
ABSTRACT
Mechanical thrombectomy is a highly effective but time dependent treatment for acute ischaemic stroke due to large vessel occlusion. In the UK, the national clinical guidelines for stroke and National Institute for Health and Care Excellence guidance endorses thrombectomy as an acute stroke treatment, and NHS England commissioned thrombectomy services. However, there are no UK ‘real-world’ data to verify the efficacy of the hub-and-spoke model in thrombectomy. There are currently 24 tertiary neuroscience centres in the UK that can provide thrombectomy treatment and many of these operate only within working hours. This study is the first to demonstrate that a hub-and-spoke thrombectomy service in routine UK 24/7 clinical practice is as effective and safe as in the setting of randomised controlled clinical trials. However, there are 9.3% of patients accepted for transfer to the thrombectomy centre who did not proceed to thrombectomy, mostly due to delays. Fifty-three per cent of thrombectomy cases were performed outside of standard working hours when transfer delays were increased. A 24/7 thrombectomy service is needed to maximise the benefit to all suitable patients. Measures, including improving workflow and optimising work forces, are needed to minimise the delays and continue to improve the service.
Introduction
Stroke is a leading cause of mortality and disability.1 Endovascular mechanical thrombectomy treatment has been proven to be highly effective in patients with acute ischaemic stroke caused by large vessel occlusion (LVO) in the anterior circulation.2–7 Thrombectomy, like thrombolysis, is time dependent. A meta-analysis of randomised clinical trials suggested that, for every 9-minute delay in onset to reperfusion, 1/100 patients will have more severe disability at 90 days.8 This was echoed by the MR CLEAN real-world registry, which showed for every hour delay from stroke onset to starting thrombectomy results in a 5.3% decrease in the probability of functional independence and a 2.2% increase in mortality.9
The time dependence of thrombectomy has led to international debate on optimal thrombectomy models: the hub-and-spoke model (initial transport to the closest thrombolysis centre followed by a secondary transfer to a thrombectomy centre) vs the mothership model (direct admission to a thrombectomy centre). In the UK, the national clinical guidelines for stroke recommended thrombectomy for appropriate patients.10 Thrombectomy services were then commissioned following a review of cost-effectiveness based on a hub-and-spoke model in the UK.11,12 However, there are no UK ‘real-world’ data to verify the efficacy of the hub-and-spoke model in thrombectomy. There are currently 24 tertiary neuroscience centres in the UK that can provide thrombectomy treatment. Many operate within working hours only, and barriers remain in implementing a thrombectomy service for all suitable patients.
The aims of this study were to examine the safety and efficacy of the hub-and-spoke thrombectomy model in real-world UK NHS practice, and to identify any necessary improvements.
Method
We used data from the local thrombectomy registry with the approval of the institutional audit committee (AUDI000377). This is an ongoing prospective registry of consecutive patients with acute ischaemic stroke accepted for thrombectomy treatment. In our hub-and-spoke model, patients with suspected stroke are initially taken to the nearest hyperacute stroke centre (spoke). Patients with confirmed stroke caused by LVO are then transferred to the thrombectomy centre (hub) with thrombolysis started if appropriate. Our thrombectomy service comprises a comprehensive stroke centre with a neuroendovascular team, four suburban hyperacute stroke centres (spokes) and two ambulance services, serving a total population of approximately 3.5 million. The average travel times from spoke to hub range from 50 to 70 minutes by ground or air ambulance. The thrombectomy referral rates are not routinely collected in the registry but a previous audit demonstrated that 8.6% of patients directly admitted to the hub for ischaemic stroke were referred for thrombectomy, whereas 2.4% from spoke centres were referred.
All hub-and-spoke centres have 24/7 access to computed tomography (CT) and CT angiography (CTA). Imaging can be transferred between centres via the secure Image Exchange Portal (IEP). Fig 1 shows the workflow chart for hub-and-spoke centres. For patients presenting to spoke centres, door-to-door (DTD) time is from arrival at a spoke centre to arrival at the hub centre; this comprises door-in–door-out (DIDO) time (arrival at a spoke centre to leaving for the hub centre) plus en route transfer time. DIDO comprises three parts: door-to-needle (DTN) time, decision time and turnaround time. DTN time is from arrival at hospital to thrombolysis. Decision time is referral to acceptance for transfer time. Turnaround time is from calling ambulance to departure for the hub centre. Time from call to ambulance to arrival at the spoke centre was defined as prolonged if it was above 30 minutes. To avoid futile reperfusion, CT ± CT perfusion (CTP) was repeated on arrival for prolonged transfer delays or clinical deteriorations during conveyance. Door-to-puncture (DTP) time is from hub arrival to arterial puncture, including handover and repeating imaging as needed. Hub centre direct presentation time measures are DTN, decision and turnaround from emergency department (ED) to angio-suite. Working hours (WH) cases were presentations between Monday to Friday at 8am to 6pm. Presentations outside this time were considered out of hours (OOH) cases. Nocturnal transfer times are defined as 7pm to 7am.

Hub-and-spoke thrombectomy workflow chart. a) Patients who arrive to spoke stroke centres first: patients with acute ischemic stroke will be assessed and treated with thrombolysis if suitable (DTN); if a large vessel occlusion is confirmed, patients will be referred to a hub stroke centre (decision); once accepted, turnaround is the time from the ambulance being called, ambulance arriving at scene and hand over to ambulance departure for the hub centre; spoke transfer DTP is the time from arrival at angio-suite, repeat imaging (as needed), handover and anaesthetic induction time up to arterial puncture. b) Patients who arrive at the hub stroke centre directly: suitable patients will have thrombolysis (DTN) and referred to the thrombectomy team (decision); once accepted, they will have a short turnaround time from the emergency department to the angio-suite and a short ATP time including hand over and anaesthetic induction only. ATP = arrival to puncture; DIDO = door-in–door-out; DTD = door-to-door; DTN = door-to-needle; DTP = door-to-puncture.
We used the inclusion criteria of 18 years of age or older; and intracranial proximal arterial occlusion in the anterior circulation demonstrated by CTA or digital subtraction angiography (DSA). Patients transferred for thrombectomy between 01 July 2016 and 30 June 2019 were included in the data analysis.
The definition of thrombectomy was arterial puncture in the angiography suite. The choice of endovascular treatment modality was at the discretion of the treating interventional neuroradiologist (INR). Stroke onset was defined as witnessed symptom onset time or last seen well time if the symptom onset was unwitnessed. Thrombectomy start time was defined as the time of arterial puncture. Reperfusion time was only recorded in patients who achieved successful recanalisation with thrombectomy. Successful recanalisation was defined as a modified thrombolysis in cerebral ischaemia (mTICI) score 2b–3. Collateral status on single phase CTA was independently assessed retrospectively by two neuroradiologists blinded to clinical outcomes. Collaterals were dichotomised into good (≥50% filling) or poor (<50% filling) in the ischaemic hemisphere by CTA in the equilibrium phase. Tandem occlusion was defined as an intracranial LVO concomitant with either a complete extracranial internal carotid artery (ICA) occlusion or critical stenosis, with the latter defined pragmatically as a high-grade stenosis that precluded passage of interventional devices other than a microwire and/or microcatheter. Good functional outcome was defined as a modified Rankin Scale (mRS) score 0–2 at 90 days. Symptomatic intracerebral haemorrhage (sICH) was classified according to the European Cooperative Acute Stroke Study (ECASS) II criteria.13 Clinical stroke severity was measured using the National Institute of Health stroke scale (NIHSS) score prior to and at 24 hours post-thrombectomy.
For data analysis, median and interquartile ranges (IQR) were reported for continuous variables. Percentage and count were reported for categorical variables. Differences were assessed using independent t-tests for continuous variables and chi-squared tests for categorical variables. Multivariable regression and binary logistic regression analysis were performed to identify independent factors. In all analyses, a two-tailed p<0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 24 (IBM, Armonk, USA).
Results
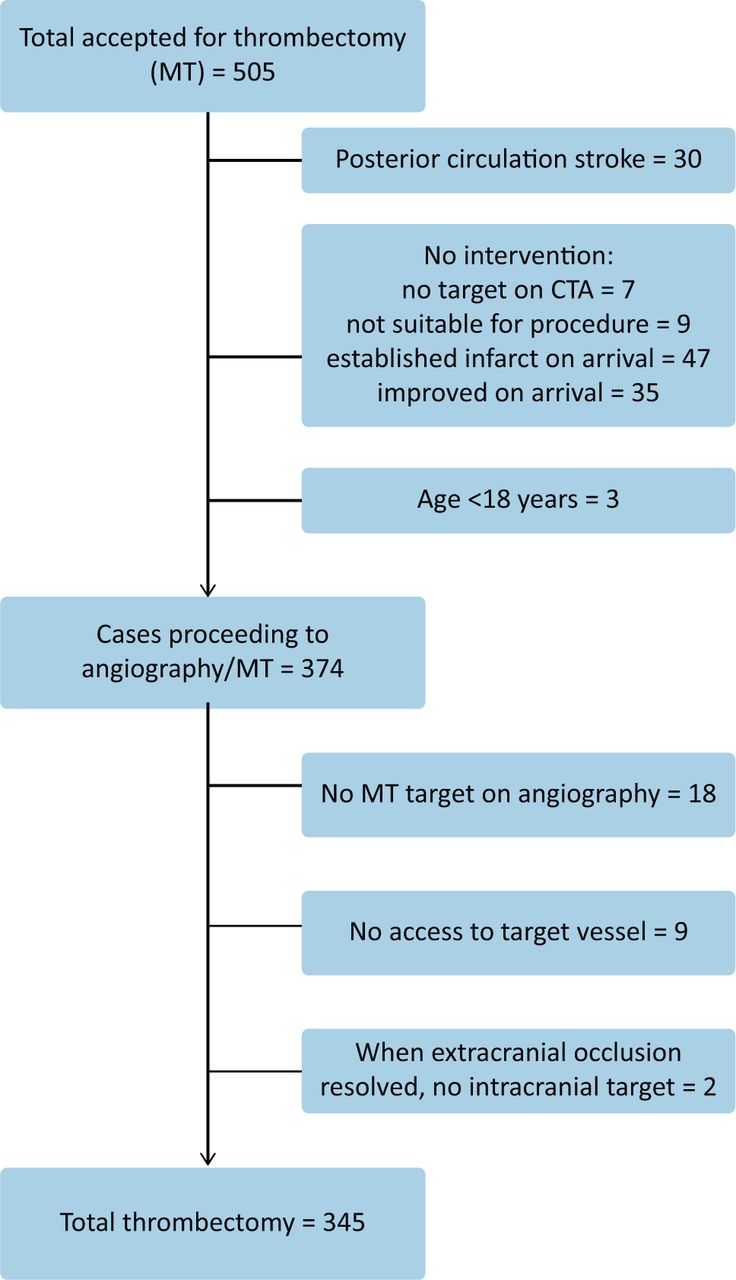
During the study period between July 2016 and June 2019, 505 patients with acute ischaemic stroke due to LVO were referred, accepted and arrived for thrombectomy (Fig 2). Three-hundred and seventy-four patients had arterial puncture and were included in this analysis. Of these, target occlusion was reached and thrombectomy attempt was performed in 345 patients.
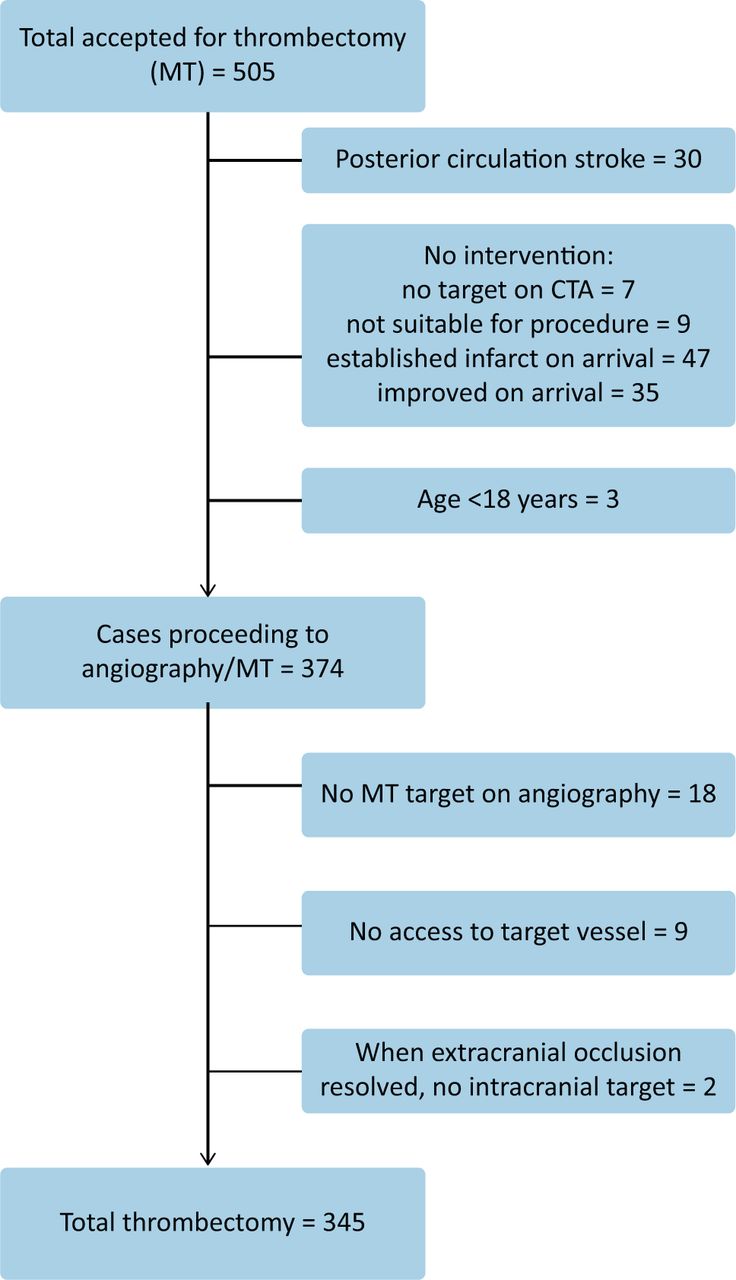
Mechanical thrombectomy cases (01 July 2016 – 30 June 2019). CTA = computed tomography angiography; MT = mechanical thrombectomy.
Comparison of our cohort with HERMES and the MR CLEAN registry
To evaluate the outcome of the hub-and-spoke model, we compared our cohort with HERMES meta-analysis (using patient level data from clinical trials) and another real-world dataset, the MR CLEAN registry (supplementary material S1).7,14 Patients in both the MR CLEAN registry and our cohort had significantly lower rates of good pre-stroke baseline function (mRS 0–1) compared with those in clinical trials (79.4% MR CLEAN; 84.2% our cohort; 95% HERMES). The prevalence of stroke risk factors was similar across these three studies. In our cohort, there was a higher rate of tandem occlusion (9.6% HERMES vs 18.7% this study) and a lower rate of thrombolysis (82.9% HERMES vs 75.7% this study). The main reasons for not receiving thrombolysis in our cohort were prior anticoagulation or unknown stroke onset time. When compared with HERMES, our cohort had similar symptom onset to arterial puncture times, higher successful recanalisation rates and comparable outcome measures (good functional outcome (mRS 0–2; 46% HERMES vs 43.3% this study) and mortality at 90 days (15.3% HERMES vs 17.9% this study), and low rates of sICH.
Our quarterly data review showed an initial learning curve. The successful reperfusion rate increased from 60% in the first quarter to above 80% by the third quarter. For spoke patients, the average DTP time improved steadily from an average of 45 minutes in the first quarter to 17 minutes in 2019.
Outcomes in hub-and-spoke patients
To evaluate if the hub-and-spoke model can deliver effective thrombectomy treatment to both hub patients and spoke patients, we compared both groups (Table 1). Compared with hub patients, spoke centre patients were more likely to have better baseline function (pre-stroke mRS 0–1; 89.0% spoke vs 77.4% hub; p<0.001), fewer comorbidities especially hypertension (48.9% vs 60.6%; p=0.024) and higher thrombolysis rates (83.1% vs 65.2%; p<0.001). Both groups achieved high rates of successful reperfusion. However, there were significant delays in groin puncture in the spoke group due to transfer times (Table 2). Both groups achieved similar functional outcomes (mRS 0–2; 45.8% vs 41.5%; p=0.413) and mortality rates at 90 days (16.8% vs 18.3%; p=0.710). These data are comparable with HERMES.7 Logistic regression analysis showed that good pre-stroke function (mRS 0–1; odds ratio (OR) 3.211; 95% confidence interval (CI) 1.596–6.462; p=0.001), good collaterals (OR 2.101; 95% CI 1.1296–3.406; p=0.003) and successful recanalisation (mTICI 2b–3; OR 3.662; 95% CI 2.013–6.661; p<0.001) are independent predictors for good outcome. Fifty-three per cent of thrombectomy cases were performed OOH.
Baseline treatment characteristics and outcome
Baseline and outcome for cases not proceeding for thrombectomy
Variation in proceeding to thrombectomy
Of 505 patients, 98 did not have arterial puncture (Fig 2). The reasons for not proceeding to thrombectomy were established infarction on repeat CT (n=47), clinical improvement (n=35), no thrombectomy target on repeat CTA (n=7) and non-stroke related comorbidities (n=9). Five out of the 35 patients with clinical improvement were direct hub presenters. Table 2 shows comparisons of spoke patients who did against those who did not proceed to thrombectomy. Of those who did not proceed to thrombectomy, those clinically improved against those with established infarction on repeat imaging were also compared (supplementary material S2). This comparison demonstrates that patients who did not have thrombectomy were more likely to have a proximal M1 occlusion and poor collateral status. They also had lower rates of good functional outcome (33.3% vs 41.6%; p<0.001) and higher mortality at 90 days (28.6% vs 18.3%; p<0.001). Patients with an established infarct on arrival had higher rates of proximal occlusion and poor collaterals. Patients that improved on arrival had significant reductions in NIHSS on arrival compared with their initial presentation at spoke centres (from median 16 (interquartile range (IQR) 10.5–20) to median 3 (IQR 2–4)). In this cohort, all improved patients (except for one) maintained the improved NIHSS up to discharge or transfer back to spoke centres; 83.3% of these patients had good functional outcome at 90 days. One patient with a transient increase in NIHSS at 24 hours had a good mRS of 1 at 90 days. One patient in the improved group died within 90 days due to a further severe stroke 2 weeks after thrombectomy transfer.
Recanalisation times and outcomes
Patients from spoke centres had prolonged onset to recanalisation time due to inter-hospital transfer times (Table 1). When we compared patients who proceeded to thrombectomy against those that did not (supplementary material S2), the latter were more likely to have prolonged DTD time (>180 minutes; 41.1% vs 58.4%; p=0.029; Table 2), and more likely to be nocturnal referrals (36.5% vs 63.5%). Further logistic regression showed that only prolonged DTD (>180 minutes) was associated with not proceeding to thrombectomy (OR=0.481; 95% CI 0.282–0.820; p=0.007).
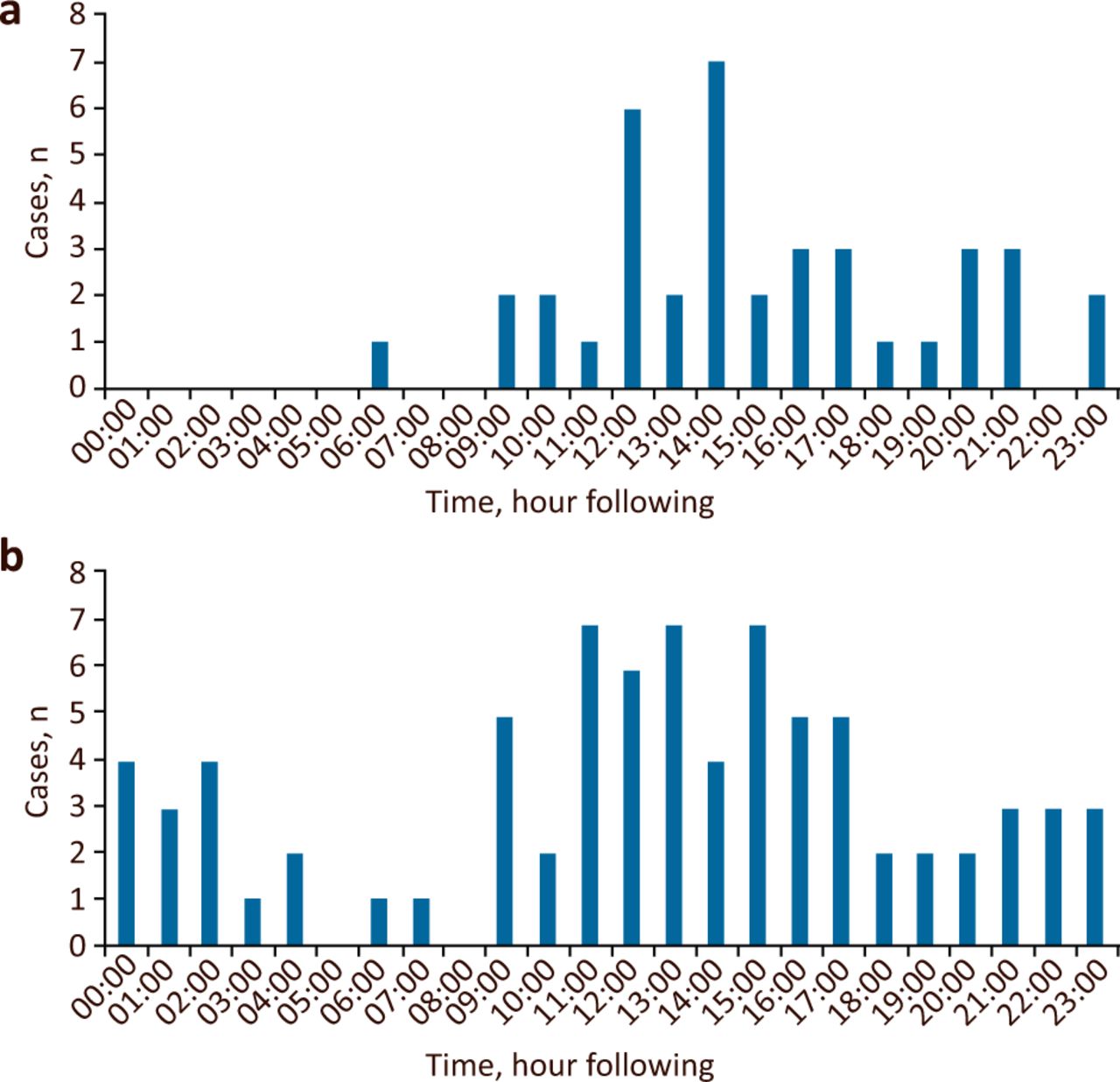
To further investigate the causes of delay in DTD time (Fig 1), we sampled DIDO times of the four spoke centres in two periods: 2017 and 2019. In the 2019 data, there were eight cases recorded with prolonged decision-making, seven due to delayed image transfer by IEP. Using ambulance service data, we were able to examine the turnaround time. Although there was no significant difference in call to ambulance-on-scene time (median 7 minutes (IQR 1–14) in 2017 vs median 10 minutes (IQR 5–22) in 2019), 21% of cases in 2019 had a prolonged time from call to ambulance arrival at spoke centres (75% of which were OOH) compared with only 10% in 2017. Compared with the 2017 period, there were significant changes in transfer pattern in 2019 (Fig 3). There were increases in both total thrombectomy transfer requests and the demand for nocturnal thrombectomy transfer. It was noted that 9 cases of OOH delay in 2019 were due to ‘no crew to send’. DTD time was also affected by ambulance-on-scene handover time that had improved between the two periods (median 28 minutes (IQR 15.5–35.5) in 2017 vs median 19 minutes (IQR 14–25) in 2019).
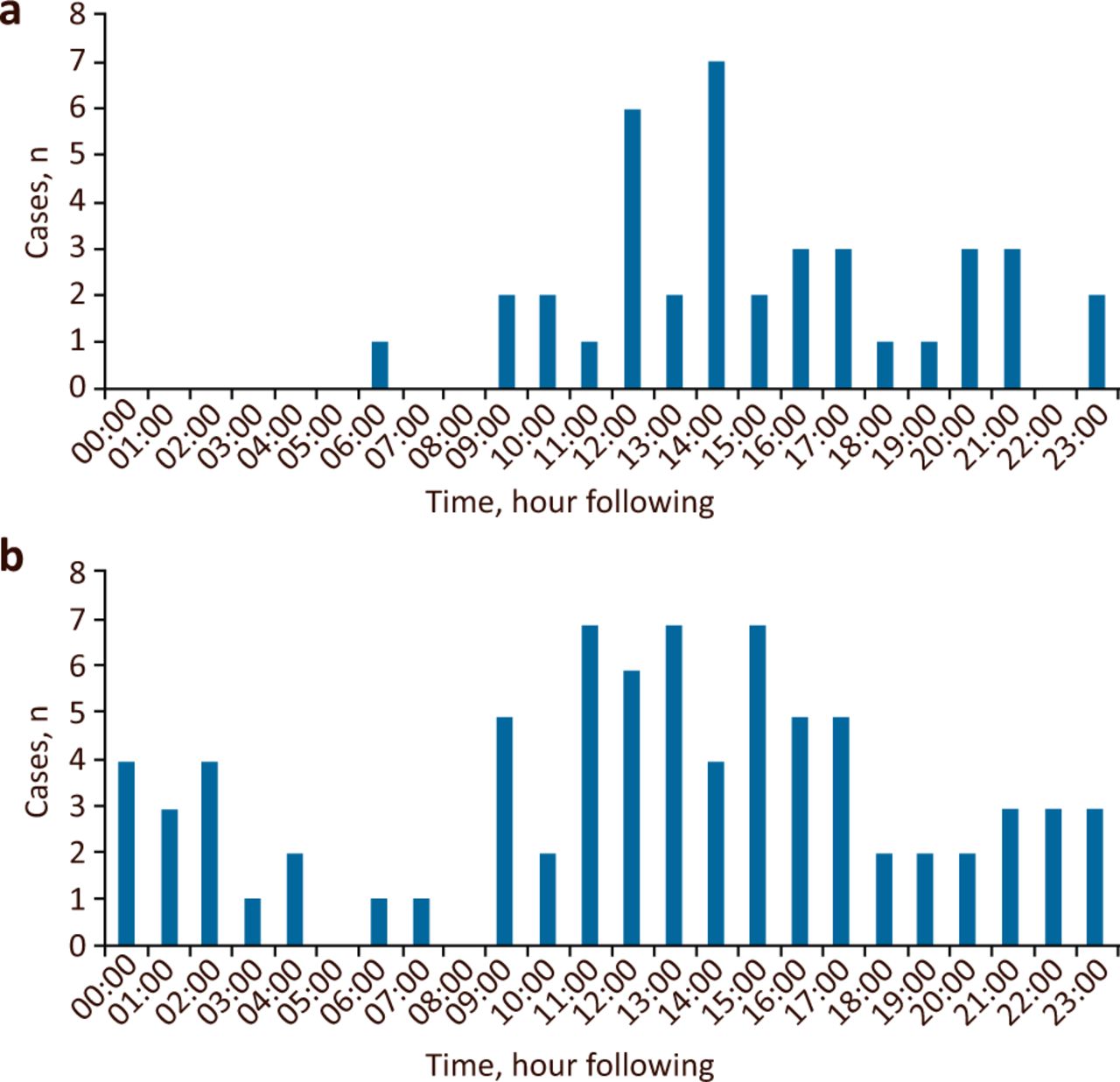
Thrombectomy transfer distribution across 24 hours. a) 2017. b) 2019. Approximate changeover of ambulance crews occurred at 7am and 7pm.
Discussion
Our study shows that the hub-and-spoke thrombectomy model in routine UK clinical practice, for patients with acute stroke due to LVO in anterior circulation, is as effective and safe as in clinical trials. However, there were many patients who did not proceed to thrombectomy, caused by a delay in transfer from a spoke to the hub centre. Fifty-three per cent of the thrombectomy workload was during the OOH period when additional delay occurred. Improvements in the workflow to ensure rapid transfer and reduce the DTD time could further improve this.
Our data showed that despite poor pre-stroke baseline function, high comorbidities in ‘real-world’ patients and the significant transfer delay for spoke patients, clinical outcomes are comparable to clinical trials (Table 1; supplementary material S1). This supports the feasibility of the hub-and-spoke model. Holodinsky et al used conditional probability modelling based on thrombectomy data from Ireland to compare hub-and-spoke and mothership models.15 If all aspects of major acute ischaemic stroke care (including DTN, DIDO at spoke and DTP at hub) are optimised, the study suggested that hub-and-spoke would be a better thrombectomy model. Furthermore, central specialised care will allow workforce optimisation and nurture specialised skills for better patient care as shown in our high reperfusion rates and continuous improvements in workflow times.
In our cohort, 26% (77/296) of spoke patients did not proceed to thrombectomy, and therefore were not included in the final analysis. A higher rate of comorbidities and poor pre-stroke function in patients that did not proceed due to established infarction (data not shown) may have caused this patient selection bias, and produced the comparable outcome between spoke centres and hub centres despite longer workflow times. Patients that did not proceed to thrombectomy due to clinical improvement on arrival had stable improvement. This needs to be repeated in a longer-term study.
Our data showed prolonged delays in transfer are associated with not proceeding to thrombectomy; Regenhardt et al reported similar findings.16 They reported the probability of undergoing thrombectomy decreases by 1% for each additional minute of transfer time over an ideal transfer time of 60 minutes. This study and our data emphasise the need to shorten DTD time in order to maximise thrombectomy rates. We noted a significant increase in transfer demand during night-time when the ambulance workforce is reduced (Fig 3). This finding agreed with Regenhardt's study, although there may be different causes given the different settings.16 To meet a shortfall in OOH ambulance provision, wider data analysis and commissioning changes are needed. We organised simulation trainings for stroke nurses at spoke hospitals to emphasise the need for rapid transfer, clinical care during conveyance and high-quality handover to the thrombectomy team. We are currently trialling an automated analysis software across our hub-and-spoke centres which may reduce delays in decision making.
In the UK, about 1% of stroke patients received thrombectomy in 2018 although McMeekin et al estimated that about 10% of stroke patients are eligible for this treatment.17,18 Most tertiary neuroscience centres are working on service expansion with the aim of rolling out a 24/7 service within a few years. Dutta et al modelled service expansion for service provision from 8am to 8pm.19 Our data showed that more than 50% of all thrombectomies were performed OOH, and 33% were nocturnal (excluding those that did not proceed to thrombectomy). These data suggest 24/7 thrombectomy services are required in order to maximise the benefit to all suitable patients. Optimal workforce arrangements are needed to ensure parity of service in both WH and OOH periods.
It is important to note that both international and UK studies to evaluate hub-and-spoke model and cost effectiveness are based on optimised treatment times, eg 60 minute DIDO time at spoke centre (comprising 30 minutes DTN time and 30 minutes decision with turnaround time), 60 minutes transfer time and 60 minutes hub DTP time for hub direct presenters.12,15,19 Our data demonstrates the urgent need for improvement in real-world practice to reach these targets. Regular governance and service meetings including all members in the thrombectomy pathway will allow continuous discussion on how to further improve our service.
This study has limitations beyond being a single centre, retrospective analysis. We did not have complete records for patients referred and not accepted for thrombectomy. More detailed data on each time point of the complex workflow are needed to identify potential targets for improvement.
Conclusion
This study is the first to present evidence that a hub-and-spoke thrombectomy service in 24/7 UK clinical practice, for patients with acute ischaemic stroke due to proximal intracranial vessel occlusion in the anterior circulation, is as effective and safe as in the setting of randomised controlled clinical trials. Over half of the thrombectomy cases were carried out during non-working hours, suggesting 24/7 thrombectomy services are needed. There are many patients who did not proceed to thrombectomy, mostly due to delays in referring and transfer, especially during OOH. Improvement measures to reduce avoidable delay in inter-hospital transfer, and optimising work forces are needed to improve the hub-and-spoke thrombectomy service.
Summary
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Comparison of St George's cohort with HERMES and MR CLEAN registry.
S2 – Baseline and outcome for cases not proceeding for thrombectomy.
Acknowledgements
We thank Jennifer Corn, stroke nurse, for collecting 90-day mRS data for the registry.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
{kind=link}