
ABSTRACT
Background Fibromyalgia and myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) are poorly understood conditions with overlapping symptoms, fuelling debate as to whether they are manifestations of the same spectrum or separate entities. Both are associated with hypermobility, but this remains significantly undiagnosed, despite impact on quality of life.
Objective We planned to understand the relevance of hypermobility to symptoms in fibromyalgia and ME/CFS.
Method Sixty-three patient participants presented with a confirmed diagnosis of fibromyalgia and/or ME/CFS; 24 participants were healthy controls. Patients were assessed for symptomatic hypermobility.
Results Evaluations showed exceptional overlap in patients between fibromyalgia and ME/CFS, plus 81% met Brighton criteria for hypermobility syndrome (odds ratio 7.08) and 18% met 2017 hypermobile Ehlers–Danlos syndrome (hEDS) criteria. Hypermobility scores significantly predicted symptom levels.
Conclusion Symptomatic hypermobility is particularly relevant to fibromyalgia and ME/CFS, and our findings highlight high rates of mis-/underdiagnosis. These poorly understood conditions have a considerable impact on quality of life and our observations have implications for diagnosis and treatment targets.
Introduction
Fibromyalgia and myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) have overlapping symptoms. All physicians will be facing the challenge of assessing possible ‘post-viral fatigue’ in the wake of COVID-19. Fibromyalgia is a common, poorly understood, complex musculo-skeletal disorder that affects around 5% of the UK population.1 It is polysymptomatic yet marked primarily by chronic widespread pain, typically believed to be non-inflammatory in nature. In addition, patients frequently report extra-musculoskeletal symptoms, including both physical and emotional fatigue with subjective cognitive dysfunction (‘fibrofog’).2 For quality of life, patients with fibromyalgia score significantly lower than the general population, or patients with other musculo-skeletal disorders (such as rheumatoid arthritis, osteoarthritis and systemic lupus erythematosus) on all eight health status domains.2,3 Pain, fatigue, subjective cognitive impairment and psychological disturbance (eg depression and anxiety) have greatest impact on quality of life. Thus, pain and fatigue are identified as among the most disabling symptoms associated with fibromyalgia. Relatedly, pain is also frequently reported in ME/CFS.4 Complexity of understanding their origins may have contributed at times to consideration of both fibromyalgia and ME/CFS as functional somatic, medically unexplained or somatisation disorders. The presence of shared symptoms in brain and body has also fuelled debate as to whether fibromyalgia and ME/CFS are manifestations of the same spectrum disorder or separate clinical entities.5,6 Although the dominant symptom of fibromyalgia is pain and ME/CFS is disabling fatigue or post-exertional malaise, patients with either diagnosis typically experience pain (including hyperalgesia and central sensitisation), fatigue, sleep problems and cognitive difficulties.6 Altered inflammatory markers and dysautonomia are reported in both fibromyalgia and ME/CFS, calling into question their perceived status as ‘functional’ disorders.7–10 Moreover, it is increasingly recognised that fibromyalgia and ME/CFS are associated with joint hypermobility, an expression of variant connective tissue.11–14
Joint hypermobility (a feature of Ehlers–Danlos syndromes (EDS)) is common and associated with many extra-articular features.15,16 Internationally, there is little agreement on the precise definition of measurement and hypermobility, nor the point at which it constitutes a disorder. In 2017, a consensus group sought to re-classify Ehlers–Danlos syndrome – hypermobility type (EDS-HT). As a consequence, the terms hEDS (hypermobile EDS) and hypermobility spectrum disorder (HSD) now refer to symptomatic joint hypermobility.17 An earlier term, joint hypermobility syndrome (diagnosed by revised Brighton criteria) was made redundant and was previously deemed indistinguishable from EDS-HT.18,19 However, one important distinction is that the revised Brighton criteria took into account historical joint hypermobility, whereas the newer criteria for hEDS rely on age and gender specific hypermobility cut-offs. There are commonalities in these criteria (including importance of widespread pain), but important differences in significance of Beighton (joint hypermobility) scoring, precise consideration of connective tissue and associated features and evaluation of family history (supplementary material S1). A broader concept of a HSD was introduced to describe the continuum that encompasses patients with symptomatic joint hypermobility through to people who do not meet full criteria for hEDS or related syndromes associated with joint hypermobility. However, this notion of a spectrum also remains controversial. Since there are no genetic tests available for hEDS, a clinical diagnostic checklist is available and consistent with the 2017 consensus criteria.17 Further research is required to validate clinical diagnostic criteria and international diagnostic codes, which presently are not consistent with newer nomenclature. In adults with hEDS/HSD, symptoms (including pain, fatigue, dysautonomic symptoms, poor coordination, attention/concentration deficits and low quality of life in general) can be also classified according to severity, reflecting neither the old nor new criteria for hEDS.20 Debate regarding diagnostic classification has intensified following a report on the prevalence of EDS and joint hypermobility syndrome (JHS) in primary care that suggests these diagnoses cannot be considered rare.21 Moreover, symptomatic hypermobility has considerable impact on quality of life, at least comparable or greater than those with other rheumatological diseases.22
The morbidity of hEDS/HSD to patients is most commonly expressed as complaints to clinicians of chronic musculoskeletal pain, headache and fatigue. These symptoms impair physical activity and quality of life, common to both fibromyalgia and ME/CFS. In rheumatology clinics, symptomatic hypermobility is estimated to contribute to nearly half of all outpatient appointments, but is only recognised one out of 19 times.14 Under-diagnosis of hEDS/HDS may exacerbate potentially disabling symptoms, complications and comorbidities, including autonomic dysfunction, fibromyalgia and ME/CFS.10,23 Enhanced recognition of symptomatic hypermobility is essential to improve function and quality of life in a patient group, whose symptoms are typically poorly understood and frequently overlooked.14 Accurate phenotyping of hEDS/HDS is needed for research, but it is also critical to effective multidisciplinary clinical management, from provision of accurate prognostic advice and identification of comorbidity to the offer of multiprofessional support and delivery of effective therapies. The relevance extends beyond rheumatology to other clinical contexts (eg cardiology, paediatrics, neurology, gastroenterology, pain management and mental health settings).
Aims of the study
The objective of this study was to understand the relevance of symptomatic hypermobility and related connective tissue variants to the expression of symptoms in fibromyalgia and ME/CFS. The study systematically tests associations between the diagnostic criteria for pain and fatigue symptom expression and further examines if specific subfactors within the diagnostic classifications of hypermobility predict clinical presentations.
Methods
This study is part of larger study investigating mechanisms of chronic pain and fatigue in fibromyalgia and ME/CFS (https://doi.org/10.1186/ISRCTN78820481) in adults. Here, we focus on the relevance of symptomatic hypermobility. All participants (patient participants and healthy controls) provided written informed consent and were compensated for their participation.) in adults. Here, we focus on the relevance of symptomatic hypermobility. All participants (patient participants and healthy controls) provided written informed consent and were compensated for their participation.
Patient and public involvement
The study idea was formed after patients and prior research participants discussed their lived experience of fibromyalgia and ME/CFS with the clinicians involved in the initial grant application.
Lay members of Arthritis Research UK critically reviewed the proposal and their suggestions incorporated into the proposal. A formal patient and public involvement panel reviewed the study after funding was obtained and advised on the study protocol and design, strategies for recruitment reflecting their priorities, experiences and preferences. Patients and public assessed the burden of testing and the time required to participate in the study.
Patients and public were involved in the promotion of the study through local support groups for patients living with fibromyalgia and ME/CFS.
Ethical approval was obtained from London – Brighton & Sussex Research Ethics Committee (REF:17/LO/0845). Patient participants with a clinical diagnosis of either fibromyalgia and/or ME/CFS were invited to be screened for the study.
To be included in the study, patients were required to either meet the American College of Rheumatology (ACR; 2010) diagnostic criteria for fibromyalgia and/or both the Canadian and Fukada criteria for ME/CFS as assessed at screening. Patients were recruited by advertisement from local support organisations for fibromyalgia and ME/CFS, local rheumatology clinics and via social media and bulletin boards. Inclusion criteria for healthy controls were a score no more than 3/10 on a pain visual analogue scale; a score of less than 36 on the fatigue severity scale and not meeting either the criteria for ACR diagnostic criteria for fibromyalgia nor the Canadian and Fukada criteria for ME/CFS; and be free of major psychiatric or neurological illness.
Healthy controls were also recruited via social media and bulletin boards. Neither patients nor controls were recruited/selected or screened on the basis of hypermobility and hypermobility assessors where unaware of clinical or screening disease specific research diagnostic information.
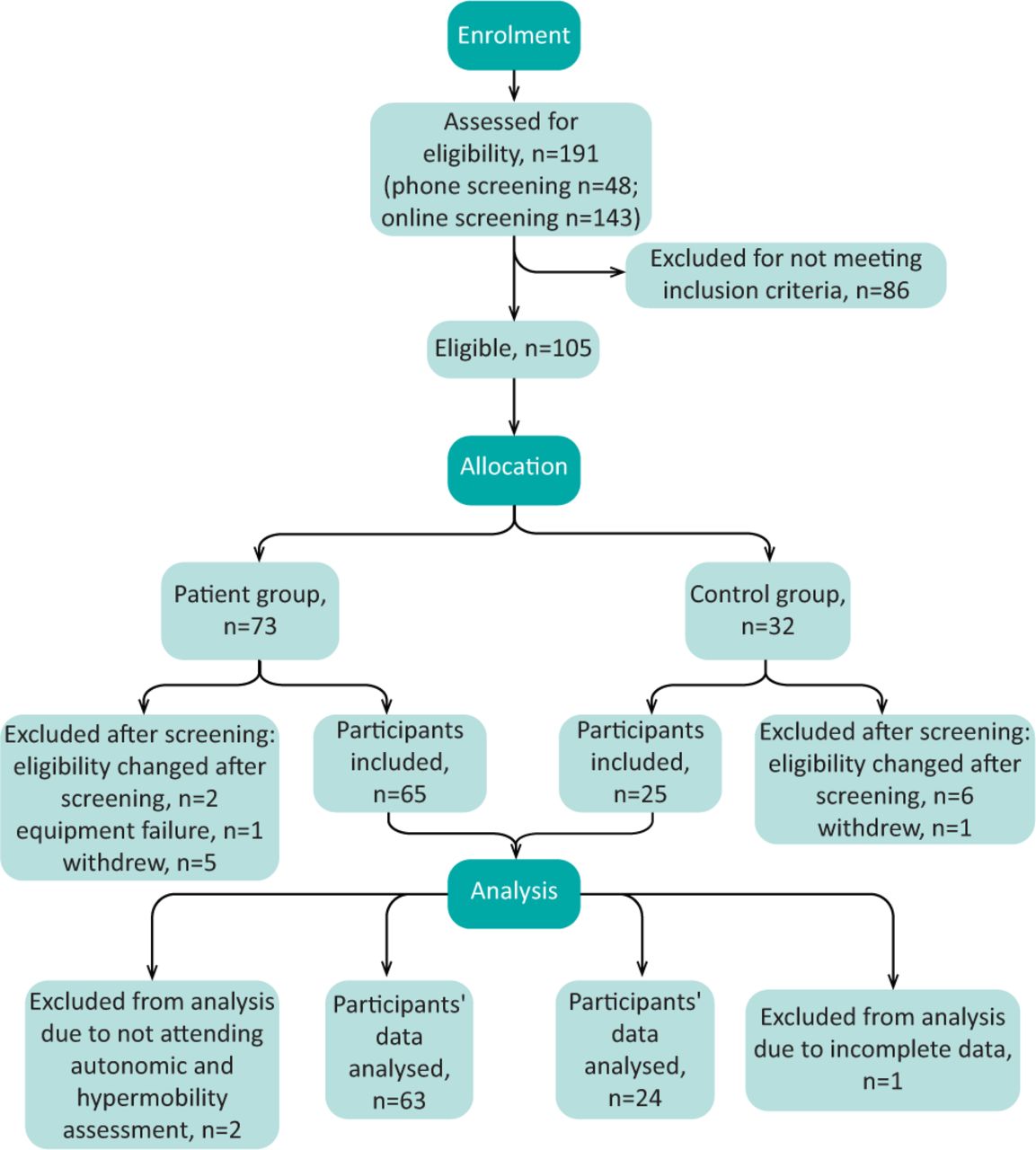
All participants who responded to advertisements were provided with more information. If they were willing to continue, there were screened via telephone or via anonymised online questionnaires for eligibility. Fig 1⇓ shows a CONSORT diagram detailing participant flow. Consenting participants completed a series of baseline questionnaires measuring subjective pain (McGill pain short form questionnaire); fatigue (fatigue impact, modified fatigue impact scale); brain-fog (mental clutter scale) and interoceptive sensibility (Porges body perception questionnaire).24 Demographic data was also collected and participants were assessed for presence of symptomatic hypermobility and variants of connective tissue by trained clinicians using the revised Brighton criteria and the 2017 hEDS classification criteria.14,17 It was not possible to determine the last item in criterion 2A (aortic root dilatation with Z-score >+2) as participants did not undergo echocardiography as part of the study protocol. Given the association between variant connective tissue and easy bruising, all participants where asked about this phenomenon independently.25 In total, 24 healthy controls were assessed alongside 63 patient participants. Where possible, controls were matched to age and gender of patient participants.

CONSORT diagram showing participant recruitment and flow through the study.
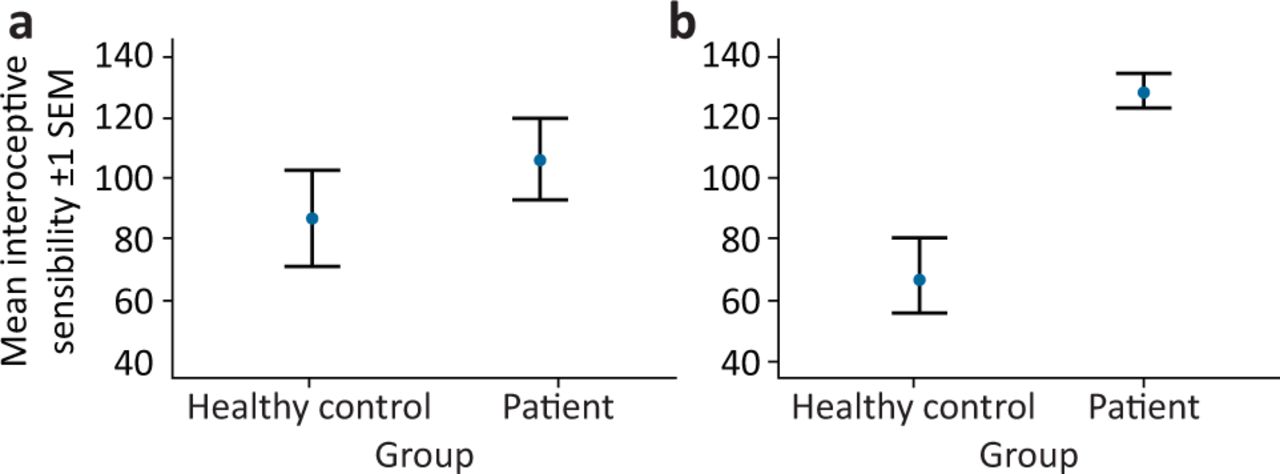
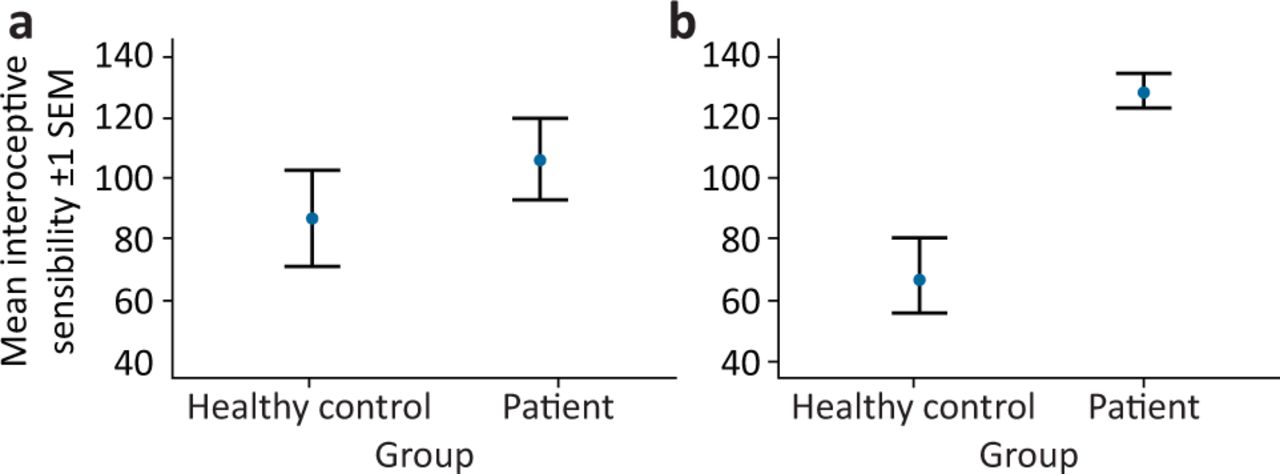
The significant interaction of meeting Brighton criteria for joint hypermobility syndrome on the association between patient group and interoceptive sensibility. a) Does not meet Brighton criteria for joint hypermobility syndrome. b) Meets Brighton criteria for joint hypermobility syndrome. SEM = standard error of the mean.
Data analysis and statistical methods
Each symptomatic hypermobility diagnostic classification (revised Brighton criteria for JHS; hEDS 2017 consensus criteria) were entered as binary variables. Further binary variables explored categorical elements of the different criteria. The Beighton scale and total number of major and minor criteria endorsed were expressed as scale data. Differences between groups in age and assessment outcomes were assessed via independent sample t-tests. Differences in sex and associations between groups were assessed via chi squared test. Binary logistic regression was used to derive prediction models for categorical variables, their odds ratios and their confidence intervals where appropriate. Univariate analyses (general linear model) were used to determine interactions. Spearman correlations were used to explore correlations with Beighton score. Hypothesis tests were considered statistically significant for p values <0.05 and all analyses were carried out using SPSS version 25 for Mac.
Results
Patient characteristics and diagnostic groups
Twenty-four healthy controls (nine male) and patients (12 male) did not differ significantly in age. Mean (standard error of the mean (SEM)) age of all healthy controls (39.3 years (2.7)) was not significantly different to the whole patient group (45.4 years (1.9)). There were no significant differences in sex.
Among the 63 patients, 20 (32%) presented with a clinical diagnosis of fibromyalgia; 24 (38%) presented with a clinical diagnosis of ME/CFS; and 19 (30%) presented with dual diagnoses of fibromyalgia and ME/CFS.
On research diagnostic evaluation, 56 (89%) met ACR diagnostic criteria for fibromyalgia, 59 (94%) met Canadian criteria for ME/CFS and 61 (97%) met Fukada criteria for ME/CFS. Strikingly, 52 (85%) patients met all three diagnostic criteria for fibromyalgia and ME/CFS. Seven (29%) healthy controls had generalised joint laxity as determined by Beighton score of four or more out of nine, compared with 29 (46%) in the patient group. Nine (37%) healthy controls met Brighton criteria, compared with 51 (81%) of the patient group. Two (8%) of healthy controls met 2017 hEDS criteria, compared with 11 (18%) of the patients. Across all participants meeting Brighton criteria, 13 (22%) endorsed a hEDS diagnosis. Of those assessed as having symptomatic hypermobility only 12 (23.5%) had received a diagnosis of hypermobility prior to evaluation in this study.
Relevance of symptomatic hypermobility to diagnosis
Beighton score
Across all participants, there were no associations between current (ie present) Beighton score and baseline pain, fatigue and interoceptive questionnaires.
Historical Beighton score (ie ever being able to perform the relevant manoeuvre) correlated (Spearman rank correlations) positively with total pain on McGill pain short form questionnaire (r=0.25; n=73; p=0.03), widespread pain index (derived from ACR diagnostic criteria; r=0.26; n=86; p=0.01), ACR symptom severity (r=0.27; n=85; p=0.01), fatigue impact (r=0.29; n=56; p=0.028), interoceptive sensibility (r=0.30; n=56; p=0.02).
There was a significant interaction of being a patient with fibromyalgia and/or ME/CFS compared with being a control on the relationship between historical Beighton score and McGill pain score (F=5.50; p=0.022); widespread pain index (F=36.87; p<0.001); ACR symptom severity (F=59.74; p≤0.001); fatigue severity scale (F=35.29; p≤0.001); fatigue impact (F=27.37; p≤0.001); modified fatigue impact scale (F=37.01; p≤0.001); mental clutter scale (F=15.72; p≤0.001; univariate general linear model). This means that the relationship symptoms and being a patient and control was significantly different according to hypermobility score.
Brighton criteria for joint hypermobility syndrome
Mixed fibromyalgia/ME/CFS
Meeting Brighton criteria significantly predicted membership of the patient group (odds ratio (OR) 7.08; p≤0.001; 95% confidence interval (CI) 2.50–20.00), and meeting both major criteria for the Brighton criteria was significantly associated with being a patient (chi squared 9.26; p=0.022).
Easy bruising was significantly associated with being a patient rather than a control (chi squared 4.10; p=0.043). No minor criteria were significantly predictive of group membership. There was a significant interaction of meeting Brighton criteria on the relationship between interoceptive sensibility and group membership (F=8.75; p=0.005).
Fibromyalgia
Endorsing both major criteria of Brighton criteria was significantly associated with an ACR fibromyalgia diagnosis (chi squared 6.53; p=0.01). ACR fibromyalgia was associated with easy bruising, (chi squared 7.58; p=0.006). No minor criteria were significantly predictive of fibromyalgia.
ME/CFS
Endorsing both major criteria of Brighton criteria was significantly associated with fulfilling Canadian criteria for ME/CFS (chi squared 7.58; p=0.006), as was endorsing Fukada criteria (chi squared 10.50, p=0.001). Easy bruising (chi squared 4.22; p=0.04) was associated with both Canadian criteria for ME/CFS and Fukada criteria (chi squared 5.71; p=0.017). No minor criteria were significantly predictive of ME/CFS.
Meeting all three diagnostic criteria (ACR, Canadian, Fukada)
Meeting Brighton criteria for JHS predicted meeting all three patient diagnostic criteria (p<0.001; OR 8.57; 95% CI 3.02–24.05).
hEDS 2017 diagnostic criteria
Mixed fibromyalgia and/or ME/CFS
A diagnosis of hEDS did not predict presence of fibromyalgia and/or ME/CFS, nor did individual elements of the diagnostic criteria.
Fibromyalgia
There were no associations between ACR definition of fibromyalgia and hEDS diagnosis or elements of the diagnostic criteria.
ME/CFS
Endorsing hEDS criterion 1 (age/sex adjusted Beighton score) significantly predicted presence of ME/CFS as defined by Canadian criteria (p=0.045; OR 3.07; 95% CI 1.01–9.28) and the Fukada criteria (p=0.031; OR 3.70; 95% CI 1.12–12.18). No other elements of the hEDS diagnostic criteria were significantly predictive.
Meeting all three diagnostic criteria (ACR, Canadian, Fukada)
A diagnosis of hEDS did not significantly predict meeting all three criteria. Neither did any diagnostic element.
Discussion
The strength of this research study is that it is the first clinical evaluation, to our knowledge, that incorporates and directly compares Brighton (JHS) and hEDS criteria. This study demonstrates the overlapping nature of fibromyalgia and ME/CFS within current diagnostic criteria, which remains controversial; fibromyalgia pain symptoms were recently reported in an overwhelming majority of patients with ME/CFS, the same authors also show high rates of generalized joint laxity in that population.5,6,13 This shared finding is perhaps not unsurprising given the presence of pain in the Canadian criteria for ME/CFS, however, no pain level is mandated, and pain is not required if symptoms started after an infection. Nomenclature and diagnostic classification of ME/CFS are subject to ongoing debate.26,27
Importantly we show the contribution of symptomatic joint hypermobility and variants of connective tissue disorder to both conditions and to associated level of symptoms. Although we use a wide variety of patient reported outcomes, and such subjective measures can be problematic, it is important to note the significant associations between historical hypermobility and key symptoms of pain and fatigue that were not present for current hypermobility.28 In particular, ACR widespread pain index and ACR symptom severity scale allow for highly accurate identification and differentiation of fibromyalgia patients.29
Our findings of high rates of generalised joint laxity in this population are in line with other studies of ME/CFS, however, ours is the first to directly compare diagnostic assessments for hypermobility.13 Fibromyalgia and ME/CFS are both associated with inflammatory abnormalities and dysautonomia (eg orthostatic intolerance, postural orthostatic tachycardia syndrome and orthostatic hypotension), which is also commonly observed in symptomatic hypermobility.7–10 In fact, autonomic dysfunction is proposed to mediate disabling symptoms in fibromyalgia and has an established association with variants of connective tissue and heightened interoceptive sensibility.30 Interoceptive sensibility is the subjective measurement of the sense relating to one's own internal bodily sensations.24 While it is clear that there are associations between symptomatic hypermobility and both fibromyalgia and ME/CFS, the relationships between these conditions remain poorly understood. Ongoing research seeks to extend our observations reported here to determine how symptomatic hypermobility relates to autonomic and inflammatory induced changes in pain and fatigue in fibromyalgia and ME/CFS. Limitations of the present study include relatively small control group and difficulty in discriminating between pain-predominant and fatigue-predominant disease.
This paper adds further recognition to the high rates of hypermobility in fibromyalgia and ME/CFS, which is important with growing recognition of ‘post-viral’ fatigue syndromes in COVID-19. However, ours is the first study to use multiple complementary assessments of joint hypermobility and variant connective tissue to explore these relationships. A rich debate has been stimulated by a recent paper reporting the prevalence of EDS and JHS.21 While other forms of EDS are likely rare, the present study suggests hEDS is common among patients with pain and fatigue. Our control group is too small to make more than anecdotal statements regarding hEDS prevalence. However, approximately one in five of those meeting Brighton criteria for joint hypermobility syndrome might endorse a diagnosis of hEDS and many patients appear to remain undiagnosed.
The classification of symptomatic joint hypermobility and variants of connective tissue is an evolving area.17,19,31 Importantly, this study reveals that distinct aspects of the diagnostic criteria for symptomatic hypermobility predict symptom severity in pain and fatigue conditions. From these data, it would appear that the Brighton criteria predict fibromyalgia and ME/CFS diagnosis and symptomatology. Interestingly, the Brighton criteria make use of the historical account of joint laxity, which was highly associated with symptom severity, compared with current joint laxity, which is not included within the hEDS 2017 criteria (criterion 1).
This relatively small study highlights the need for better recognition and accurate diagnosis in these poorly understood conditions. Fibromyalgia patients may wait, on average, almost a year after experiencing symptoms before presenting to a physician, and a diagnosis of fibromyalgia may take around 2.3 years, presenting to 3.7 different physicians, to be established.32 Once confirmed, a fibromyalgia diagnosis may have mixed benefits for patients. Similar delays to diagnosis are observed for ME/CFS.33 The impact on quality of life in fibromyalgia and ME/CFS is severe. Greater awareness among the scientific and medical community about the overlapping nature of these conditions and their system-wide symptomatology will improve the appropriate diagnosis and multi-disciplinary treatment for patients.34 Studies underway will determine the wider role of variant connective tissue (of which joint hypermobility may be but a single manifestation) and its relationship to autonomic and inflammatory induced changes in pain and fatigue in fibromyalgia and ME/CFS including interoceptive and neural mechanisms and the role of the transcriptome.
Summary
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Diagnostic criteria to evaluate symptomatic hypermobility.
Acknowledgements
We wish to acknowledge the invaluable practical assistance of Valentina Toska and Mel Smith, the significant support of the Clinical Investigations Research Unit (Brighton and Sussex University Hospitals NHS Trust) and the editorial assistance of Robert Simonoff and AS Chamings. We wish to acknowledge the assistance of the Brighton and Sussex University NHS Hospitals Trusts Patient and Public Involvement Panel (JAFFA Panel).
Funding
This project was primarily funded by a Versus Arthritis grant (21994), with additional support provided by a studentship awarded by Action for ME and match-funded by Brighton and Sussex Medical School. The work was also supported by a charitable donation from the Fibroduck Foundation. Jessica Eccles was supported by the National Institute for Health Research (CL-2015-27-002). We are indebted to the Sussex ME/CFS Society and ReMEmber for their promotion and engagement with the study.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Neural Correlates of Autonomic Interoception in a Clinical Sample: Implications for Anxiety
- The Neural Correlates of Autonomic Interoception: Perceptual Mismatch and Clinical Implications
- Gastrointestinal symptoms and nutritional issues in patients with hypermobility disorders: assessment, diagnosis and management
- Finding your own way to manage patients with functional disorders
- The challenges of chronic pain and fatigue