
ABSTRACT
We report a patient with chronic diabetes and was referred for recent onset proteinuria. Light microscopy of the renal biopsy specimen showed mildly expanded mesangium with mesangial hypercellularity and segmental sclerosis, features compatible with diabetic glomerulosclerosis. However, crystalglobulin-induced nephropathy with crystal deposit was identified on electron microscopy. Renal biopsy is often performed for diabetic patients who present with proteinuria and light microscopy often shows features of diabetic glomerulosclerosis. Additional information may occasionally be revealed on electron microscopy, altering the subsequent plan of management.
Case presentation
A 45-year-old man who had a history of hypertension, hyperlipidaemia and type 2 diabetes mellitus with retinopathy presented with frothy urine for 3 months. He had had diabetes for 4 years, and his medication included lisinopril 20 mg daily, amlodipine 10 mg daily, metformin 1,000 mg twice daily and glimepiride 1 mg every morning. Physical examination showed no oedema; his blood pressure was 140/80 mmHg, and the heart rate was 72 beats/min. Laboratory tests revealed a glycated haemoglobin (HbA1c) level of 7.1%, serum creatinine of 95 μmol/L, serum albumin of 33 g/L, total protein of 80 g/L and the spot urine total protein-to-creatinine ratio was 2.14 mg/mg-Cr. Further blood tests including hepatitis B surface antigen, anti-hepatitis C antibody, antinuclear antibody and anti-neutrophil cytoplasmic antibody were negative. Ultrasound showed normal-sized kidneys.
Investigation
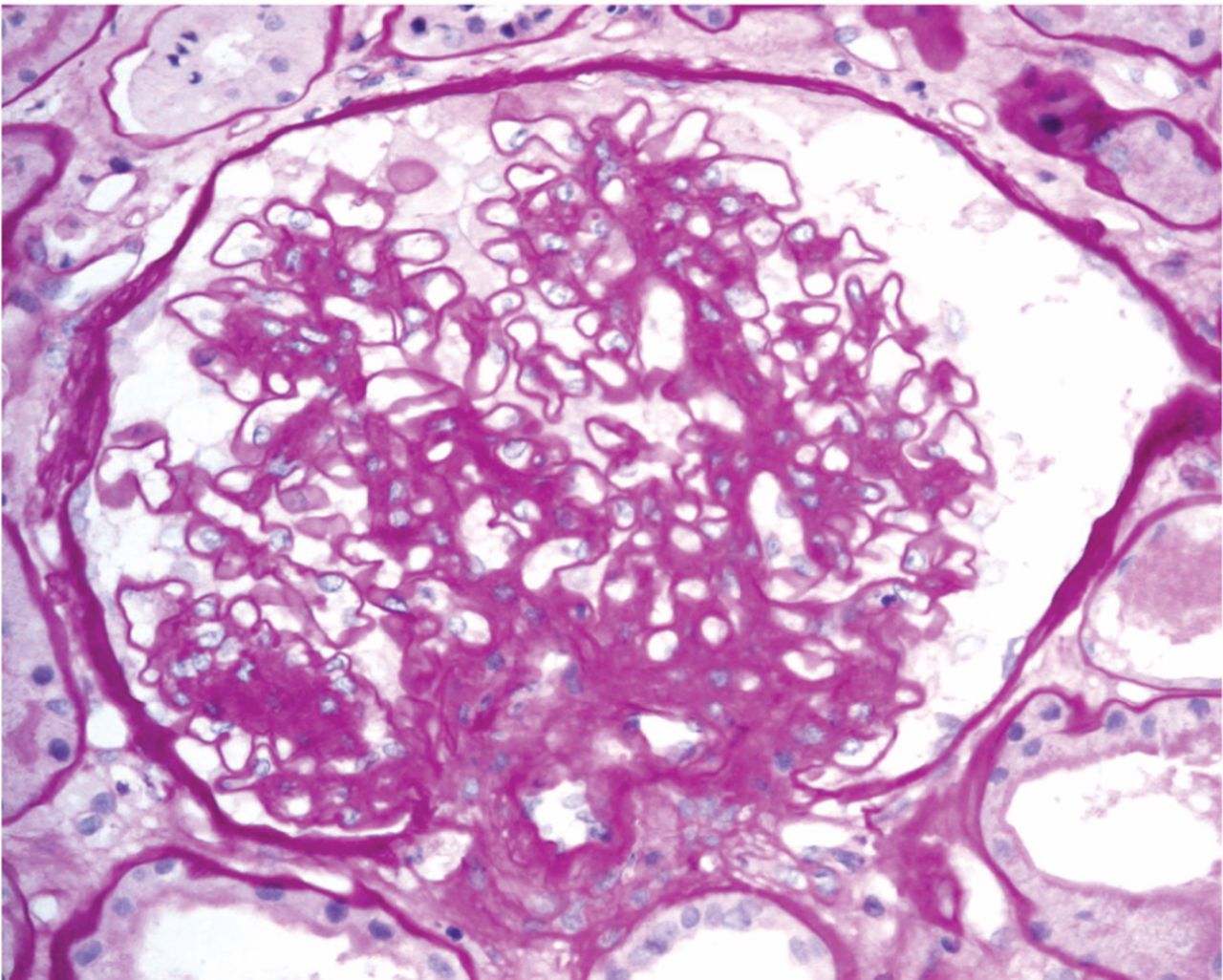
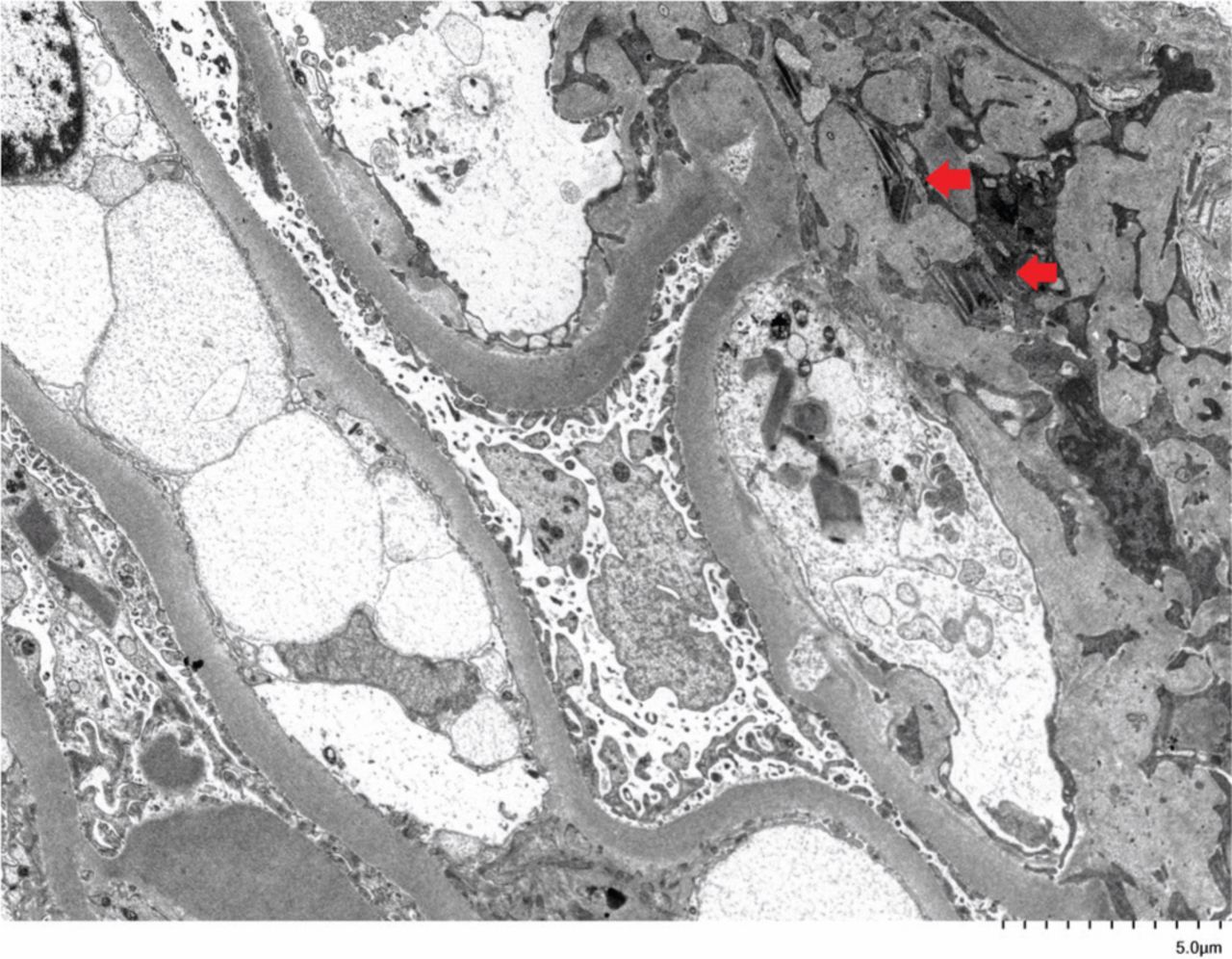
A renal biopsy was performed. Light microscopy of the renal biopsy specimen showed mildly expanded mesangium with mesangial hypercellularity and segmental sclerosis (Fig 1). There was no leukocyte infiltrate or necrotising lesion. Immunofluorescent study showed glomerular and tubular staining with predominantly kappa light chain. Electron microscopy revealed a uniformly thickened glomerular capillary basement membrane, prominent surface microvilli in podocytes with intracytoplasmic crystalline structure and intra-lysosomal inclusions (Fig 2). Similar crystalline cytoplasmic inclusion was also found in proximal tubules (not shown). Serum protein electrophoresis demonstrated immunoglobulin A (IgA) kappa paraproteinaemia 13 g/L, with a kappa-to-lambda ratio of 71 (reference range 0.26–1.65). Bone marrow examination showed 30–40% clonal plasmacytosis with kappa light chain restriction. There was no other clinical feature of Fanconi syndrome; serum uric acid, bicarbonate and phosphate levels were normal, although urine amino acid was not tested.
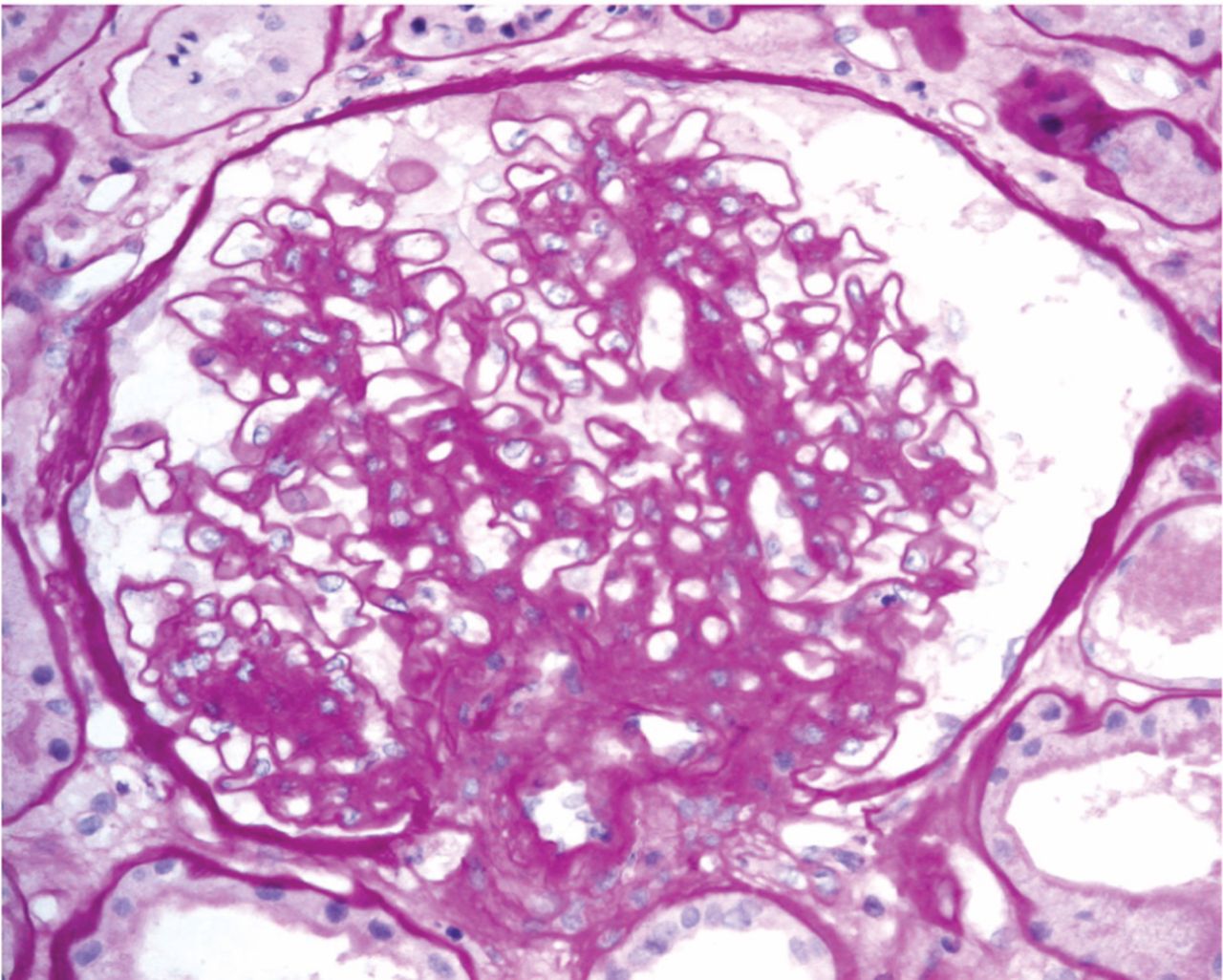
Light microscopy of renal biopsy with periodic acid–Schiff (PAS) stain showed mildly expanded mesangium with mesangial hypercellularity and segmental sclerosis.

Electron microscopy of renal biopsy showing crystalline structure (red arrows) in glomerular podocyte.
Discussion
Crystal nephropathies are classified according to the localisation of crystal deposits, namely the renal vasculature (type 1), the nephron (type 2) and the urinary tract (type 3).1 Crystal nephropathies may be caused by monoclonal gammopathy when the monoclonal immunoglobulin gives rise to the crystals.2 The clinical spectrum includes light chain proximal tubulopathy, crystal storing histiocytosis and crystalglobulin glomerulonephritis. Depending on the dynamics of crystal accumulation, either acute kidney injury or chronic kidney disease could occur.1
This case demonstrated the importance of electron microscopy in establishing the correct diagnosis. The IgA kappa paraproteinaemia and raised kappa to lambda ratio, which are often performed and available before renal biopsy, may give a clue to the underlying pathology. The identification of crystal deposit on electron microscopy is the key to the diagnosis. Bone marrow should be performed as the next step for clonal identification, in which plasma cells, lymphoid aggregates or amyloid deposits should be assessed. Imaging studies, such as computed tomography, should be considered especially when bone marrow examination is unrevealing and low-grade lymphoma is suspected. Clone-directed therapy is central to the management of monoclonal gammopathy of renal significance and bortezomib has the most robust data.3
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.