
ABSTRACT
Despite the recent announcement of promising drug candidates to treat COVID-19, there is currently no effective antiviral drug or vaccine. There is strong evidence that acute lung injury/acute respiratory distress syndrome (ALI/ARDS), likely triggered by a cytokine storm, is responsible for the severity of disease seen in COVID-19 patients. In support of this hypothesis, pilot studies using IL-6 receptor inhibitors such as tocilizumab have shown promising results. Therefore, the use of drugs or cocktails of drugs with broader ability to inhibit these cytokine receptors is likely to be effective. In this article, we propose the use of sphingosine analogues, which have been shown to mitigate acute lung damage in animal models of ALI/ARDS, as early adjuvant therapies to prevent and/or mitigate the cytokine response in COVID-19 patients. This proposal is based on the ability of these drugs to decrease the production of IL-6 and other cytokines. The potential application of fingolimod (FTY720), the oldest sphingosine analogue approved for the treatment of multiple sclerosis, in the early stages of COVID-19 is discussed in more detail as a prototype drug.
Introduction
The lack of specific treatment for patients with COVID-19 infection1 has triggered the search for treatment modalities including adjuvant drugs. Several existing drugs that have been approved for other diseases are being evaluated in pilot clinical trials in COVID-19 patients. The selection of these drugs is based on their effect on targets thought to be implicated in the pathophysiological mechanisms underpinning COVID-19 complications.
A significant number of patients have died from complications that at present are not clearly understood, but there is strong evidence that acute lung injury/acute respiratory distress syndrome (ALI/ARDS), likely triggered by a cytokine storm, may play a key role.2,3 Therefore, treatment for ALI/ARDS will play an important role in decreasing the mortality of the disease. ALI/ARDS are common conditions occurring in critically ill patients that are characterised by widespread pulmonary inflammation and by clinical symptoms such as hypoxemia, progressive dyspnea and even severe acute respiratory failure involving the lungs bilaterally.4
Cytokine storm is a systemic inflammatory response involving a plethora of cytokines.5 In COVID-19 patients the severity of the disease depends on the increase of pro-inflammatory factors such as IL-1, IL-2, IL-6, IL-7, IL-10, granulocyte-colony stimulating factor, interferon-γ-inducible protein 10, monocyte chemoattractant protein 1, macrophage inflammatory protein-1 alpha, and TNF-α.1 High levels of several cytokines (IL-2R, IL-6, IL-10, and TNF-a) were significantly associated with severe COVID-19 on admission.6 In addition, serum SARS-Cov-2 RNA (RNAaemia) was associated with elevated IL-6 concentration and poor prognosis in COVID-19 patients.7 Thus, blocking the biological activities of these cytokines, or at least the most important ones such as IL-6, may be beneficial for COVID-19 patients. This is the basis for the inclusion of tocilizumab (an IL-6 receptor blocker) and other IL-6 blockers in several treatment regimes. Tocilizumab appears to be an effective treatment option in COVID-19 patients at risk of cytokine storm as suggested by two pilot clinical studies8,9 and several case reports.10–15 It is natural to assume that to target the cytokine storm a cocktail of cytokine and/or cytokine receptor inhibitors is needed, which will result in a higher incidence of adverse effects. For instance, tocilizumab has been associated with hypertriglyceridemia in COVID-19 patients.16
Drugs with a broader ability to block cytokine activity may be more beneficial. In this article we propose the use of sphingosine analogues, in particular fingolimod, a drug approved for the treatment of relapsing-remitting (the most common) form of multiple sclerosis (MS).17,18 Fingolimod (FTY720, Gilenya®) is a non-selective agonist of sphingosine 1-phosphate receptor (S1PR). It acts as a selective functional antagonist of the S1P1 subtype by inducing receptor downregulation. This downregulation leads to immunosuppression.19
Rationale for the use of fingolimod and other sphingosine analogues in COVID-19 patients
FTY720 and its derivative AAL-R are sphingosine analogues that are phosphorylated by sphingosine kinase 2 (SphK2), one of the enzymes responsible for the conversion of sphingosine into S1P.20 In an animal model of influenza, AAL-R significantly inhibited the production of IL-1α, IL-1β, IL-6, IL-10, MCP-1, TNF-α and GM-CSF while maintaining protective neutralising antibody and cytotoxic T cell responses.21 FTY720 alleviated podocyte injury in a rat model chronic kidney disease via downregulation of inflammatory cytokines including TNF-α and IL-6.22 In addition, FTY720 has protective effect on several other conditions such as stroke, probably by decreasing pro-inflammatory cytokines such high mobility group box 1 (HMGB1) and tumour necrosis factor-α (TNF-α).23 Vascular endothelial cell (EC) barrier disruption may play a key role in ARDS; FTY720 analogues have been shown to potently enhance lung EC barrier function via G coupled receptor signaling in vitro24 and FTY720 has been shown to alleviate/mitigate lung injuries in mice experimental models.25
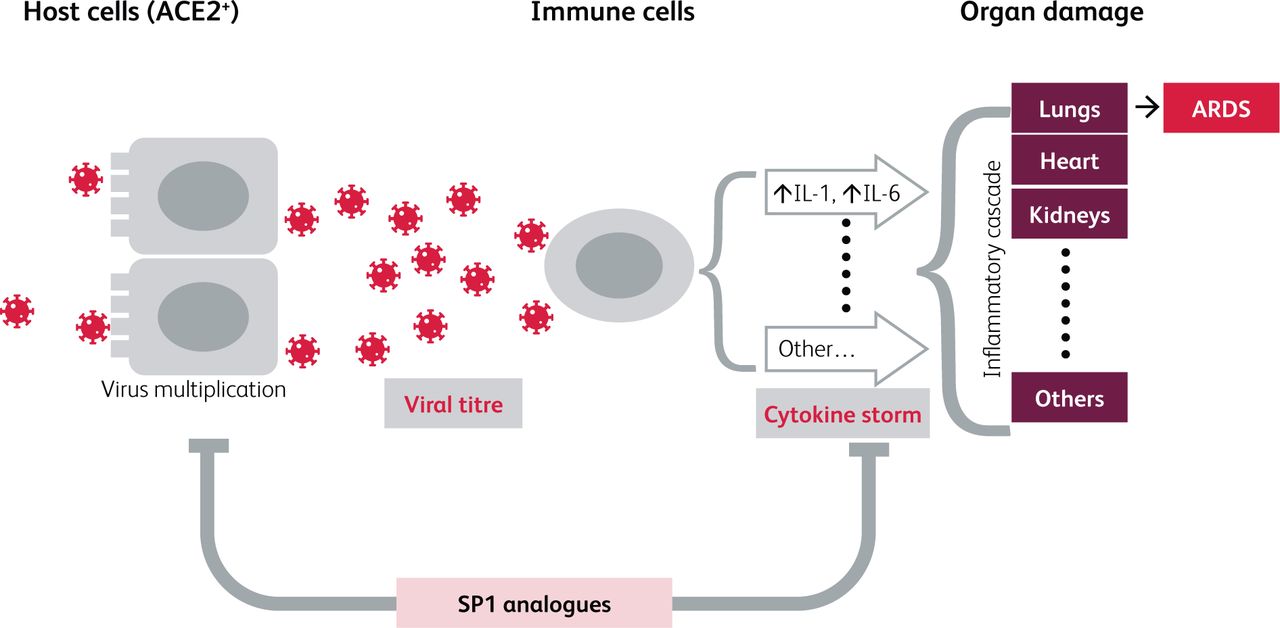
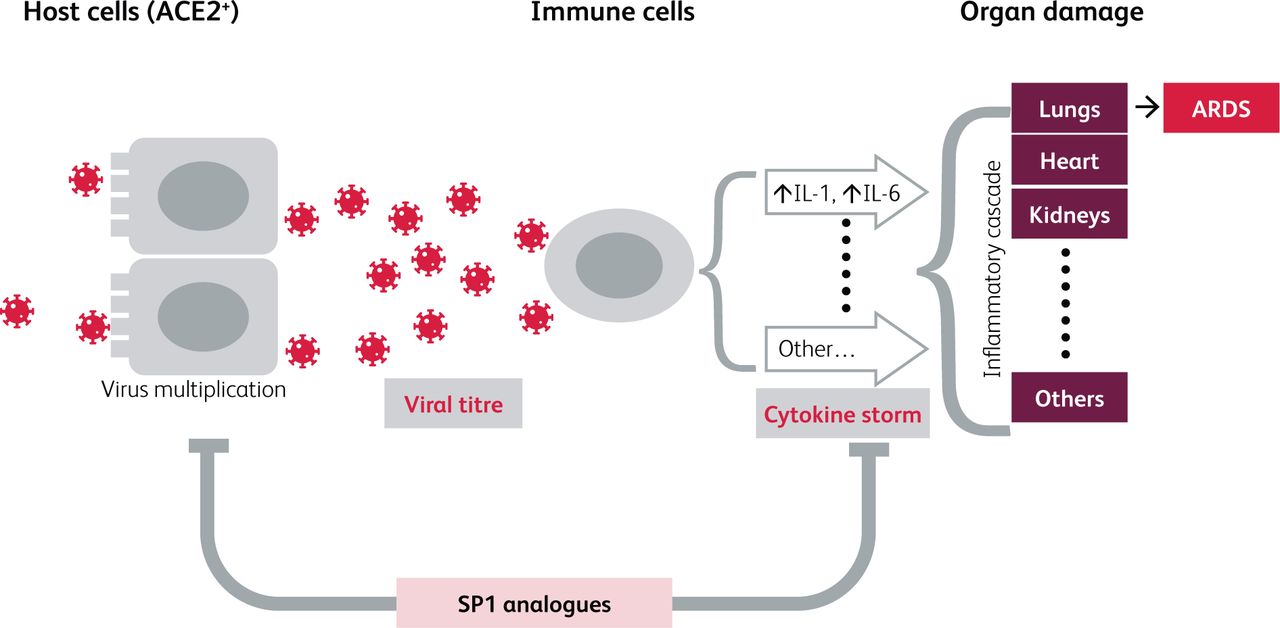
Mechanism of SARS-CoV-2-associated cytokine storm and associated cytokine storm-induced damage. Infection with SARS-CoV-2 in host (ACE2+ cells) cells followed by replication leads to high virus titre and stimulation of immune cells (eg macrophages, neutrophils, basophils) to produce and release high levels of cytokines (‘cytokine storm’). The cytokine storm causes an adverse inflammatory cascade that damage several organs. Damage to the lungs leads to acute respiratory distress syndrome (ARDS). SP1 analogs have the potential to inhibit virus multiplication as well as to decrease the intensity of the cytokine storm.21,36
There is therefore strong evidence that FTY720 has some type of ‘pancytokine’ or at least ‘polycytokine’ inhibiting properties and may therefore show more beneficial effects compared to selective cytokine inhibitors. At the same time, a polycytokine/pancytokine inhibitor may have more adverse effects. COVID-19 being a relatively new disease, information regarding the risk/benefit of targeting multiple cytokines is lacking. To our knowledge, there is only one ongoing clinical trial (at the recruiting stage) that proposed the use of fingolimod in patients with new coronavirus pneumonia (www.clinicaltrials.gov; NCT04280588). It is important to mention that in this clinical study the primary outcome measured is the change of the pneumonia severity after 5 days of treatment. Thus, the aim of this clinical trial is not to evaluate the preventive property of fingolimod on disease progression but its ability to change the severity once the pneumonia is already present.
Rationale for the use of sphingosine analogues as early adjuvant therapy
There are several reasons why it may be beneficial to use FTY720 at an earlier stage of infection to prevent or mitigate the severity of ALI/ARDS. First, while it is not known exactly when the cytokine storm starts in COVID-19 patients, cytokine levels at the time of admission to hospital are already several times higher than normal6 and thus preventing the rise of these cytokines at earlier stages may hold the key to mitigating the severity of the disease and decreasing hospital admissions. Second, infectious complications are relatively low in patients receiving sphingosine modulators.26 FTY720 has been prescribed for patients with relapsing-remitting multiple sclerosis to prevent the acute attacks since 2010 with good tolerability.17 Remarkably, the incidence of adverse events in patients treated with FTY720 for 12 and 24 months (the duration of treatment ranges from 6 to 24 months) was 7% and 14.8% and no death was reported even after 24 months of treatment.17 It is important to mention that when compared to placebo the incidence of adverse effects, while statistically significant, is not strikingly different (fingolimod 14.8% vs placebo 12.7%).17 This observation suggests that FTY720 when administered for shorter periods (2-3 weeks) as we propose will be relatively safe.
Case studies reporting outcomes in COVID-19 patients who were already being treated with fingolimod for their MS using provide another rationale for the use of sphingosine analogues as early adjuvant therapy. Barzegar et al reported the positive outcome of a 42-year-old woman infected with COVID-19 with multiple comorbidities including multiple sclerosis, which was being treated with fingolimod.27 Malluci et al28 reported two cases of MS patients on fingolimod treatment who tested positive for COVID-19 but did not develop any symptoms, signs, or complications. Similar benign29 or more severe symptomatic but non-fatal30–32 cases of COVID-19 were reported in MS patients taking fingolimod. Conversely, an exacerbation of COVID-19 symptoms was observed when fingolimod was discontinued in one case report.33 A severe COVID-19 infection in a MS patient treated in whom fingolimod was discontinued was also reported; it is not clear when fingolimod was stopped34 but it is likely that the drugs were discontinued upon hospital admission due to concern that immunosuppression may worsen COVID-19.32
In addition, there are other novel sphingosine analogues available to treat MS such as siponimod (Mayzent), ozanimod (Zeposia) and ponesimod (not yet approved) that can be considered as alternatives. It was recently suggested that immunosuppression in MS may play a protective role in these patients.35 If this suggestion is proven in larger studies, other drugs used for the treatment of MS should be evaluated for their potential protective/preventive role in the progression of COVID-19 disease. Finally, recent in vitro data (from an article still in the preprint stage) demonstrated that non-toxic concentrations of fingolimod produced a 38.4-fold decrease of SARS-CoV-2 viral titer as compared to the DMSO control.36
Conclusions
The rationale to consider sphingosine analogues currently approved for the treatment of MS has been recently suggested by others.37 It use as early adjuvant therapy is supported by strong experimental data in other conditions relevant to COVID-19 disease as well as by recent several case reports with positive outcomes in COVID-19 patients taking fingolimod for MS treatment. Sphingosine analogues are relatively safe and well tolerated even when administered for prolonged times.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.