
ABSTRACT
There is growing evidence linking vitamin D deficiency with risk of COVID-19. It is therefore distressing that there is major disagreement about the optimal serum level for 25-hydroxyvitamin D (25(OH)D) and appropriate supplement dose. The UK Scientific Advisory Committee for Nutrition has set the lowest level for defining sufficiency (10 ng/ml or 25 nmol/L) of any national advisory body or scientific society and consequently recommends supplementation with 10 micrograms (400 IU) per day. We have searched for published evidence to support this but not found it. There is considerable evidence to support the higher level for sufficiency (20 ng/ml or 50 nmol/L) recommended by the European Food Safety Authority and the American Institute of Medicine and hence greater supplementation (20 micrograms or 800 IU per day). Serum 25(OH)D concentrations in the UK typically fall by around 50% through winter. We believe that governments should urgently recommend supplementation with 20–25 micrograms (800–1,000 IU) per day.
Vitamin D, COVID-19 and current guidance
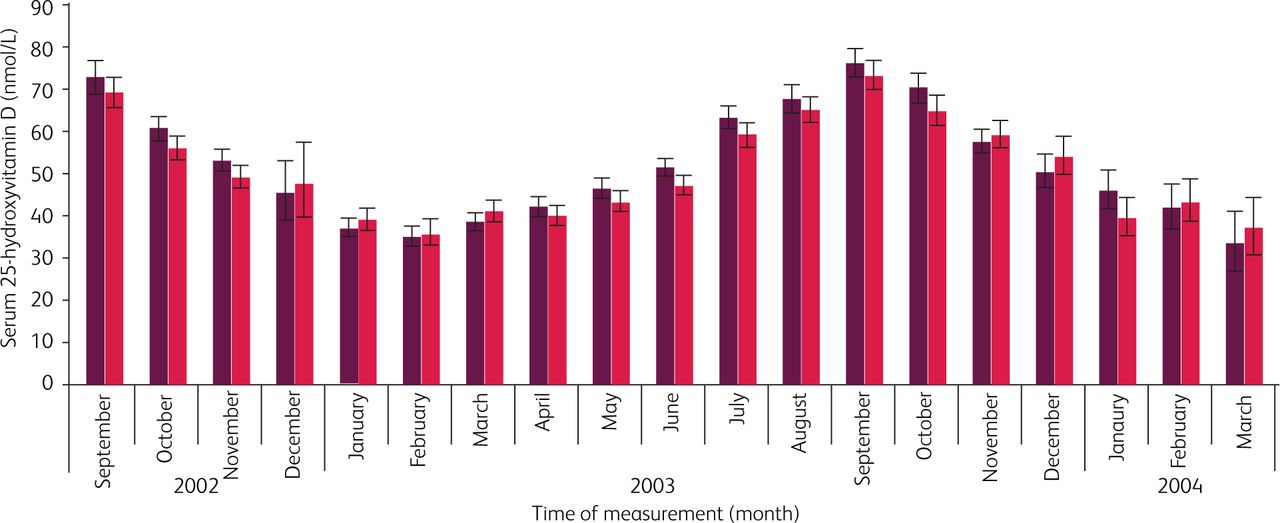
Evidence for a possible impact of vitamin D deficiency on COVID-19 has been strengthened recently by the positive Spanish trial of 25-hydroxyvitamin D3 (25(OH)D3 or calcifediol) in hospitalised patients1 and by the association between vitamin D deficiency and increased risk for COVID-19 seropositivity found in hospital staff from Birmingham, UK.2 There is a plausible scientific basis for this as 25(OH)D3 is a prohormone that can be metabolised to active, hormonal 1,25-dihydroxyvitamin D3 (1,25(OH)2D3). When bound to its intracellular vitamin D receptor (VDR), 1,25(OH)2D3 is able to regulate many target genes, with beneficial effects on immune and lung cell function that may be compromised by vitamin D deficiency.3 In the UK, serum 25(OH)D concentrations fall by about 50% from a peak in September to a trough in February (Fig 1).4 With much of the northern hemisphere experiencing a resurgence of the pandemic as we move into winter, it is increasingly urgent to ensure appropriate public health measures to prevent vitamin D deficiency.
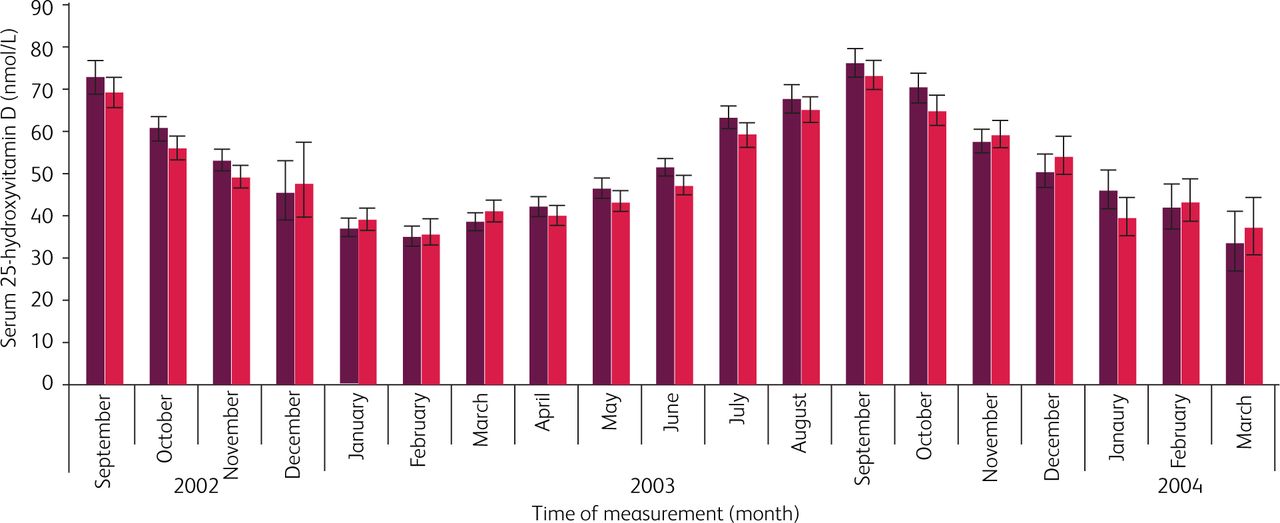
Seasonal variation in serum vitamin D concentrations (mean (95% confidence interval)) among 7,437 white British (1958 British birth cohort) at age 45. Dark red bar = male, red bar = female. Adapted with permission from Hypponen and Power 2007.4
There is unfortunately considerable variance between countries in recommendations for supplementation: 10 micrograms (400 IU) per day in the UK, 600 IU per day in the EU and 600 IU per day or 800 IU per day for those aged >70 years in the USA.5 The UK Scientific Advisory Committee on Nutrition (SACN) is an outlier among representative bodies in choosing the lowest blood level (25 nmol/L) of 25(OH)D to define sufficiency when compared with thresholds of 50 nmol/l set by the American Institute of Medicine (now National Academy of Medicine) and European Food Safety Authority, and 75 nmol/l set by the US Endocrine Society. The evidence base underlying the UK target serum level has been questioned by others,6 and we now explore it further.
Seeking the evidence base for the UK SACN threshold for vitamin D sufficiency at 25 nmol/L
SACN in their 2016 report7 state (p43, section 6.17): ‘In the UK, a serum 25(OH)D concentration <25 nmol/L has been the threshold adopted to define increased risk of rickets (DH, 1998).’
In turn, the DH (Department of Health) 1998 report8 states (p40 6.2.3):
Plasma levels of 25(OH)vitamin D found in clinical rickets or osteomalacia range from undetectable to around 20nmo1/l [citing the 1991 DH report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy9] and a level of plasma 25(OH)vitamin D of 25nmo1/l has conventionally been used as a cut off for defining the lower limit of adequacy of vitamin D status [citing Grindulis et al 198610], although others have suggested slightly higher levels [citing Gloth et al 199511].
The DH reports8,9 that underpin the SACN position do not stand close scrutiny. The 1991 DH report9 states (section 18.1.2): ‘Plasma 25(OH)D concentrations in rickets range from not detectable to about 8 ng/ml’, citing Arnaud et al.12 However, this is definitely not what Arnaud et al reported: a case series of nine children with nutritional rickets, seven of whom had serum 25(OH)D concentrations above 10 ng/ml (= 25 nmol/L) and up to approximately 50 nmol/L.
Grindulis et al10 did indeed state: ‘For this study a vitamin D concentration <10 ng/ml (25 nmol/L) was taken to be suboptimal and <5 ng/ml deficient’ but no data were referenced in support of this statement.
Gloth et al11 state: ‘Reference ranges for our laboratory (normal range), 25 to 137 nmol/L (10 to 55 ng/mL)’. In the discussion of this paper, however they question the validity of the lower limit, commenting that:
the elevation in intact PTH levels seen with 25-OHD serum levels between 25 and 37 nmol/L (10 and 15 ng/mL) is distressing if we define a vitamin deficiency as the Food and Nutrition Board does, ie, ‘that level of an essential nutrient that leads to an abnormal physiologic change.’ Since secondary hyperparathyroidism causes abnormal bone loss, among other physiological changes, then perhaps the lower limit of the normal range for serum 25-OHD should be increased.
Here the trail ‘runs dry’ – seemingly the 25 nmol/L limit has been agreed by consensus within SACN rather than by referral to any specific source with the possible exception of the historic laboratory reference range (25 to 137 nmol/L) of the Johns Hopkins University School of Medicine, Baltimore as cited, but criticised, in Gloth et al.11
It is interesting that the earlier SACN (2007) position statement was much more circumspect and concluded (p38, section 13.118):
Accumulating evidence suggests that vitamin D may be important for health outcomes other than rickets and osteomalacia, and that plasma concentrations of 25(OH)D several fold higher than 25 nmol/L may be required for optimal health.
It is unclear why subsequent SACN reports have not addressed this.
It seems then that the UK SACN definition of vitamin D deficiency as <25 nmol/L and consequently the 400 IU per day supplement dosing was based on consensus rather than on any systematic analysis of data. It may be more than a coincidence that 400 IU is approximately the amount of vitamin D in one teaspoon of cod liver oil, for over 70 years the standard daily supplement recommended in Norway. With the passage of time and subsequent reports from SACN this position seems to have become firmly entrenched without any further evidence to justify it.
The SACN/UK government advised dietary intake level of 400 IU per day for all >4 years was re-affirmed in June 202013 on the account that:
This is the average daily amount of vitamin D (from natural food sources, fortified foods or supplements) needed by the majority (97.5%) of the population to maintain a serum 25(OH)D concentration ≥25 nmol/L when UVB sunshine exposure is minimal.
The ‘97.5%’ is presumably based on the definition of reference nutrient intake (RNI) as used by DH (1998) – ‘two standard deviations above estimated average requirements’. In 1998 the Department of Health set no RNI for older children or for adults aged 18–64 but did set 400 IU (10 microgram) per day as the recommendation for adults ≥65.8 This report cited a randomised trial comparing no supplement with 400 IU per day and 800 IU per day completed through to 1 year in 109 institutionalised elderly people. This showed that serum 25(OH)D increased to >40 nmol/L in all subjects who received either 400 IU or 800 IU per day.14 This does not however address the greatly increased vitamin D supplement requirements needed to achieve sufficiency in people with obesity.15
The evidence base for 50 nmol/L as the threshold for 25(OH)D sufficiency
This has been reviewed elsewhere.5 The American Institute of Medicine (now called the National Academy of Medicine) and the European Food Safety Authority both set >50 nmol/L 25(OH)D as the definition for sufficiency while the US Endocrine Society sets a higher level of >75 nmol/L. Serum concentrations of parathyroid hormone rise with vitamin D deficiency but there is considerable variation between individuals. Evidence supporting 50 nmol/L as a recommended serum vitamin 25(OH)D level was strengthened by Malabanan et al16 who looked at the impact of vitamin D supplementation on parathyroid hormone levels in 35 people with different baseline levels of 25(OH)D. People with baseline serum 25(OH)D concentrations in the ranges 27.5–39.9 and 40–49.9 nmol/l showed significant falls in parathyroid hormone in response to vitamin D supplementation whereas people with baseline 25(OH)D ≥50 nmol/l showed no significant fall in parathyroid hormone.
Muscle strength has also been studied as an outcome measure to define vitamin D sufficiency. Interestingly, the SACN (2016) report says (p68, section 6.169):
Evidence from cohort studies was also supportive of an association between mean serum 25(OH)D concentration and muscle strength and function when baseline serum 25(OH)D concentration is <50 nmol/L.7
Other studies have looked more broadly at associations between vitamin D status and all-cause mortality. Gaksch and colleagues17 performed a meta-analysis across a European consortium of eight prospective studies including 26,916 study participants, median age 61.6 years, followed-up for median 10.5 years. Significant increases in all-cause mortality were seen with baseline serum 25(OH)D <50 nmol/L. There was no significant increased mortality risk at high levels up to 125 nmol/L, important since an earlier study had suggested a possible U-shaped dose response curve.18
There is therefore a substantial body of evidence to support the 50 nmol/L definition of 25(OH)D sufficiency as set by the American Institute of Medicine and the European Food Safety Authority.
In the UK 55.4% of the population, rising to 69.3% in winter, are reported to have serum 25(OH)D <50 nmol/L and black, Asian, and minority ethnic populations, as well as people who by occupation or institutionalisation receive less sunlight exposure, are at still higher risk of insufficiency.19 A recent study of the UK Biobank cohort found that 92% of 6,433 UK-dwelling South Asians have 25(OH)D <50 nmol/L.20
Identification of the daily supplement dosage needed to achieve optimal vitamin D status defined as ≥50 nmol/L
Modelling based on a meta-analysis of 94 cohort studies that included 11,566 individuals supplemented for a median period of 274 days suggests that for adults, supplementation with 800 IU per day (but not 400 IU per day) should be adequate, even in obese individuals, for achieving >50 nmol/L (Table 1).21 However, to achieve >75 nmol/L would typically require supplementation of between 3,000 IU per day to 4,000 IU per day for an obese individual. It seems reasonable to conclude from this meta-analysis that a regular daily intake of at least 800 IU should be sufficient, even in obese individuals, to achieve a target blood level >50 nmol/L. A higher initial daily intake, eg 4,000 IU per day for the first 4 weeks, would be reasonable to achieve sufficiency quickly in people likely to be deficient during the current pandemic. Intermittent blood 25(OH)D monitoring and personalised replacement, although scientifically ideal, has a cost and is not essential given the safety of vitamin D supplementation at appropriate dosage.
Calculated daily vitamin D3 dose for achieving in vitamin D-deficient individuals target 25-hydroxyvitamin D levels of 50 nmol/L and 75 nmol/L, respectively
Regarding safety, SACN (2016) concludes that:
Upper limits for vitamin D recommended by EFSA, of 100 μg/d (4000 IU/d) for adults and children aged 11–17 y, 50 μg/d (2000 IU/d) for children aged 1–10 y, and 25 μg/d (1000 IU) for infants, are considered appropriate. The upper limits do not distinguish between total and supplementary vitamin D intake since dietary intakes of vitamin D make only a small contribution to total exposures at the ULs.7
Conclusion
The current UK SACN threshold for vitamin D sufficiency of 25 nmol/L 25(OH)D is set too low and is not supported by evidence. A higher threshold of 50 nmol/L is supported by the evidence and is safely achievable by supplementation with at least 800 IU per day (20 micrograms per day). Since vitamin D is widely sold in 1,000 IU capsules, and it is universally agreed that doses up to 4,000 IU per day are safe, then a recommendation of 800–1,000 IU per day (20–25 micrograms per day) for all adults would be safe and sufficient and should be urgently promoted.
Conflicts of interest
Martin Hewison and David Thickett have received speaking honoraria from Thornton Ross.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
Jump to section
- Article
- ABSTRACT
- Vitamin D, COVID-19 and current guidance
- Seeking the evidence base for the UK SACN threshold for vitamin D sufficiency at 25 nmol/L
- The evidence base for 50 nmol/L as the threshold for 25(OH)D sufficiency
- Identification of the daily supplement dosage needed to achieve optimal vitamin D status defined as ≥50 nmol/L
- Conclusion
- Conflicts of interest
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- COVID-19 pandemic and vitamin D: rising trends in status and in daily amounts of vitamin D provided by supplements
- Perspective: Vitamin D supplementation prevents rickets and acute respiratory infections when given as daily maintenance but not as intermittent bolus: implications for COVID-19
- Response
- Vitamin D