
ABSTRACT
Background Despite a body of evidence demonstrating reduced incidence of post-lumbar puncture headache associated with pencil-point (vs bevelled-edge) needles, their use remains variable in the UK.
Methods A multimodal longitudinal intervention was performed over a 12-month period at a tertiary neurology referral centre. In addition to simulation training using pencil-point needles and an electronic documentation pro forma, a change in the default needles presented in clinical environments was performed.
Results Prior to the intervention, pencil-point needle usage was minimal. Documentation significantly improved throughout the intervention period. Simulation training interventions only resulted in transient, moderate improvements in pencil-point needle usage. However, changing the default produced a marked increase in use that was sustained. No significant changes in operator success rate were found.
Conclusions In the context of wider literature on the power of default options in driving behavioural choices, changing defaults may be an effective, inexpensive and acceptable intervention to improve lumbar puncture practice.
Introduction
Headache is a historically known complication of lumbar puncture (LP). In 1899, August Bier and his assistant August Hildebrandt performed LPs on each other attempting to reproduce complications from spinal anaesthesia in humans.1 Both men developed severe headaches beginning the following day. For a further 8 days, Bier was forced to lie flat as rising provoked severe pain. This classical description remains very relevant to modern clinical practice. Post-dural-puncture headache (PDPH) commonly causes morbidity, in serious cases requiring hospital admission or epidural blood patch.2–4 One key modifier of these risks is spinal needle design.
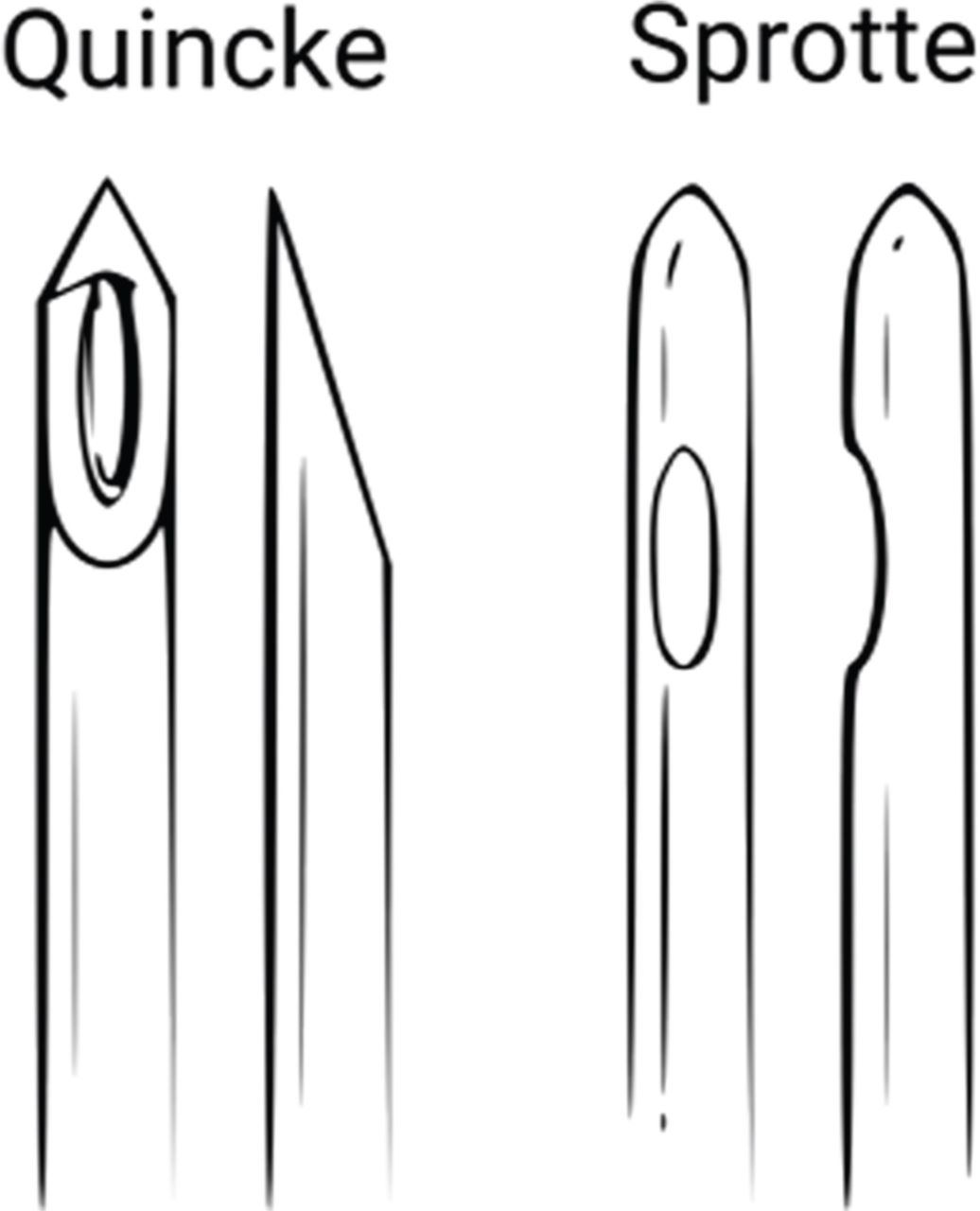
A wide variety of designs have been used historically.5 The bevelled tip of the conventional Quincke needle readily cuts through tough ligamentous structures and the dura mater. With electron microscopy, the dural defect left by this needle is seen as a crescent-shaped flap with cleanly-cut borders.6 This may allow persistent cerebrospinal fluid (CSF) leak and intracranial hypotension to develop, leading to headache. To address this problem, needles with blunter ‘pencil-point’ or ‘atraumatic’ tips were designed with the aim of dividing rather than cutting dural fibres (Fig 1). The Greene, Whitacre and Sprotte needles were introduced in the 1920s, 1950s, and 1980s, respectively.
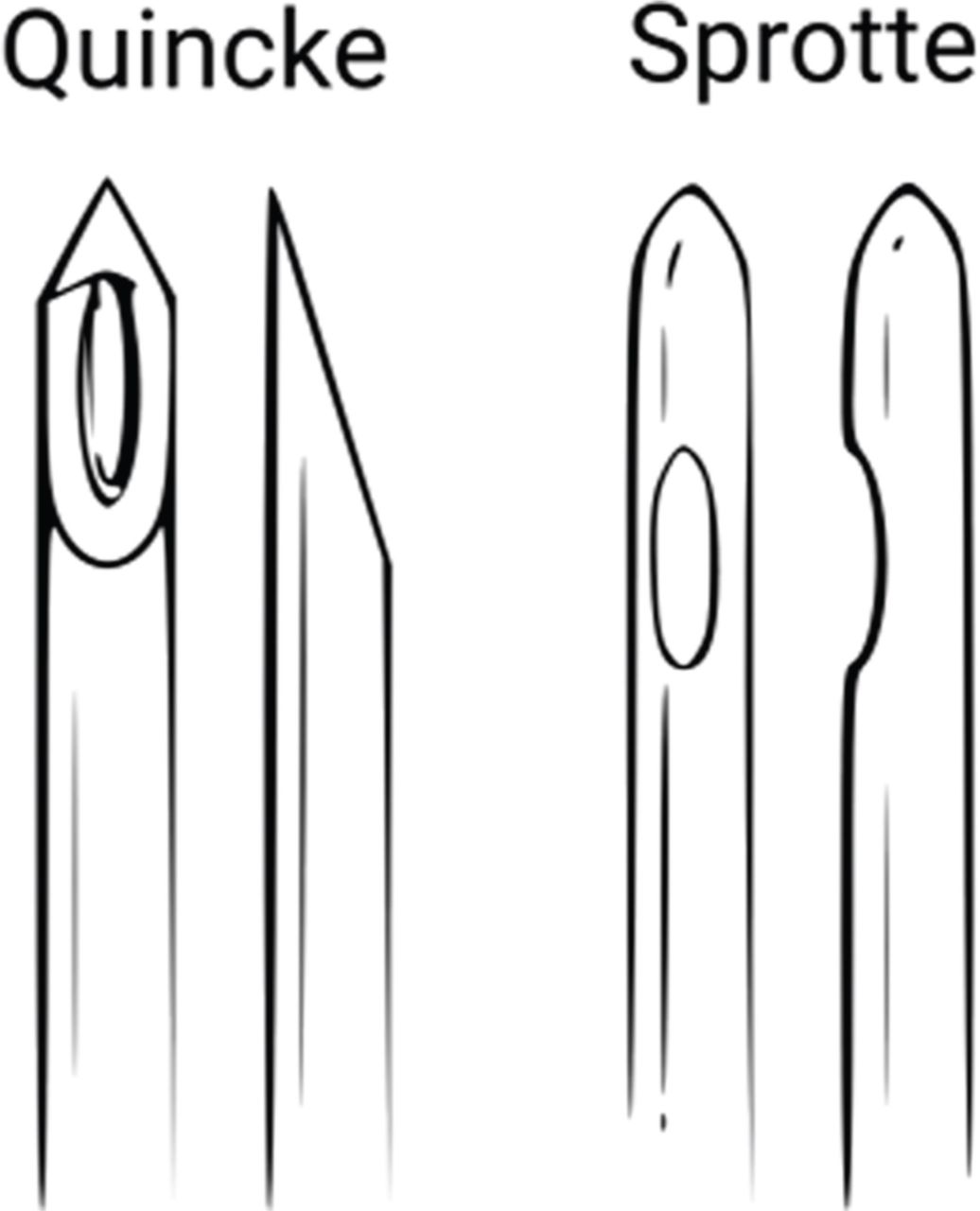
Examples of different needles: sharp tip (Quincke) and blunter ‘pencil-point’ or ‘atraumatic’ tip (Sprotte).
These needles form irregular defects with ragged borders and a smaller cross-sectional area on the arachnoid surface.6 Mechanically, these defects may be less likely to allow persistent CSF leak. The greater tissue destruction at the ragged edges has also been suggested to provoke inflammation, facilitating closure. Precise mechanism notwithstanding, if needle design mitigates headache risk, a clinician’s choice of needle becomes an important determinant of LP outcomes.
Meta-analyses suggest that larger diameter needles and cutting needle tips increase headache risk.7,8 The difference is clinically meaningful, with PDPH incidence, intravenous fluid or analgesia requirement, and blood patch all reduced by at least 50% with pencil-point needles. LP success rate is unchanged. Where equivalent, replacing cutting needles with pencil-points would benefit patients and save healthcare resources.8,9
Adoption of pencil-point needles as the standard of care is widespread in the original context of their development – spinal anaesthesia.10 However, in other clinical settings where LP is performed (acute medicine, neurology and neurosurgery) cutting needles remain in common clinical use despite various interventions.11 This study reports a multimodal intervention where, in addition to standard interventions, the effect of replacing the default stocked needle in the ward environment was assessed.
Methods
The clinical population was ambulatory outpatients who had diagnostic LP, generally prior to neurological diagnosis. This group did not include inpatient admissions to acute medicine. Patients having large-volume CSF drainage for idiopathic intracranial hypertension were also excluded. Electronic records were reviewed for diagnostic LPs at the neurology investigations unit (NIU), Oxford University Hospitals NHS Foundation Trust, from October 2017 to December 2018. LPs from October 2016 were a pre-intervention reference. Pencil-point needle usage was recorded in addition to a documentation quality score based on local and national clinical guidelines. One point for recording each of (to a maximum of seven) procedure indication, platelets/clotting checked, causes of intracranial pressure reviewed, informed consent obtained, local anaesthetic administration, CSF appearance and tests requested.
The intervention comprises three areas.
Electronic pro forma for documentation (introduced September 2017) recording pre-procedure safety checks, consent, patient positioning, type of needle used and investigations requested.
Simulation training sessions for clinicians performing LPs using a training model and pencil-point needles. Sessions took place in September 2017, February 2018 and July 2018.
Changing the default needle. In September 2018, the 22G Quincke needles stocked by default in trolleys and cupboards on the NIU were replaced with 22G Sprotte needles. Quincke needles remained accessible in ward stores if specifically indicated for therapeutic CSF drainage.
Results
Between October 2017 and December 2018, 210 LPs were recorded. Documentation score improved with the pro forma and training interventions. However, prior to the change in default needle, pencil-point needle usage was variable. In the 3 months after each training session, transient increases in atraumatic needle usage were seen. After the 1st intervention (proforma and simulation training) in September 2017, mean pencil-point needle usage October–December 2017 was 37%. Following a 2nd intervention (simulation training) in February 2018, mean pencil-point needle usage was 23%. However, usage returned to near baseline following these increases (Fig 2).
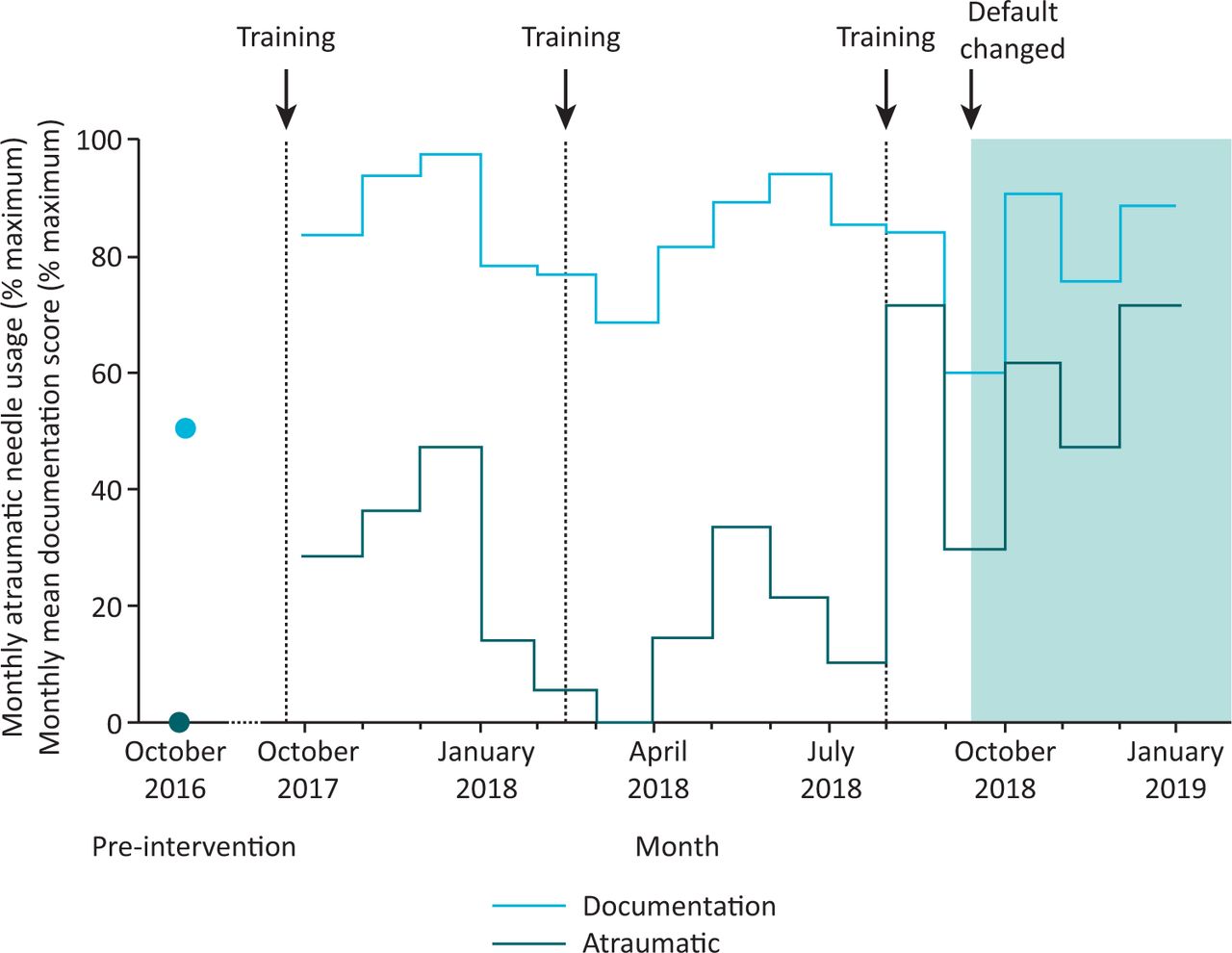
Monthly atraumatic needle usage and mean documentation score.
On changing the default needle available on the ward in September 2018, a larger and sustained increase in mean pencil-point needle usage over the subsequent 3 months was seen (60.1%). Clinician success rate did not differ throughout the study period with cutting vs pencil-point needles (48% vs 46%; p=0.4).
Discussion
Our multimodal intervention increased pencil-point needle usage in this centre, illustrating the importance of systemic factors in clinical medicine. Training and pro forma interventions have previously been characterised by transient effects, diluted by staff turnover and fatigue. In this study, the default needle in trolleys and stock cupboards was changed to pencil-point, which was associated with a more sustained change in needle usage.
Behavioural economics describes the marked influence on human decision-making of a ‘choice environment’ composed of default settings, presentation of options and a range of other subtle cues.12 No choice environment is neutral, and existing structures may favour decisions that cause undesirable outcomes. ‘Choice architecture’ is the design of small alterations, described as ‘nudges’, that avoid undue restriction, while promoting decisions associated with a desired outcome. A range of ethical and practical caveats accompany these design choices, and interventions based on behavioural theories require a robust evidence base to justify implementation.
Changing defaults is a well-established method to drive behavioural change more widely in medicine.13 Opt-out systems for organ donation result in substantially more organs available for transplant.14 Changing defaults in electronic prescribing systems promotes cheaper generic prescribing.15 Far fewer urinary tract infections occur when indwelling urinary catheters are routinely removed after a certain time.16 More widely, people opt in to receive email marketing, change their energy supplier and open retirement savings at rates strongly determined by default options.17–19
By following up three different intervention styles (pro forma, training and choice architecture), we are able to differentiate the impact of these interventions and observe their impact over time. Through capture of all LPs done in a single unit by a range of clinical staff of similar background in the same environment, we reduce ecological effects and site-specific confounders. Unforeseen negative effects of the intervention were actively investigated, anonymous clinician feedback was solicited, and success rate with needle type was assessed. However, the scope of this study was too limited to detect significant differences in re-admission and blood patch. With regards to headache, accurately determining its rate from clinical records is challenging. Follow-up across the entire time range over which headache can occur was considered outside the scope of this study. Another limitation is the difficulty in inferring changes in clinician choice from clinical documentation; individual procedures were not monitored.
Conclusion
This study resulted in sustained improvement in lumbar puncture practice at this centre. Of the interventions performed, choice architecture was an effective, inexpensive and acceptable approach. In appropriate clinical environments and in the absence of mandated needle choice, it offers significant improvement over previously described interventions to improve LP.
- © Royal College of Physicians 2020. All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.