
Introduction
Acute kidney injury (AKI) is common in hospitalised patients and provides valuable prognostic information, although there is suggestion of negligible mortality difference between AKI stages 2 and 3.1,2 AKI stage is principally determined by proportional serum creatinine (SCr) changes, not by absolute values. We hypothesised that establishing prognostic differences within and between AKI stages can be improved by using peak SCr (pSCr) values as well as proportional change. To address a secondary aim, we compared prognosis based on pSCr between patients with AKI and those with chronic kidney disease (CKD). This was to determine whether the outcome for any given SCr is worse in AKI or CKD.
Methods
Anonymised data for all adult inpatient episodes at Salford Royal Hospital from March 2014 to August 2018 were acquired as previously described.3 Exclusion criteria were: pregnancy, renal transplant, maintenance dialysis, transfers for tertiary nephrology care, insufficient SCr data. AKI events were determined using the NHS England algorithm.4 pSCr for each hospital episode was classified as ≤100, 101–200, 201–300, 301–400 or >400 μmol/L. Odds ratio (OR) for in-hospital death was determined for each pSCr category against a reference group of no AKI and pSCr ≤100 μmol/L, using binary logistic regression adjusted for age, gender and ICD-10 coded comorbidities. Results were compared between AKI stages and CKD status.
Results
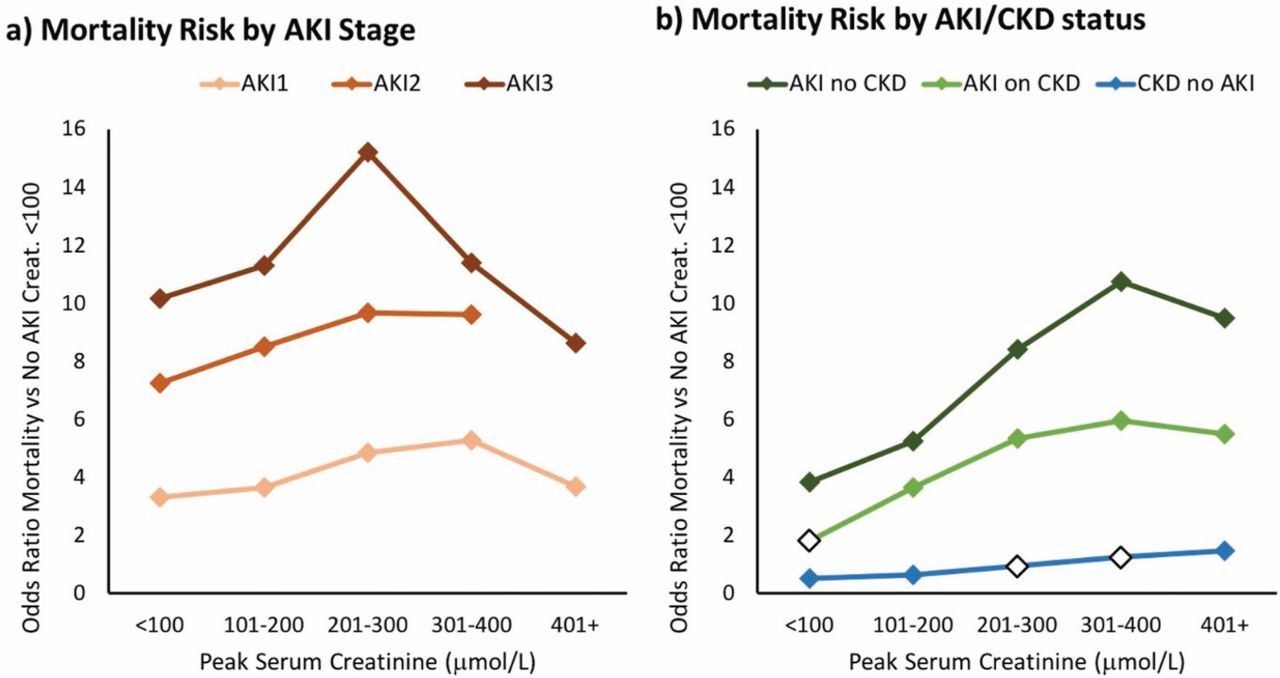
There were 163,428 inpatient episodes, of which 21,545 were excluded. Of 141,883 included episodes (52.6% female; mean age 56.5±22.1 years; CKD 5.9%; inpatient death 3.8%), 9.8% were complicated by AKI. Highest AKI stage was one in 9,339 (6.6%), two in 2,614 (1.8%) and three in 1,882 (1.3%). Table 1 displays the number of admissions, AKI and deaths in each pSCr classification, categorised by AKI stage and CKD status. Fig 1 displays the OR for mortality between pSCr categories. Mortality risk generally rose with increasing pSCr, and there was a greater risk with advancing AKI stage. The highest mortality risk was in AKI stage 3, pSCr 201–300 μmol/L (OR 15.22 (confidence interval 11.71–19.77); p<0.001). Of note, mortality risk was lower for pSCr >400 μmol/L in patients with AKI stages 1 (OR 3.70 (2.11–6.51); p<0.001) and 3 (OR 8.65 (7.19–10.41); p<0.001) compared with categories 201–300 and 301–400 μmol/L. In AKI stage 3, pSCr >400 μmol/L had the lowest OR across the range of pSCr, including pSCr ≤100 μmol/L (OR 10.18 (5.65–18.36); p<0.001). Sub-analyses showed that overall adjusted mortality risk was significantly higher in AKI stage 3 vs 2 (OR 1.25 (1.09–1.44); p=0.001), although when assessed across pSCr categories this was not significant at extremes. In patients with CKD, AKI was associated with significantly higher mortality across pSCr levels.

Mortality risk by peak serum creatinine. A blank marker denotes that this odds ratio is not significant (p>0.05); all other results are significant (p>0.05).
Admissions and deaths in peak serum creatinine categories
Conclusion
Mortality risk is high in hospital episodes complicated by AKI and risk increases proportionately with AKI stage and pSCr, except in patients with pSCr >400 μmol/L. For a given pSCr, AKI carries significantly greater mortality risk than CKD. The absolute value of SCr has relevance for prognosis during inpatient AKI episodes, beyond that indicated by AKI stage alone.
Conflicts of interest
None declared.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.