
Article Figures & Data
Figures
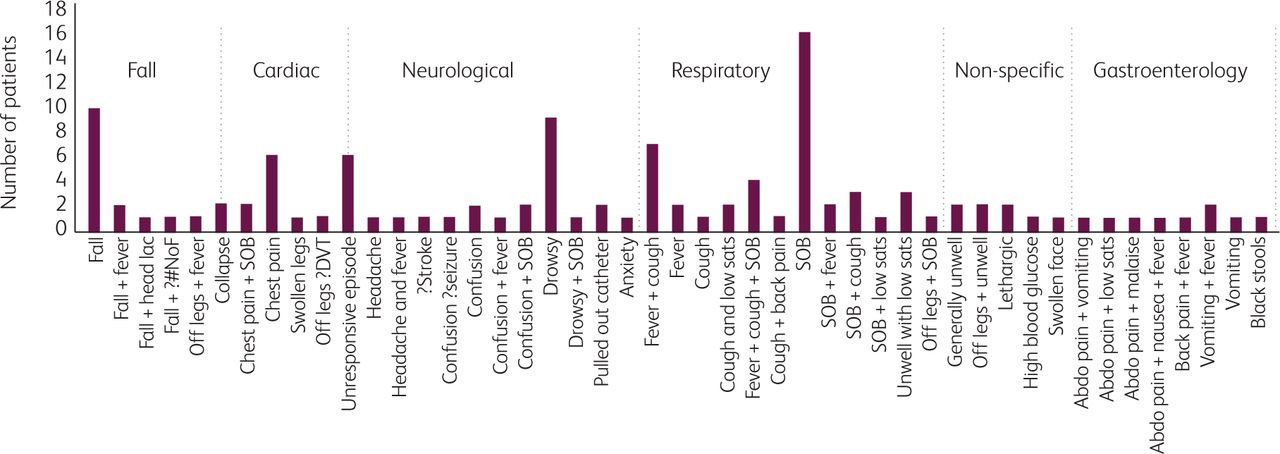
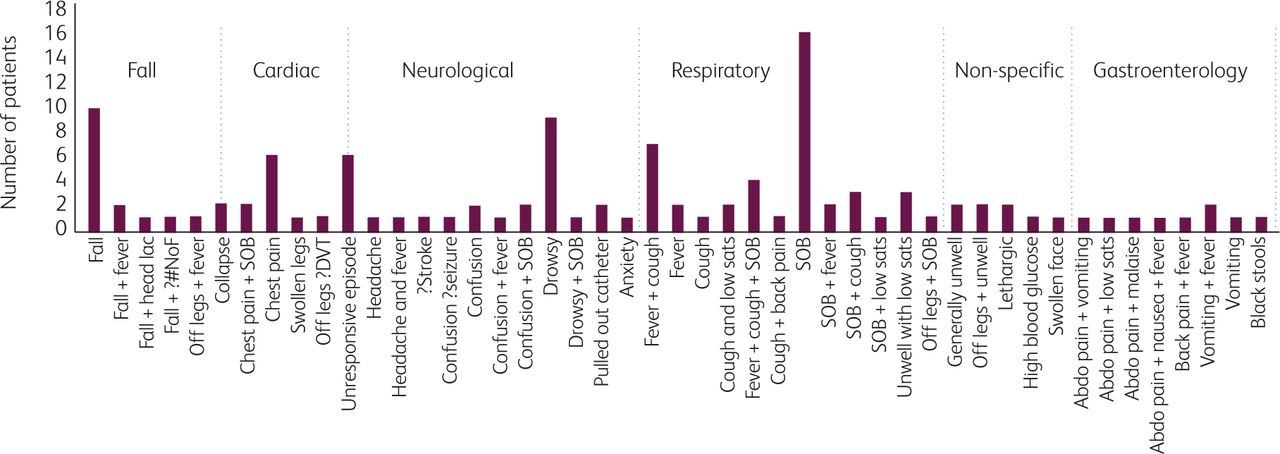
- Fig 1.
Reason for presentation to hopsital, according to emergency department triage records. Abdo = abdominal; DVT = deep vein thrombosis; lac = laceration; #NoF = fractured neck of femur; SOB = shortness of breath.
- Fig 2.
Example temperature traces, showing three patients with either high temperature spikes, high and low temperature spikes or only low temperature spikes.
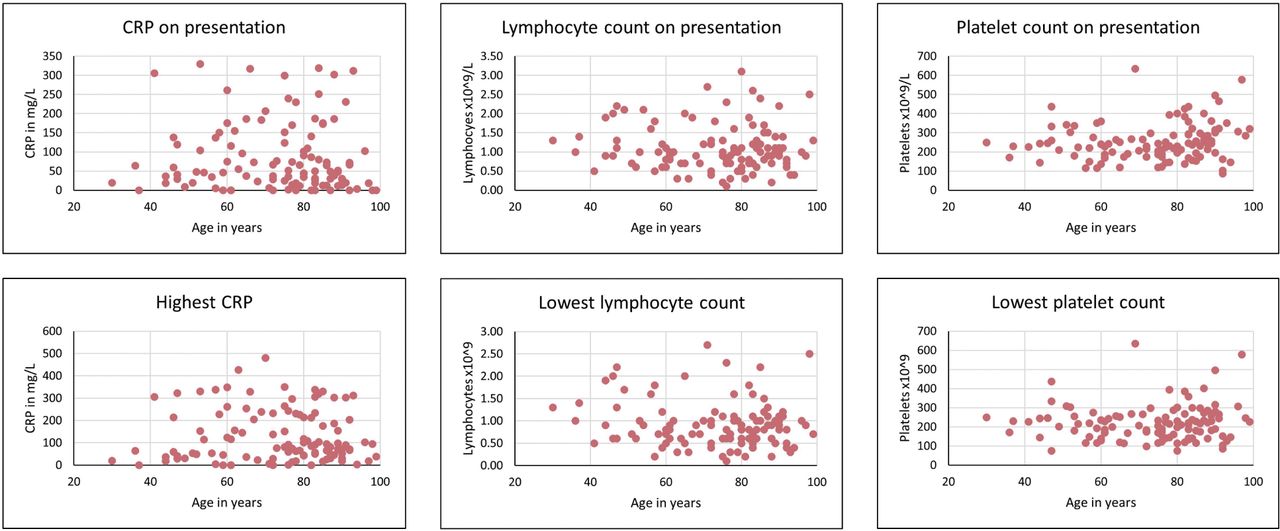
- Fig 3.
Key laboratory parameters across the age range.


Tables
What is already known? Much speculation has centred on the topic of where COVID-19 cases come from late into lockdown, but little is published to inform this debate. Similarly, while several large patient cohorts have been reported by various countries around the world, little attention has been paid to whether the presentation of COVID-19 may vary in the elderly, who represent the group most likely to be seriously affected. What is the question? We therefore sought to assess the epidemiological question of where cases continue to come from in weeks 5 and 6 of lockdown, and the diagnostic question of whether presentations of COVID-19 differ in the elderly. What was found, and implication for practice now? The majority of cases of COVID-19 late in lockdown are epidemiologically linked to contact with health and care services, including carers visiting people at home, which is an important public health consideration for ongoing pandemic planning. COVID-19 can present differently in the elderly, overlapping with many common medical presentations, so focusing testing on those with a cough or fever will miss at least 1 in 3 cases in those over the age of 70. - Table 1.
Cohort demographics and epidemiology of infection with coronavirus-19 in weeks 5 and 6 of lockdown in the UK
Characteristic Whole cohort (N=115) Under 70(n=40) Aged ≥70 (n=75) Baseline demographics Median age in years, interquartile range 77.5, 51–86 57.5, 47–61 84, 78–89 Male 66 (57.4) 30 (75) 36 (48)* Epidemiological factors Previous hospitalisation within 28 days 22 (19.1) 4 (10.0) 18 (24) Admitted from a care home 46 (40.0) 8 (20.0) 38 (50.7)* Carers at own home 18 (15.7) 2 (5) 16 (21.3)* Works/household works in healthcare 6 (5.2) 5 (12.5) 1 (1.3)* One of following applies: recent admission/care home/carers/health work 81 (70.4) 17 (42.5) 64 (85.3)* Documented household transmission 3 (2.6) 3 (5) 1 (1.3) Working (non-healthcare) 4 (3.5) 4 (10) 0 (0)* Community (unidentified source) 14 (12.2) 16 (35) 10 (13.3)* Comorbidities Hypertension 50 (43.5) 16 (40) 34 (45.3) Type 2 diabetes mellitus 38 (33.0) 14 (35) 24 (32) Ischaemic heart disease 29 (25.2) 5 (12.5) 24 (32)* Dementia 28 (24.3) 2 (5) 26 (34.7)* Chronic obstructive pulmonary disease 19 (16.5) 4 (10) 15 (20) Chronic kidney disease 18 (15.7) 3 (7.5) 15 (20) Stroke or TIA 14 (12.2) 2 (5) 12 (16) Cancer 11 (9.6) 2 (5) 9 (12) Asthma 7 (6.1) 3 (7.5) 4 (5.3) No comorbidities 8 (7.0) 7 (17.5) 1 (1.3)* Values are numbers (percentages) unless stated otherwise.
↵*p <0.05, comparing the <70 and ≥70 groups.
- Table 2.
Presenting symptoms and signs, along with temperature during hospital admission, in patients diagnosed with COVID-19 in weeks 5 and 6 of lockdown in the UK
Presenting symptoms Whole cohort (N=115) Under 70(n=40) Aged ≥70 (n=75) Fever (or reported chills) or cough 82 (71.3) 33 (82.5) 49 (65.3) Cough 59 (51.3) 27 (67.5) 32 (42.7)* Fever or reported chills 66 (57.4) 26 (65) 40 (53.3) Shortness of breath 61 (53.0) 24 (60) 37 (49.3) One of cough, fever or shortness of breath 92 (80) 36 (90) 56 (74.7) All of cough, fever and shortness of breath 32 (27.8) 16 (40) 16 (21.3)* Chest pain 21 (18.3) 10 (25) 11 (14.7) General malaise/off food 32 (27.8) 11 (27.5) 21 (28) Nausea/vomiting 16 (13.9) 6 (15) 10 (13.3) Diarrhoea 19 (16.5) 7 (17.5) 12 (16) Abdominal pain 14 (12.2) 5 (12.5) 9 (12) One of diarrhoea/nausea/abdominal pain 35 (30.4) 17 (42.5) 18 (24)* Confusion 20 (17.4) 3 (7.5) 17 (22.7)* Drowsiness 14 (12.2) 2 (5) 12 (16)* Fall 22 (19.1) 6 (15) 16 (21.3) Presenting signs High fever ≥38.0°C 36 (31.3) 15 (37.5) 21 (28) Low grade fever 37.5–37.9°C 11 (9.6) 6 (15) 5 (6.7) Normal temperature 36.0–37.4°C 52 (45.2) 16 (40) 36 (48) Low temperature ≥35.5°C 12 (10.4) 1 (2.5) 11 (14.7)* Average oxygen saturations 92% 89% 93% During hospital stay ≥38.0°C (high-grade fever) 61 (53.0) 26 (65) 35 (46.7) ≥37.5°C (fever) 79 (68.7) 31 (77.5) 48 (64) 36.0–37.4°C (normal) 25 (21.7) 3 (7.5) 22 (29.3)* ≥35.5°C (low temperature) 54 (47.0) 7 (17.5) 47 (62.7)* ≥35.5°C and never ≥38.0°C 24 (20.9) 4 (10) 20 (26.7)* Values are numbers (percentages) unless stated otherwise.
↵*p<0.05, comparing the <70 and ≥70 groups.
Laboratory investigation Under 70 survivors Under 70 died Over 70 survivors Over 70 died Lymphocyte count on presentation ×109/L
(NR 1.4–4.8)1.0
(0.73–1.3)1.0
(0.58–1.93)0.95
(0.7–1.3)1.0
(0.78–1.33)Lowest lymphocyte count ×109/L 0.9
(0.6–1.3)0.7
(0.5–0.9)0.8
(0.6–1.0)0.9
(0.63–1.13)Platelet count on presentation ×109/L
(NR 150–400)244.5
(180.75–273)225.5
(181–231.25)225.0
(180.5–288.5)289*
(242.5–395.75)Lowest platelet count ×109/L 235.5
(173–256.5)191
(145.5 – 226.5)197.0
(147.5–256)236.5
(187–273)White cell count on presentation ×109/L
(NR 4.0–11.0)6.25
(5.28–8.93)8.9
(7.0–12.1)8.7
(6.7–12.35)13.1*
(9.1–15.65)Highest white cell count ×109/L 7.05
(5.6–12.3)13.15*
(11.18–17.53)9.85
(7.0–14.38)14.05*
(13.18–19.55)CRP on presentation mg/L (NR<5) 57.0
(30.25–133.25)126.5*
(66.25–196.5)58.0
(25.75–101.75)49.0
(30–207)Highest CRP mg/L 61.5
(37.25–223.75)232.5*
(115.5–314.0)80
(50.0–214.0)96
(54.25–217.5)Values are median (interquartile range). CRP = C-reactive protein; NR = normal range.
↵*p<0.05, comparing those who survived to those who died within each age-group cohort.
Characteristic Whole cohort Under 70 Aged ≥70 CXR (9 did not have a CXR) No consolidation 37 (34.9) 12 (31.6) 25 (36.7) Unilateral consolidation 23 (21.7) 6 (15.7) 17 (25.0) Bilateral consolidation 43 (40.5) 20 (52.6) 23 (33.8) Outcome Discharged 87 (75.7) 31 (77.5) 56 (74.7) Died 28 (24.3) 9 (22.5) 19 (25.3) Died 30–39 (n=3) 0 Died 40–49 (n=9) 1 (11.1) Died 50–59 (n=13) 3 (23.1) Died 60–69 (n=15) 5 (33.3) Died 70–79 (n=22) 2 (9.1) Died 80–89 (n=35) 9 (25.7) Died 90–99 (n=18) 8 (44.4) Values are numbers (percentages). n represents the total number of patients in each age group. CXR = chest radiograph.








{kind=link}
{kind=link}
{kind=link}