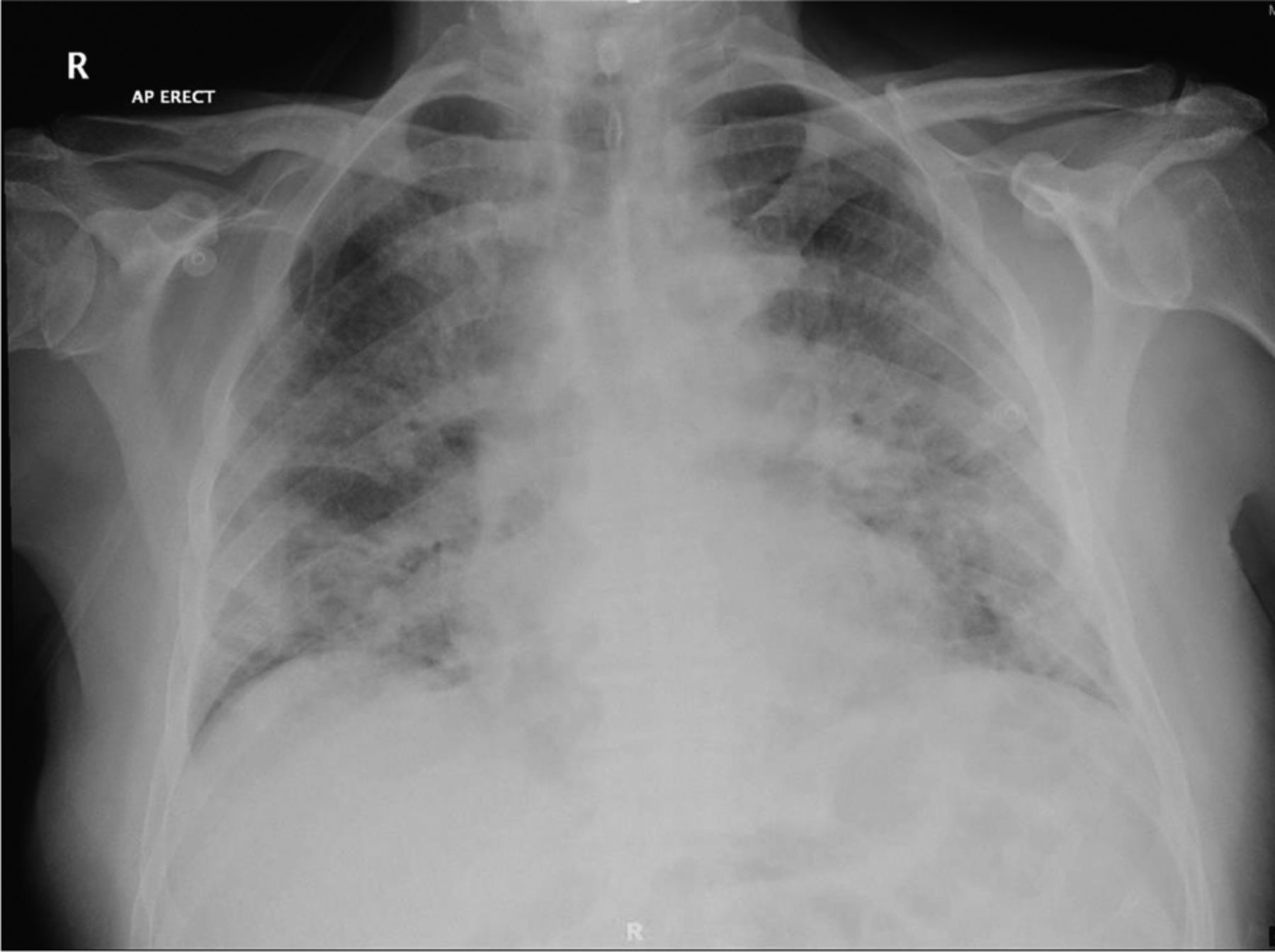
After 36 hours of admission, he developed sudden onset central crushing chest pain on the medical ward. Electrocardiography revealed dynamic marked ST-segment elevation in leads V1–4, with reciprocal changes in the lateral leads, consistent with an acute anterior ST-elevation myocardial infarction (STEMI; Fig 2). Troponin T was raised at 354 ng/L (range 0–14) and 9 hours later increased to 4,549 ng/L. Subsequent electrocardiography revealed deep Q waves in leads V1–4 and the inferior leads. His case was discussed with the regional primary percutaneous coronary intervention (PPCI) centre. Given his pre-existing oxygen requirement, it was felt that he would require invasive ventilation to facilitate transfer to a different hospital site for PPCI. After discussion with local and regional cardiologists, intensivists and physicians, it was decided that he was not a candidate for intubation or resuscitation. A decision was made to treat locally with thrombolysis with 8,000 units of intravenous tenecteplase, 300 mg of aspirin, 300 mg of clopidogrel, intravenous morphine and an intravenous glyceryl trinitrate infusion. He demonstrated a partial response with a marked reduction in his chest pains and remained haemodynamically stable.

Electrocardiography revealing dynamic marked ST-segment elevation in leads V1–4, with reciprocal changes in the lateral leads, consistent with an acute anterior ST-elevation myocardial infarction.
He was initiated on non-invasive ventilation using continuous positive airway pressure (CPAP) with 75% FiO2 and positive end-expiratory pressure of 10 cmH2O. He was also started on 1.25 mg of bisoprolol and 1.25 mg of ramipril once daily, subcutaneous 60 mg of enoxaparin twice daily and 80 mg of atorvastatin once daily.
Further tests revealed a significantly elevated D-dimer at 12,525 ng/mL (normal range <243) and raised lactate dehydrogenase at 1,635 IU/L (normal range 240–480). He was lymphopenic for the majority of the admission (nadir 0.66×109/L). His peak CRP was 501 mg/L, 9 hours after chest pain onset.
A transthoracic echocardiography was performed and revealed a moderately impaired left ventricular ejection fraction (approximately 40%), a left ventricular aneurysm and regional wall motion abnormalities (basal septal and apical wall hypokinesis). A small left ventricular thrombus was also detected measuring 0.8×1.1 cm (Fig 3). The right ventricle appeared normal with no significant valvular abnormalities. Due to the left ventricular thrombus, warfarin was initiated with a target international normalised ratio of 2–3.

A small left ventricular thrombus was also detected measuring 0.8×1.1 cm.
As he was not a candidate for invasive ventilation, he received a prolonged CPAP course of 14 days. Unfortunately, this could not be weaned, with a persistent FiO2 requirement of >55%. His dependence on CPAP meant coronary angiography could not be performed. A repeat chest X-ray demonstrated worsening diffuse bilateral infiltrates. His FiO2 increased to 95% despite a trial of antibiotics and diuresis, so a decision was made for palliative care and withdrawal of CPAP treatment. He sadly died on the 16th day of his admission.
Discussion
We describe a case of a left ventricular thrombus associated with an STEMI in a patient with severe COVID-19 infection, who subsequently died. We suspect that these arterial thrombotic events were complications of severe COVID-19 infection. A recent case series described 18 patients with ST-segment elevation and COVID-19 infection.1 Like our patient, all these patients had a significantly raised D-dimer, which is an unusual finding in acute myocardial infarction. Notably, eight out of 18 patients in this series suffered a STEMI after developing confirmed COVID-19 infection. Another recent case series described five large vessel ischaemic strokes in patients with an age range of 33–49, who were all also diagnosed with COVID-19 on admission.2 Three of these patients also had a significantly elevated D-dimer.
A significant prothrombotic state in severe COVID-19 infection has been described, with a combination of severe inflammation, cytokine storm, immobility and disseminated intravascular coagulopathy.3,4 In one case series of 184 COVID-19 patients on intensive care units, 27% had a venous thromboembolic event and 3.7% had an arterial thrombotic event despite standard prophylaxis.5 Furthermore, thrombotic microvascular injury and endothelial cell damage have been evident on post-mortem studies of severe COVID-19 patients.6
Managing patients with confirmed severe COVID-19 and acute myocardial infarction provides a significant management challenge. The finding of a left ventricular thrombus in this case is consistent with a strongly prothrombotic state. It may be more important to screen for left ventricular thrombus in such patients. A significant prothrombotic state in severe COVID-19 infection appears to increase the risk of both venous and arterial thrombotic events, which can be fatal. It is possible that COVID-19 specific thromboprophylaxis regimens may reduce both venous thromboembolism rates and acute cardiovascular events such as myocardial infarction and stroke in the context of severe COVID-19 infection. Further research is required in this area and also to explore whether modulation of acute proinflammatory pathways or the immune response would reduce acute thrombotic complications of severe COVID-19.
Learning points
Severe COVID-19 infection appears to be linked to a prothrombotic state which may cause severe arterial thrombotic complications including STEMI and ventricular thrombus formation. Clinicians should be alert to this possibility when managing such cases. Further studies are required to establish any causative link and any pathophysiological mechanisms.
Further research is required to determine optimal anti-coagulation strategies in severe COVID-19 patients for prevention and treatment of venous/arterial thromboses.
Patients with STEMI in the context of severe COVID-19 infection appear to often have a significantly elevated D-dimer. This is not normally a feature of acute myocardial infarction and may reflect an underlying prothrombotic state.
Acknowledgements
We thank to the patient's family for allowing us to publish this case report.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.