
Abstract
The emergence of SARS-CoV-2 has proven to be a challenge to healthcare bodies globally. The virus has been associated with a spectrum of clinical features, from anosmia to gastrointestinal upset to multiorgan dysfunction in the most severe cases. Given the range of features observed, it is important to be aware that infectious diseases can present atypically. Furthermore, in many hospitals, including our own, teenagers aged 16 to 18 years old are admitted under the care of adult medical services. Clinicians should be aware of patients presenting with the novel condition of paediatric inflammatory multisystem disorder – temporarily associated with SARS-CoV-2 (PIMS-TS).
Case presentation
A previously fit and well 16-year-old male patient with no prior health issues presented to a district general hospital with a history of fever, headache, vomiting and malaise. He reported that his fever started 5 days prior to admission and his headache was central, worsened by sudden movement and leaning forward but not associated with any photophobia or new neurology. The abdominal pain and vomiting (non-bilious) started 2 days before presenting to the emergency department.
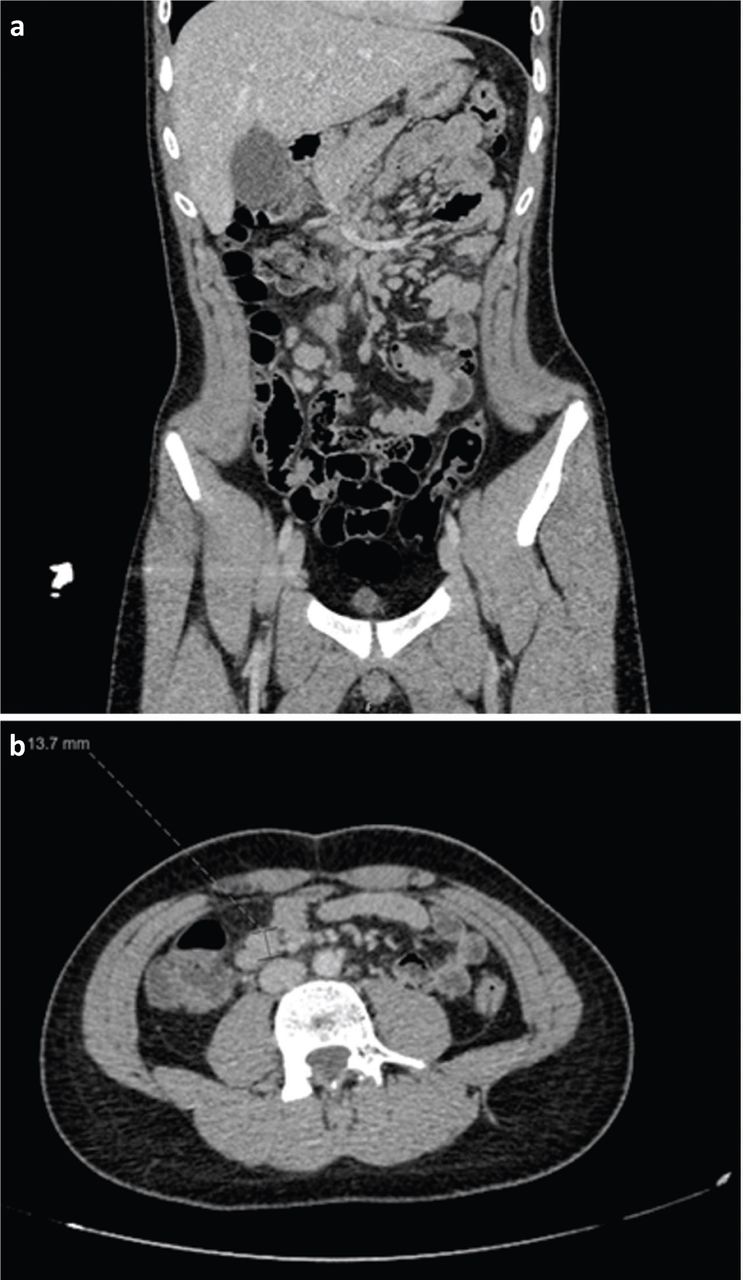
On admission he was febrile (37.6°C) and tachycardic (133 beats per minute), with otherwise normal observations. Examination findings included tenderness in the right iliac fossa (RIF) and a blanching rash on his lower back. Blood tests revealed elevated C-reactive protein (CRP; 183 mg/L), white blood cells (WBC; 12.9 × 109/L), neutrophils (10.8 × 109/L) and international normalised ratio (INR; 1.3). Liver function was also deranged with low total protein (52 g/L), albumin (28 g/L), globulin (23 g/L) and alkaline phosphatase (49 U/L). A surgical review was sought, and they recommended radiological imaging. Contrast computed tomography (CT) of the chest, abdomen and pelvis showed multiple enlarged mesenteric nodes, especially in the RIF, possibly in keeping with mesenteric adenitis (Fig 1). The visualised appendix was unremarkable and both lung fields were clear. All other abdominal and pelvic viscera were unremarkable.
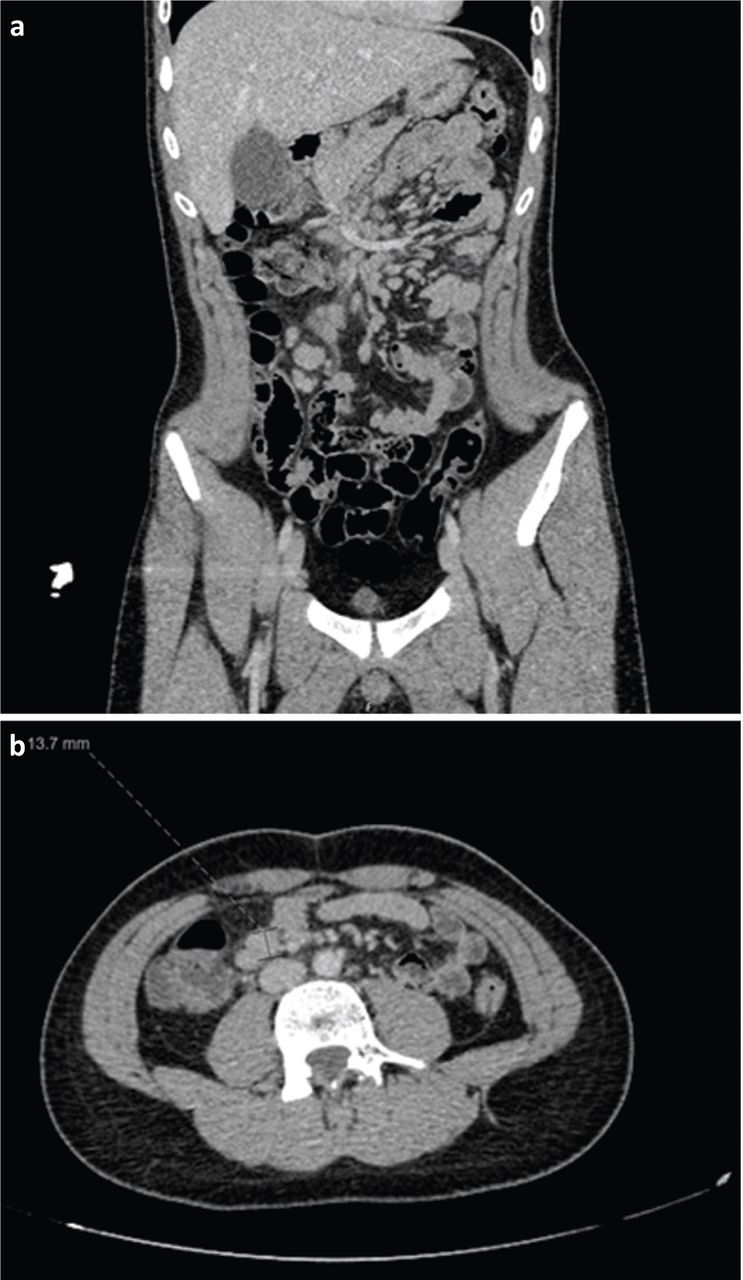
Contrast computed tomography of the chest, abdomen and pelvis showing multiple enlarged mesenteric nodes, especially in the RIF, possibly in keeping with mesenteric adenitis.
As appendicitis was ruled out by the surgical team, he was started on intravenous (IV) aciclovir 600 mg, 3 times a day, and IV ceftriaxone 2 g, 12 hourly, to cover for meningitis. He also received IV fluids and regular paracetamol to treat his fever. A lumbar puncture was planned to investigate for meningitis after CT of the head was done. The patient was reluctant to have CT of the head due to radiation and so magnetic resonance imaging (MRI) of the head was performed 6 days after admission which showed normal brain, brainstem and cerebellum, with no abnormal parenchymal enhancement or any leptomeningeal disease. Subsequent to this, a lumbar puncture was performed which showed no evidence of meningitis (Table 1). Throughout his admission, he developed diarrhoea, had a temperature daily (maximum 39.5°C) and remained tachycardic (maximum 142 beats per minute). He also began exhibiting bilateral conjunctivitis, peripheral oedema of his hands and complained of arthralgia in his knees. There was no evidence of palpable cervical lymphadenopathy or a strawberry tongue. Despite being on ceftriaxone and aciclovir for an extended period, his CRP remained elevated, he developed a normocytic anaemia, thrombocytosis and had persistently low albumin (Table 2). Other significant positive tests were a raised erythrocyte sedimentation rate (ESR; 33 mm/hour), lactate dehydrogenase (262 U/L), N-terminal pro-brain natriuretic peptide (3,885 pg/mL), troponin (21 ng/L) and ferritin (418 μg/L). Significant negative tests include two SARS-CoV-2 swabs, blood cultures, urine/stool cultures, connective tissue screens and infective screens (Table 1).
Infectious disease and special test results undertaken at the district general hospital during the patient's 8-day admission
Laboratory results from the district general hospital over the patient's 8-day admission
Further surgical input was sought in light of the continuing abdominal pain and poor response to antibiotics on day 7. An abdominal ultrasound showed enlarged lymph nodes in the RIF and a small volume of free fluid. The appendix was not positively visualised. The surgical team were again confident appendicitis was not the cause for his presentation.
Echocardiography (ECHO) was performed which showed normal coronary artery dimensions, mild aortic regurgitation, normal biventricular size and systolic function and a left sided pleural effusion. The case was discussed with the infectious disease team at a specialist children's hospital for further advice. They requested urgent transfer of the patient to their care for initiation of IV immunoglobulins (Ig) and aspirin as a treatment of SARS-CoV-2 hyperinflammatory syndrome resembling atypical Kawasaki disease.
While at the specialist hospital, it was decided that as he was improving (evidenced by his inflammatory and cardiac markers and clinical state) then IVIg was not needed and instead was treated with aspirin 75 mg once a day (OD). He had a repeat ECHO after a further 2 days which showed a small pleural effusion and normal coronary arteries. He was discharged with aspirin 75 mg OD and outpatient follow-up. His formal diagnosis was paediatric inflammatory multisystem disorder – temporarily associated with SARS-CoV-2 (PIMS-TS).
He was readmitted 4 days later due to new moderate biventricular impairment on ECHO, and rising ferritin and d-dimer levels. After a period of monitoring and an increase in the aspirin dose, ECHO changes returned to normal. He was discharged again after 6 days. His eyes were still mildly erythematous and had some residual minimal abdominal pain, but he remained otherwise well.
Subsequent cardiac CT and MRI of the heart, lungs, abdomen and pelvis were normal. A repeat SARS-CoV-2 swab and stool PCR were again both negative.
Discussion
Following the outbreak of SARS CoV-2, clinicians in multiple countries have been reporting disparities in the effects the virus is having on children compared with adults. Interestingly, not only have children seemingly been protected from the worst effects of the virus, there have also been cases of children presenting with symptoms consistent with hyperinflammatory syndrome, akin to atypical Kawasaki disease.1
Kawasaki disease is an acute systemic inflammatory vascular disorder commonly affecting children, with peak incidence under the age of 5 years old.2 It has shown to have a mortality rate of 0.17% in an American study, largely resulting from cardiac complications.3 Strict criteria have been defined when diagnosing the classical variant of the disease which include fever of unknown origin for ≥5 days, plus four of the following five requirements: bilateral conjunctivitis; changes to oropharyngeal mucous membranes (including injected and/or fissured lips, strawberry tongue and enanthema); palmar and/or plantar erythema and/or periungual desquamation (in convalescent phase); polymorphous exanthema; and primarily truncal (not vesicular nor cervical) lymphadenopathy (at least one lymph node >1.5 cm).4 However, patients who do not meet these criteria may still fulfil the requirements of incomplete or atypical Kawasaki disease as described by the American Heart Association.5
These new hyperinflammatory syndrome with atypical Kawasaki disease features during the SARS-CoV-2 era cases have been given the new term PIMS-TS. The increasing prevalence of such cases has led to the Royal College of Paediatrics and Child Health (RCPCH) developing a case definition for PIMS-TS (Box 1).6 The literature surrounding PIMS-TS is understandably scant with the diagnostic criteria only being recently published (Table 3).6 Treatment options remain similar to those utilised in the management of Kawasaki disease although no rigorous guidelines have been issued. IVIg, aspirin and steroids have all been trialled according to a study conducted at a UK tertiary children's hospital. All 15 of the patients included in their study were discharged home with a median inpatient stay of 12 days.7 Elsewhere, biological agents such as infliximab and anakinra have also been used in patients not responding to the treatments described previously.8 In that study, out of 58 patients included, 5% were given anakinra and 14% were given infliximab with one death out of the whole study population.
Royal College of Paediatrics and Child Health paediatric inflammatory multisystem disorder – temporarily associated with SARS-CoV-2 diagnostic criteria6
Royal College of Paediatrics and Child Health case definition of paediatric inflammatory multisystem disorder – temporarily associated with SARS-CoV-26
Conclusion
As SARS-CoV-2 cases continue to rise globally, it is important for clinicians to be aware of the threat that the virus poses for the paediatric population. We must therefore be vigilant when faced in the current climate with cases in which there is evidence of a hyperinflammatory response, with or without a SARS-CoV-2 positive test. It is important to note that the World Health Organization (WHO) PIMS-TS criteria require a positive SARS-CoV-2 test result, however, literature has shown that PCR testing is not reliable.7 It is predicted that with a more reliable and widely available test that this aspect of the criteria will change from the RCPCH to fall in line with WHO.
Early input should be sought from a specialist paediatric centre and PIMS-TS associated laboratory tests should be sent promptly. This will provide the best outcomes for patients by allowing for a multidisciplinary discussion and prompt initiation of treatment.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.