
Background
Forty per cent of patients undergoing angiography to investigate exertional chest pain have normal coronary arteries. While described for nearly half a century, this condition has remained a mechanistic enigma.1–2 Diminished coronary blood flow augmentation to a pharmacological vasodilator, or coronary microvascular dysfunction (MVD), portends a greater risk of major adverse cardiovascular events.3–4 However, patients report symptoms during physical exercise, and the response to pharmacological ‘stress’ and physical exercise differ in the healthy heart.5 Moreover, it is unclear whether MVD is confined to the coronary circulation or a generalised disorder in myocardial and systemic blood flow during stress.
Aims
To identify whether patients with MVD have abnormal coronary blood flow during physical exercise, generalised systemic endothelial dysfunction and abnormal global myocardial blood flow during stress.
Method
Patients with angina and unobstructed coronary arteries underwent simultaneous acquisition of intra-coronary pressure and flow during rest, supine bicycle exercise and pharmacological vasodilatation with adenosine (hyperaemia), in the catheter laboratory. Coronary flow reserve (CFR) was calculated as hyperaemic coronary blood flow (CBF) / resting CBF.6 Wave intensity analysis quantified the proportion of accelerating wave energy (perfusion efficiency), a measure of the dynamic interaction between the contracting myocardium and interweaving coronary vasculature during the cardiac cycle, or cardiac–coronary coupling.5 Forearm blood flow ratio (FBF) was assessed to acetylcholine and NG-monomethyl-L-arginine (L-NMMA) infusions, an endothelial-dependent dilator and nitric oxide synthase inhibitor.7 Global myocardial blood flow and subendocardial:subepicardial perfusion ratio (endo/epi) were quantified using 3-Tesla cardiac magnetic resonance imaging (MRI) during hyperaemia and rest; inducible ischaemia was defined as hyperaemic endo/epi<1.0.8 Myocardial perfusion reserve (MPR) was calculated as hyperaemic myocardial blood flow / resting myocardial blood flow.9 Patients were classified as having MVD if CFR<2.5 and controls if CFR≥2.5, with researchers blinded to the classification.10
Results
A total of 95 patients were enrolled (57±10 years, 81% women); 52 were classified as having MVD and 43 as controls. Microvascular resistance (MR) and CBF during peak exercise were similar in MVD and controls (4.5±1.6 vs 4.7±1.6 mmHg/cm/s and 30±10 vs 27±8 cm/s; p=0.68 and p=0.15). However, patients with MVD had higher systolic blood pressure and rate–pressure product (172±29 vs 155±29 mmHg and 20,486 vs 17,550 beats per minute*mmHg; both p=0.02). From rest to stress coronary perfusion efficiency improved in controls, whereas a paradoxical reduction occurred in those with MVD (59±11% to 65±14%; p=0.02 vs 61±12% to 44±10%; p<0.001; Fig 1). Patients with MVD had attenuated FBF augmentation to acetylcholine and exaggerated reduction to L-NMMA (3.6±1.8 vs 4.5±2.0 and 0.53±0.14 vs 0.78±0.09; p=0.02 and p<0.001). Those with MVD had a higher rate of inducible myocardial ischaemia and reduced MPR (22% vs 82% and 2.0±0.4 vs 2.7±0.5; both p<0.001).
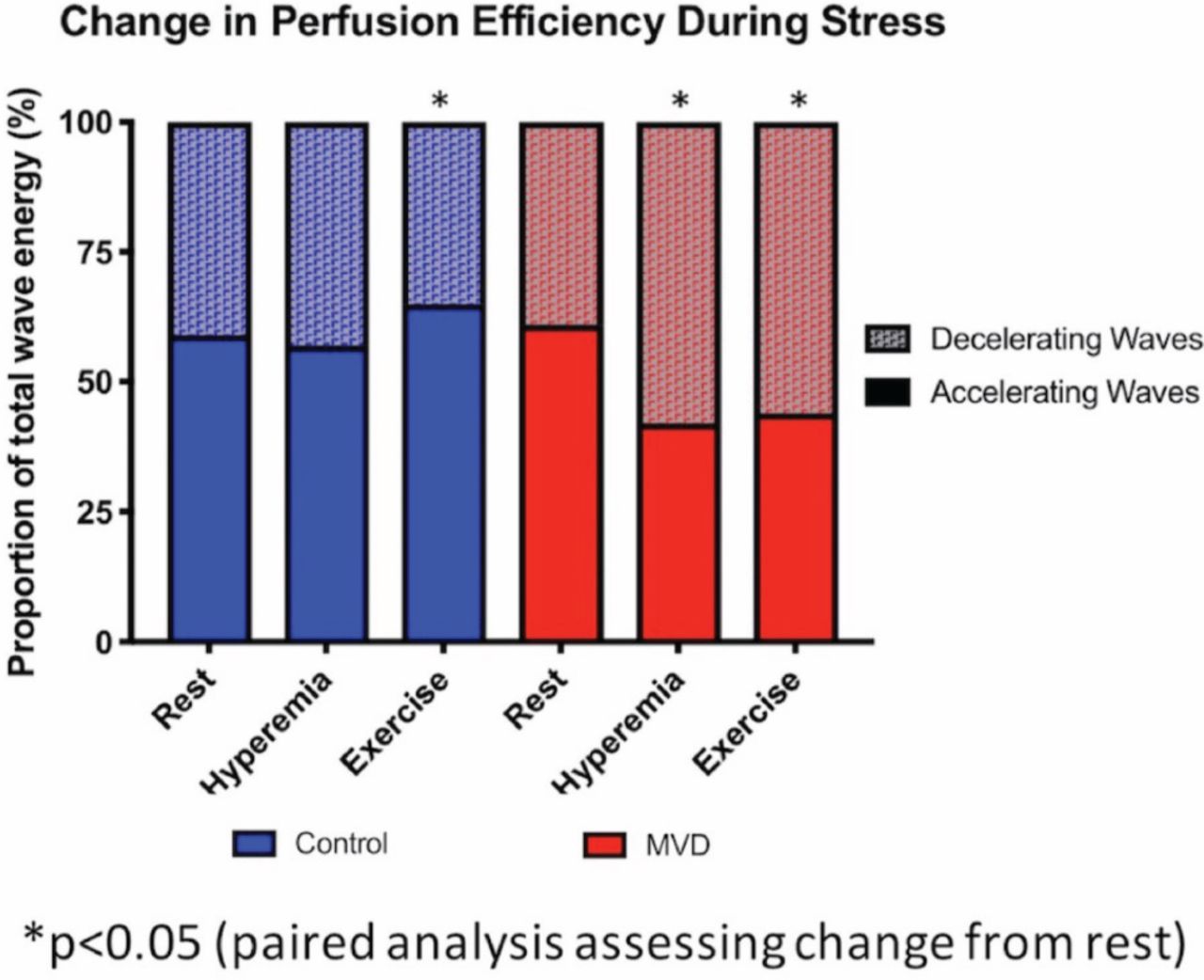
Changes in coronary perfusion efficiency (a measure of cardiac–coronary coupling) from rest to stress. MVD = microvascular dysfunction.
Conclusions
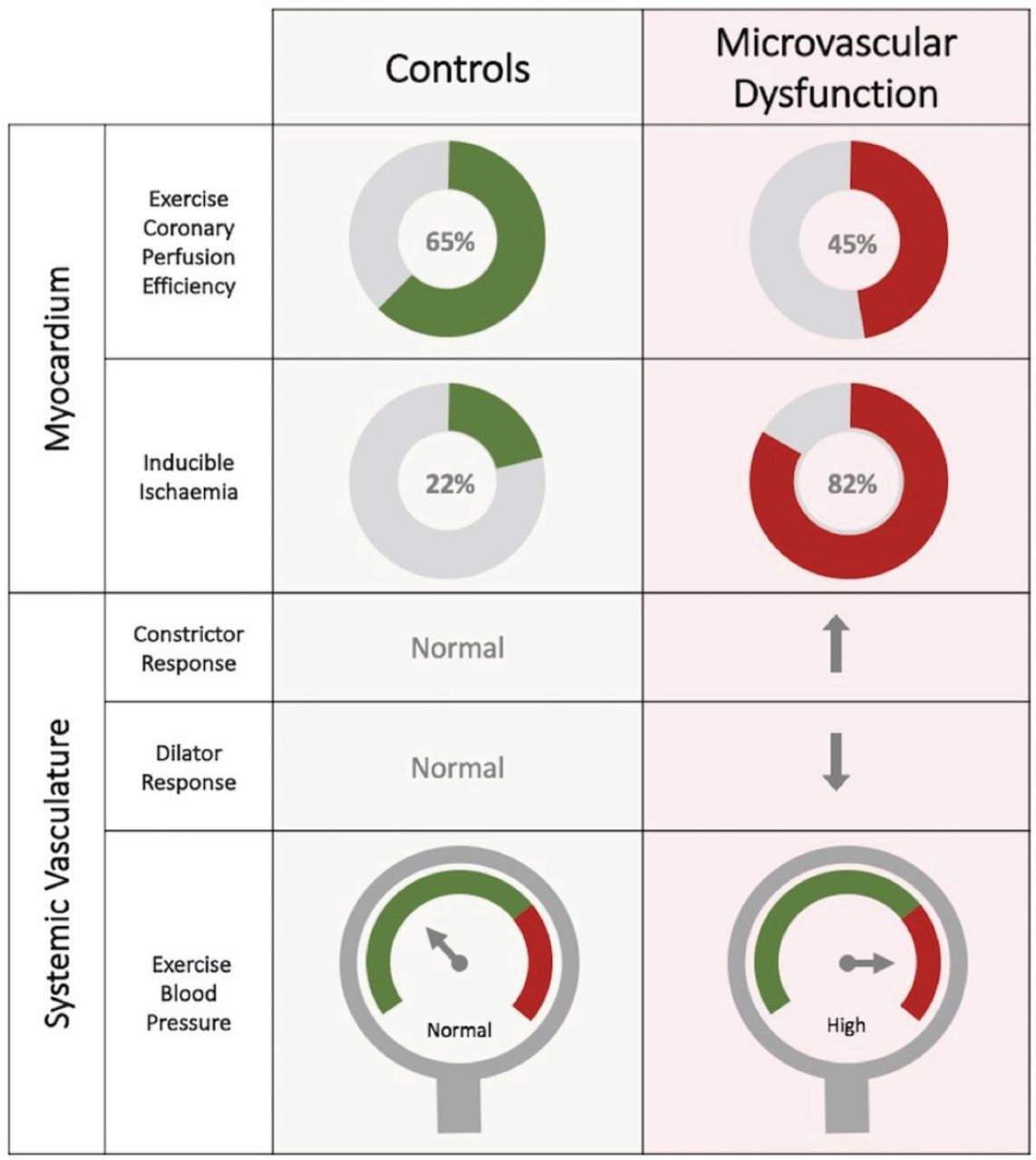
Compared with controls, MVD is associated with abnormal cardiac–coronary coupling during exercise, systemic endothelial dysfunction and hypertension with resultant increased myocardial oxygen demand. These pathophysiological changes act in concert to produce global myocardial ischaemia during stress and may underlie the higher incidence of cardiovascular morbidity observed in this population (Fig 2). The nitric oxide synthase pathway may represent a novel therapeutic target and should be the subject of future work; currently no disease-modifying therapy exists specifically for MVD.
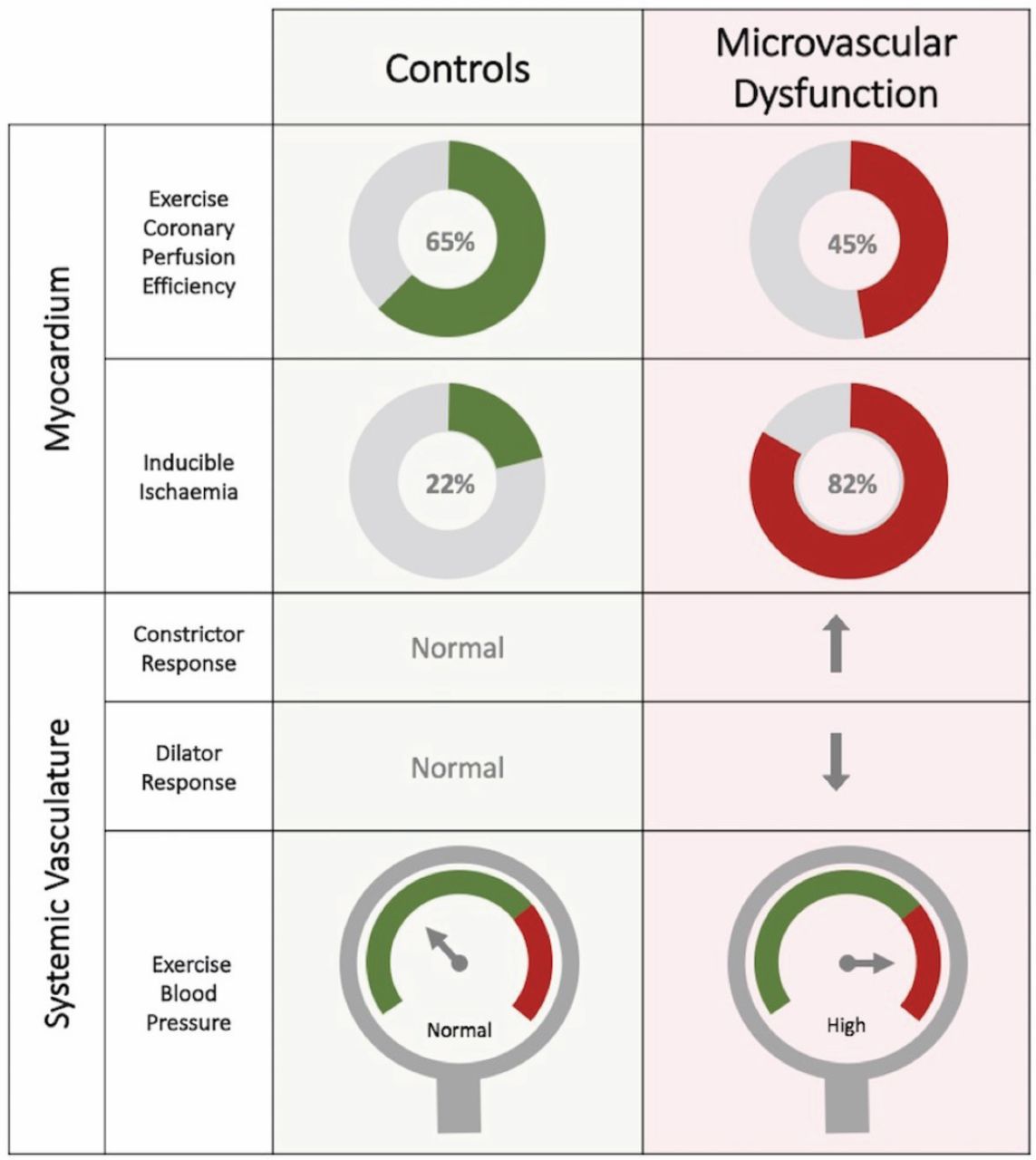
Summary of cardiac and systemic responses to stress in microvascular dysfunction compared with controls.
Conflicts of interest
None declared.
- © Royal College of Physicians 2020. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.