
Introduction
We describe a rare case of a 69-year-old woman presenting with sudden onset right-sided weakness, sensory disturbance and dysarthria due to a left-middle cerebral artery territory stroke. The patient was successfully thrombolysed, but shortly developed a recurrent stroke in a different vascular territory. Transthoracic echocardiography showed a 2×1 cm mobile structure on the aortic valve. This was resected and histology identified a fibroelastoma. This case highlights the importance of early completion of cardiac investigations in stroke patients, and that a known cardiac papillary fibroelastoma (CPF) should not be considered a contraindication to thrombolysis or thrombectomy.
Case presentation
A 69-year-old woman, with a past history of migraine with aura, hypercholesterolaemia, herpes simplex keratitis and a previous right carotid artery dissection, presented to the emergency department with sudden onset of right-sided weakness, sensory disturbance and dysarthria.
Examination revealed a right hemiparesis with hemi-sensory loss and her National Institute of Health Stroke Scale (NIHSS) score was 6. Systemic examination and observations were normal, and there were no additional heart murmurs.
Computed tomography (CT) of the brain showed no focal intracranial abnormalities and she subsequently underwent intravenous thrombolysis with alteplase. CT of the brain performed 24 hours post-thrombolysis identified a small focal infarction in the posterior left lentiform nucleus and external capsule. Doppler ultrasound of both carotid arteries were normal. Her blood tests showed mildly elevated cholesterol and electrocardiography (ECG) showed sinus rhythm.
She improved with rehabilitation in the stroke unit. Her NIHSS was 1 and she had a modified Rankin score of 2 upon discharge with atorvastatin, perindopril, ranitidine and clopidogrel.
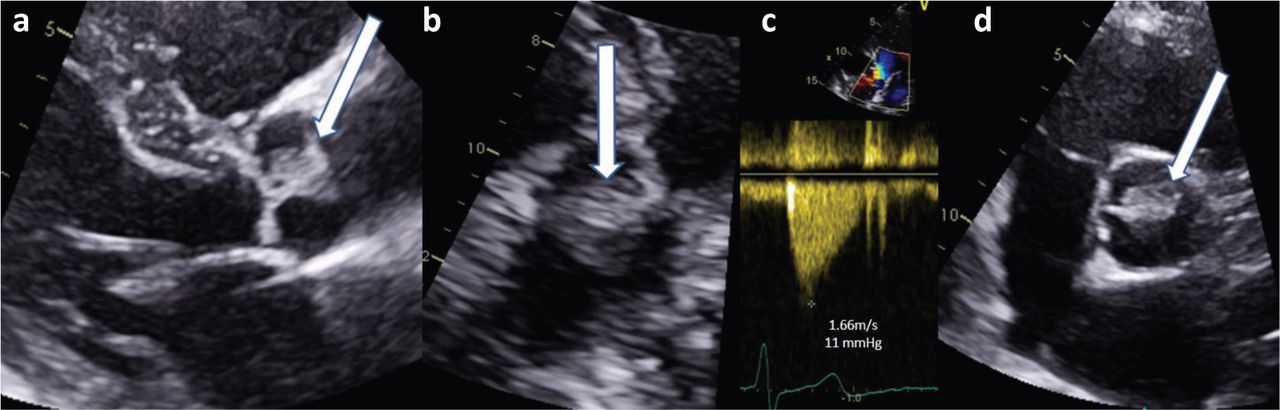
As part of her on-going outpatient investigations, she underwent a 72-hour Holter ECG monitoring 2 months after discharge. It identified a single episode of ventricular tachycardia that lasted for 10 beats, and prompted a request for transthoracic echocardiography (TTE). She suffered a minor posterior circulation stroke a week before the TTE, which subsequently identified a 2×1 cm mobile structure on the aortic valve (Figs 1 and 2).

Transthoracic echocardiography showing the fibroelastoma (white arrow) on the right coronary cusp. a) Parasternal long axis view. b) Modified four-chamber apical view. c) Normal Doppler velocity across the valve. d) Parasternal short axis view.
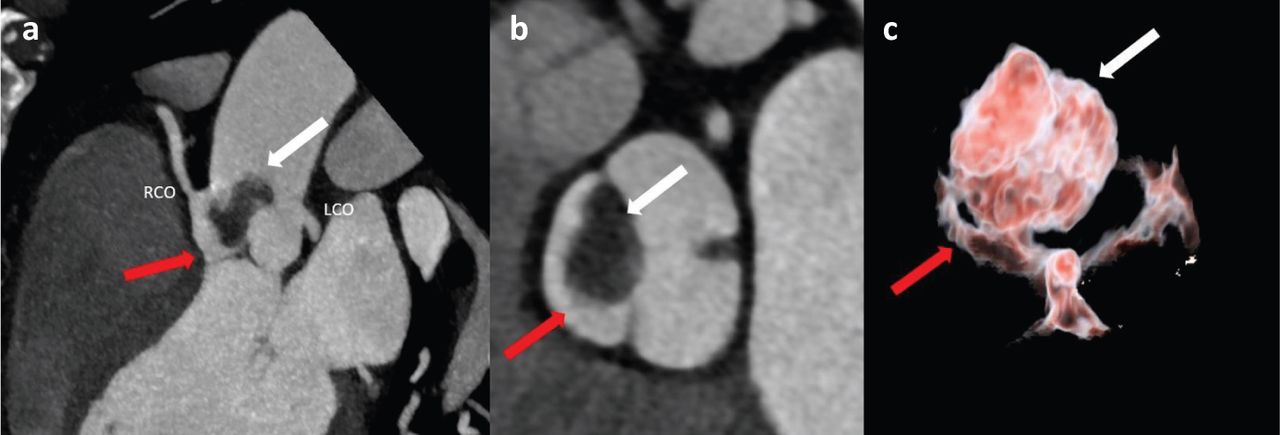
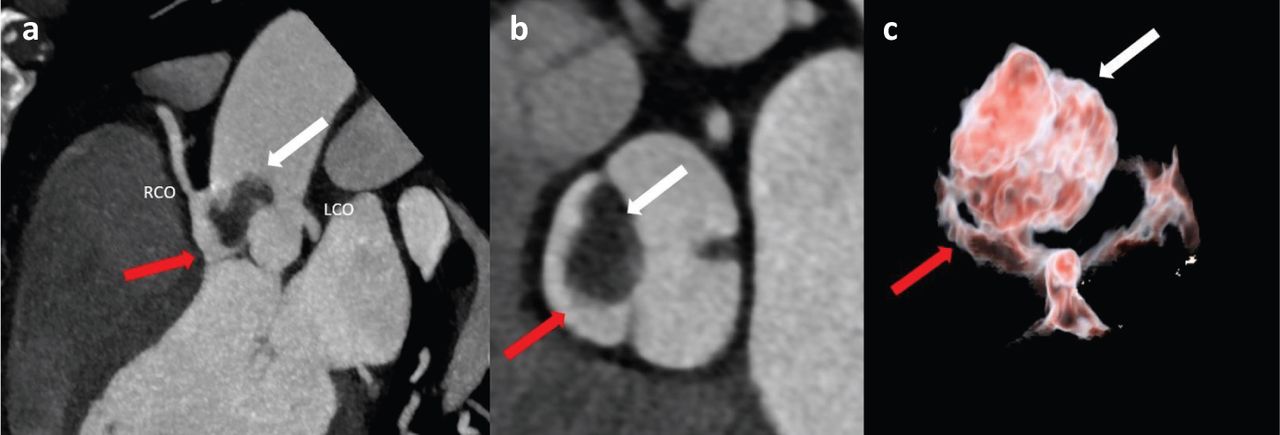
Computed tomography showing fibroelastoma (white arrow) and right aortic valve cusp (red arrow). a) Maximum intensity projection of the aortic valve showing left coronary artery ostia (LCO) and right coronary artery ostia (RCO). b) Maximum intensity projection through the aortic valve plane. c) 3D volume rendering technique of the aortic valve showing the three cusps, and the attachment of the fibroelastoma to the right coronary cusp.
The patient was admitted directly to the coronary care unit for further investigation. Repeat inflammatory markers and three sets of blood cultures were normal. A CT cardiac coronary angiography did not show any evidence of coronary artery disease, but confirmed that the mass was attached to the anterior leaflet of the aortic valve extending into the supravalvular aorta (Fig 1).
She was transferred to a tertiary centre for surgical resection of the mass. Subsequent histology had identified it as a fibroelastoma (Fig 3). Repeated TTE 2 years post-surgical removal showed no evidence of recurrence of the fibroelastoma with preserved left ventricular systolic function and mild aortic regurgitation.
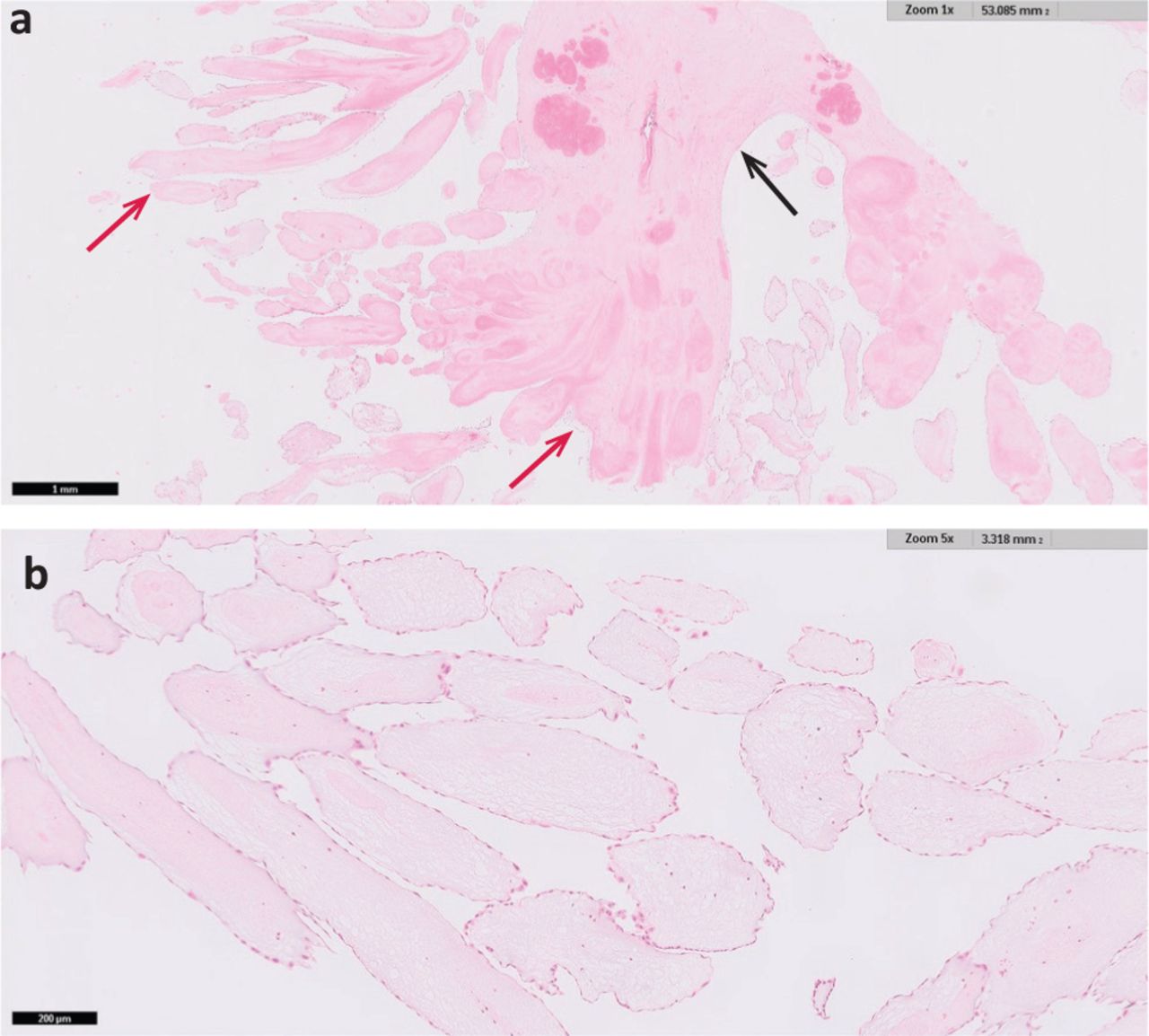
Haematoxylin and eosin stain of papillary fronds. a) Papillary fronds (red arrows) arising from a central stalk (black arrow) at low magnification. b) Papillary fronds showing the fibroelastic core covered with bland endothelium at higher magnification.
Discussion
Our case demonstrated cerebral embolisation secondary to a CPF, a rare cause of stroke and successful treatment with reperfusion therapy. CPFs are benign tumours, accounting for <10% of all cardiac tumours but the most common type of valvular tumour.1,2 The majority of CPFs are found at the aortic valve, with the left ventricle as the most common non-valvular site.3–5 The mean age of onset was 66 years and the size ranged from 4–70 mm.6 It has a sea anemone-like appearance macroscopically, and microscopic examination reveals an avascular frond formed by a fibroelastic core with spindle cells and an endocardial covering.5
CPFs are usually found incidentally, but have presented in a number of ways, including transient ischaemic attack/stroke, heart failure and even sudden death.5 In this case, the patient's ventricular tachycardia is postulated to be secondary to the CPF, perhaps due to cardiac ischaemia caused by obstruction of the blood supply to the coronary arteries.6 Conversely, right-sided tumours are often asymptomatic until sizeable enough to restrict intracardiac flow or induce arrhythmias.4 CPF has a 1.6% risk of recurrence after resection, and requires regular postoperative surveillance.6
Along with this case, a detailed search of PUBMED and EMBASE revealed 11 additional cases (supplementary material S1) that had described good outcomes with patients undergoing reperfusion therapy in strokes secondary to CPFs.2,3,8–14 However, all but one had a histological examination of the retrieved clot that confirmed a fragment of the tumour, and hence one could not exclude the possibility that some of the embolised clots in these studies contained predominantly thrombus rather than the tumour material, which could in turn explain the good prognosis.11 Once identified, CPFs should be removed as soon as possible due to the risk of recurrent embolic events, while balancing the increased risk of bleeding during cardiopulmonary bypass.4,6 Other modifiable risk factors for stroke should also be adequately treated.
Clinicians are increasingly aware of the importance of detection of paroxysmal atrial fibrillation after transient ischaemic attack and stroke but the clinical utility of echocardiography is uncertain.15 Despite that, the Royal College of Physicians’ stroke guideline has recommended TTE in patients with transient ischaemic attack or stroke who have clinical or electrocardiographic features of structural cardiac disease, and in those with undetermined aetiology especially if brain imaging is supportive of cardioembolism.16 One could even speculate that this patient's recurrent stroke might have been potentially preventable with faster completion of cardiac investigations.
Conclusion
CPF is the most common cardiac tumour and has high risk of cerebral embolisation. Patients with a known CPF should not be considered a contraindication to thrombolysis or thrombectomy and tend to have a good outcome after such therapies. Cardiac investigations should be completed early in stroke patients with undetermined aetiology.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Summary of search of PUBMED and EMBASE revealing 11 additional cases that describe good outcomes with patients undergoing reperfusion therapy in strokes secondary to cardiac papillary fibroelastomas.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
{kind=link}
{kind=link}