
Case presentation
A 67-year-old woman with a background of type 2 diabetes mellitus (T2DM) presented to the dermatology department with a 4–6 week history of a blistering eruption and oral mucosal ulceration.
She had blisters arranged in an annular fashion and erosions on her trunk and limbs, and desquamative gingivitis and ulceration in her mouth (Fig 1). A diagnosis of bullous pemphigoid or linear immunoglobulin (Ig) A bullous dermatosis was suspected; the former was confirmed by histologic findings of a sub-epidermal blister with a polymorphonuclear infiltrate admixed with eosinophils and the presence of linear staining for IG3 and C3 at the basement membrane zone on direct immunofluorescence.
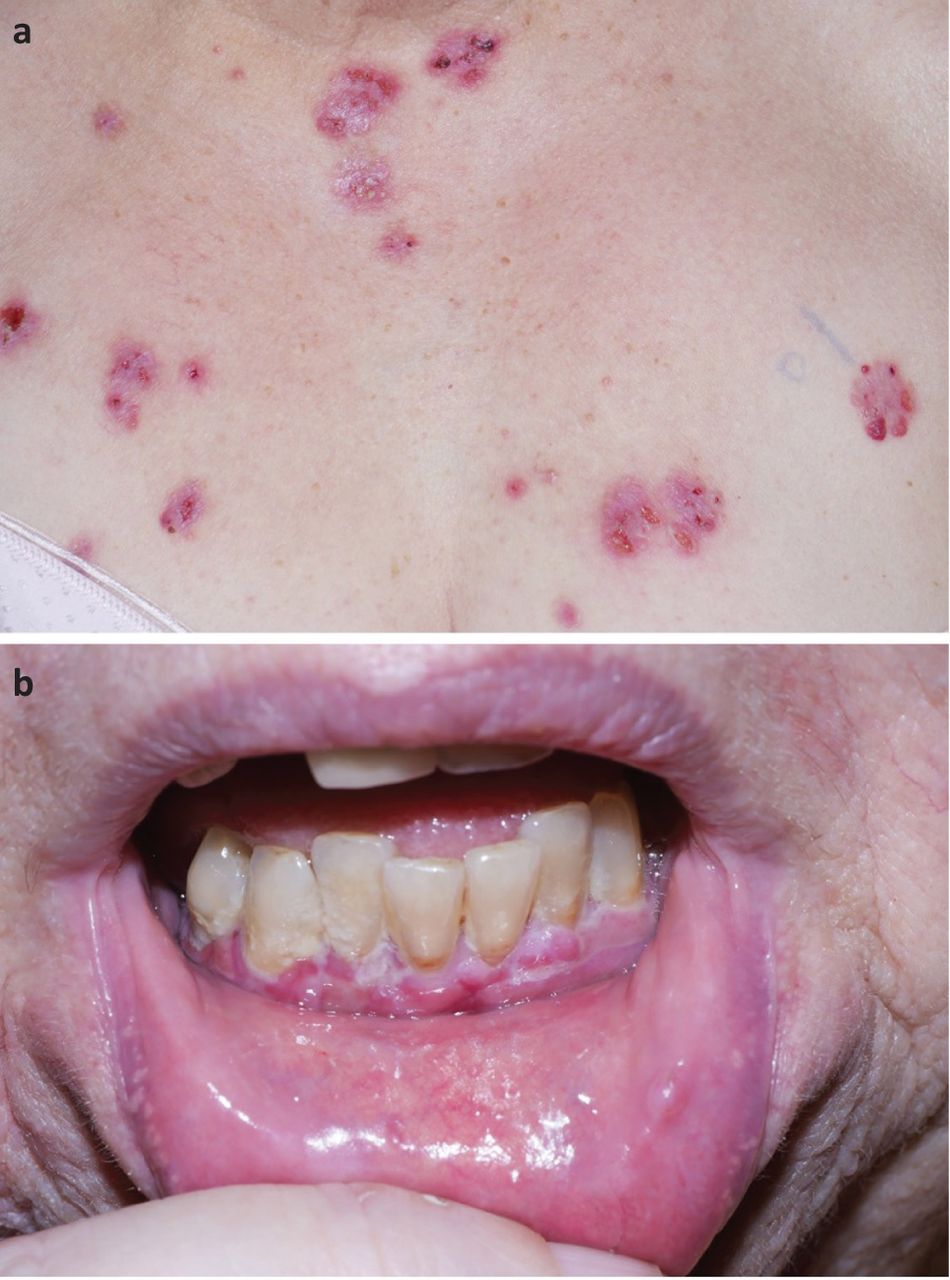
a) Blisters and erosions on the anterior chest wall. b) Desquamative gingivitis.
From her medication history, we identified that 13 months prior to developing the rash she was started on linagliptin, a dipeptidyl peptidase-4 (DPP-4) inhibitor, to manage her T2DM. The linagliptin was stopped and she was managed with topical corticosteroids, clobetasol propionate 0.05% ointment and betamethasone 500 mg mouthwash.
She improved without requiring systemic corticosteroids or other immunosuppressive agents. Interestingly, as a result of a painful mouth, she lost 15 kg in weight and no longer required oral anti-diabetic medication.
Discussion
Bullous pemphigoid is an organ specific autoimmune blistering skin disease that most commonly affects the elderly and has an annual incidence of 4.3 per 100,000.1 It occurs as a result of immunological responses to BP180 and BP230 antigens, both components of hemidesmosome proteins that play a role in the adhesion between the epidermis and dermis. The typical clinical presentation is of tense bullae often preceded by and/or associated with an eczematous or urticarial rash. Pruritus is the hallmark feature and mucosal involvement is uncommon. Diagnosis is based on a combination of clinical manifestations, direct and indirect immunofluorescence and serological tests. Although some patients respond to topical corticosteroids alone, many require a prolonged course of oral corticosteroids and other systemic immunosuppressants that are associated with severe adverse effects.
Bullous pemphigoid can occur secondary to a number of medications.2 DPP-4 inhibitors (such as linagliptin), widely used in the management of T2DM, have recently been implicated. The latency period between the initiation of a DPP-4 inhibitor and the development of bullous pemphigoid ranges from 1 to 48 months.3 Response to withdrawal of the medication varies from partial or complete remission of bullous pemphigoid in one study to no change in disease course in another.4,5
This case is presented to alert physicians of the risk of developing bullous pemphigoid during the management of diabetes with DPP-4 inhibitors. This awareness can prevent the use of systemic medications that have significant side effects, especially in the elderly population, because some patients improve with medication withdrawal. Lastly, our case highlights the value of a detailed medication history in the management of patients with skin eruptions.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
Related Articles
Cited By...
- No citing articles found.