
ABSTRACT
Objectives We aimed to assess the frequency and nature of financial conflicts of interest among both the guideline committee authors and the authors of research studies used to support the European Society of Cardiology (ESC) guidelines.
Design We evaluated the competing interests of the doctors that write five of the key ESC clinical practice guidelines (CPG): valvular heart disease (VHD), atrial fibrillation (AF), pericardial diseases (PD), heart failure (HF) and myocardial revascularisation (IHD). In addition, we examined the funding sources of studies cited in the recommendations that were related to pharmaceutical agents. If a study was sponsored by industry, the disclosures of all authors were reviewed to assess whether there was a financial conflict of interest with the study funder.
Results In total, there were 603 recommendations (PD 112, VHD 111, HF 169, IHD 97 and AF 114) across the five guidelines, of which, 271 (45% (PD 26, VHD 23, HF 72, IHD 84 and AF 66)) related to pharmaceutical agents. At least 80% of guideline committee authors, except for the PD guidelines, had a relevant financial conflict of interest, with the most frequent being a direct personal payment (68–82%). Industry support for studies varied across the guidelines from 5% (PD) to 65% (IHD). If a study was funded by industry, authors were frequently (55–90%) conflicted with the industry sponsor.
Conclusions The majority of the doctors that write clinical guidelines have a relevant financial conflict of interest. In addition, industry sponsorship of studies is frequent, and authors are often conflicted with the study funder. We propose that physicians that write clinical guidelines should be free of such financial conflicts of interest to maintain scientific integrity and independence in the clinical guidelines.
Introduction
Clinical practice guidelines (CPGs) are produced to optimise and standardise patient care by making evidence-based recommendations. These CPGs are developed by committees of experts within the field, which usually comprises a task force of ‘authors’ and document ‘reviewers’. These practice-defining guidelines have substantial implications for clinicians, institutions that provide healthcare, pharmaceutical companies (industry) and, most importantly, patient care.1 Clinical recommendations within the guidelines are formed because of the guideline committee members’ interpretation of available evidence. This creates two potential opportunities for industry to exert influence: the studies used as evidence and the way these studies are interpreted.
A conflict of interest (CoI) is ‘a set of circumstances that creates a risk that professional judgement or actions regarding a primary interest will be unduly influenced by a secondary interest’.2 While financial CoIs (FCoIs) are the focus of much research and commentary, there are also important non-financial CoIs, such as ‘intellectual’ CoIs.1 Intellectual CoIs are ‘academic activities that create the potential for an attachment to a specific point of view that could unduly affect an individual’s judgment about a specific recommendation’.3 These are often subtle and pervasive, making their assessment more challenging.1
Industry spends significant sums of money on relationships with healthcare organisations and professionals because FCoIs have been demonstrated to change practice.4,5 However, collaboration with industry facilitates development of new therapies and technologies that can improve patient care.6 It is therefore important not to abandon collaborative working with industry but to aim to strike a balance between joint endeavour and financial reward while preserving the integrity and independence of the processes involved in guideline development.
Given the importance of CPGs to clinical practice and the data demonstrating the potential impact that FCoIs have, we sought to review the frequency of these conflicts (among those that write the clinical guidelines as well as the research study authors) in relation to five of the European Society of Cardiology’s (ESC) CPGs: valvular heart disease (VHD), atrial fibrillation (AF), pericardial diseases (PD), heart failure (HF) and myocardial revascularisation (IHD).7–11
Methods
We first extracted the financial disclosures from the supplementary documentation for each of the five guidelines for all 220 guideline contributors (categorised by the ESC as authors / task force members and document reviewers). These disclosures are divided into five categories by the ESC (listed in Box 1). These declarations were reviewed and classed as an FCoI if these relationships were relevant to any part of the guideline; this included relationships with the pharmaceutical drug, device, imaging and any other industries that could benefit from recommendations within that guideline.
Types of financial conflict of interest with the pharmaceutical industry as defined by the European Society of Cardiology
In the second aspect of the study, we analysed all recommendations related to pharmaceutical (medication) agents. For each of these recommendations, we noted the corresponding class of recommendation (CoR) and level of evidence (LoE). All references used to support these recommendations were then reviewed. We noted whether the studies were partly or fully funded by industry and, if so, the disclosures of all study authors were reviewed to ascertain whether the authors had a direct CoI with the industry study sponsor. If no disclosures were available for review, this was recorded.
Results
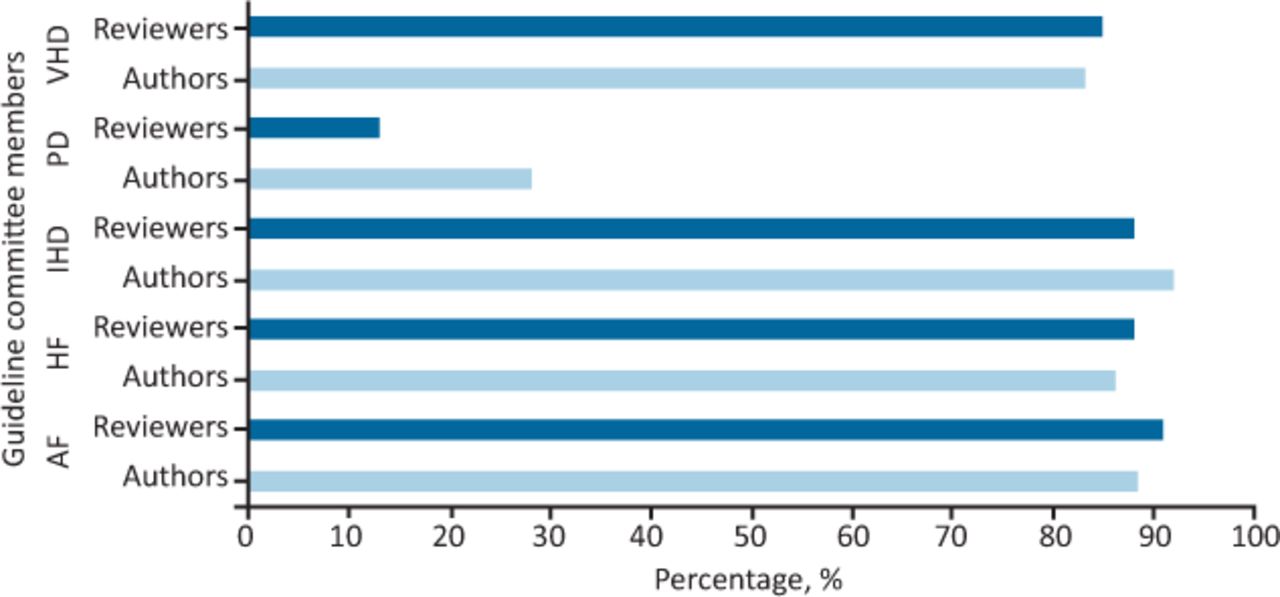
Disclosures were available for all 220 contributors to the five guidelines. The vast majority of guideline authors/reviewers had a direct FCoI with industry (illustrated in Fig 1). The most common relationship with industry in all the guidelines except PD was a direct personal payment, which was observed in 68–82% of guideline authors and 69–76% of guideline document reviewers. Table 1 lists the breakdown of the FCoIs among the guideline committee members. As revealed in this table, in four of the five guidelines (IHD, AF, VHD and HF), the majority of guideline authors and reviewers received direct personal payments from industry; ranging from 68% (IHD) to as high as 82% (AF). Such payments were uncommon in the PD guideline.

Frequency of any financial conflict of interest among guideline committee members. AF = atrial fibrillation; HF = heart failure; IHD = myocardial revascularisation; PD = pericardial diseases; VHD = valvular heart disease.
Breakdown of the type of financial conflict of interest for guideline committee members
In total, there were 603 recommendations (PD 112, VHD 111, HF 169, IHD 97 and AF 114) across the five guidelines, of which, 271 (45% (PD 26, VHD 23, HF 72, IHD 84 and AF 66)) related to pharmaceutical agents. There were a small number of references for which no funding data was available (AF 5, HF 4, IHD 2, PD 4 and VHD 1), for analysis purposes, these were included in the total number of studies.
Industry sponsorship for the studies that were used to support the pharmaceutical recommendations was observed in a total of 152/360 (42%) studies. This ranged from just 5% support in the PD guideline (1/20 studies) to 65% in the IHD guideline (62/96 studies). Industry support for studies related to pharmacological agents in the AF, HF and VHD guidelines was present in 25% (30/121 studies), 46% (51/112 studies) and 64% (7/11 studies), respectively. There were no author disclosures available in a small number of studies funded by industry (AF 8, HF 12, IHD 12, PD 0 and VHD 0). Fig 2 demonstrates that, except for PD, authors of these studies frequently had an FCoI with the industry sponsor, irrespective of the level of evidence of the study. Indeed, in the HF and AF guidelines, the vast majority of authors of studies cited in the guidelines at the lowest level of evidence (level of evidence C) had relevant financial conflicts with study the sponsors.

Percentage of authors with a financial conflict of interest with the study funder by guideline and level of evidence. AF = atrial fibrillation; HF = heart failure; IHD = myocardial revascularisation; PD = pericardial diseases; VHD = valvular heart disease.
Discussion
There are two principal findings of our study. The first is that financial conflicts are extremely prevalent among the individuals that write five of the key ESC clinical guidelines. The second major finding is that, in four of the five guidelines we analysed, most authors of studies cited in support of pharmaceutical recommendations also had a direct FCoI with the study sponsor.
We believe that this is the first such analysis of key practice guidelines issued by a major international cardiovascular organisation, but our results are consistent with studies examining this issue in other areas of medicine. FCoIs have been frequently reported in CPG committee members across a range of specialties.12–14 This observation is likely to be an underestimate because FCoIs are often both under and inaccurately reported.12,13,15 Interestingly, authors of government-sponsored CPGs are less likely to have a direct FCoI compared with other sources of CPGs.12 Neuman et al analysed 14 CPGs related to diabetes and dyslipidaemia published between 2000–2010.12 Panel members from government-sponsored CPGs were significantly less likely to have a CoI compared to CPGs issued by non-governmental sources (16% vs 69%; p<0.001).12 George et al analysed two CPGs related to management of idiopathic thrombocytopenic purpura (ITP).14 One CPG was issued as an international consensus report (ICR) and was supported by companies that manufacture products used in the treatment of ITP. The majority (73%) of ICR panel members had financial CoIs with associated industries. A second CPG was issued by the American Society of Hematology (ASH) who chose panel members based upon a lack of competing interests. The authors found that the ICR panel produced considerably stronger recommendations for the use of agents manufactured by companies from which panel members had received financial support than the authors of the ASH-sponsored CPG, demonstrating that CoI among CPG authors influences recommendations.14 Of further concern, bias has been shown often to result in an overestimation of benefit and to trivialise harm.1,14
Our study does, however, highlight that at least 10% of guideline committee members had no FCoIs. These data support the observation that there is a body of experts available that do not have FCoIs who could be used for guideline committees.15 Further measures, as have been adopted by both the National Institute for Health and Care Excellence (NICE) and recently by the American College of Physicians (ACP), can be used to grade the relevance of a FCoI for a particular guideline and potentially exclude those with significant FCoIs from partaking in discussion or voting upon recommendations (Table 2).16,17
Classification of conflict of interest and action taken in the American College of Physicians’ guidance for management of competing interests among guideline authors17
The significantly lower prevalence of CoIs among study authors and guideline authors/reviewers in the PD guideline is not surprising, as the majority of pharmaceutical recommendations in PD relate to generic medications such as aspirin, non-steroidal anti-inflammatory drugs, corticosteroids and colchicine, for which industry has no pecuniary interest.
In common with previous studies and the observation that industry now provides the largest source of funding for clinical trials in the USA, our analysis has demonstrated that a significant proportion (up to 64%) of studies used to support the ESC guidelines are either fully or partially funded by industry.2,18–20 Furthermore, our study supports previous observations that the authors of these studies are frequently conflicted with the study funder.18,20–23 There is much evidence to suggest that studies are more likely to be positive and the objectivity of reporting is likely to be reduced when authors have an FCoI.23,24 These observations are likely to be an underestimate given that self-reporting of FCoIs is often inaccurate.22,25 Importantly there is no evidence to suggest that studies not supported by industry are of poorer quality.26
Limitations
This study focused on five guidelines which were chosen because they covered a broad range of clinical cardiology; it is, however, not possible to be certain that these findings are representative of other guidelines. This study is descriptive and therefore unable to assess whether the declared FCoIs resulted in changes in reporting and recommendations. It is not possible to corroborate the documented disclosures; this raises the possibility that we may have underestimated the magnitude of the issue.12,13,15,22,25 Finally, this study assessed for financial CoIs and not intellectual CoIs. This assessment is important but challenging because intellectual CoIs are often subtle and pervasive but also powerful motivators for research.27 The inclusion of a group of authors with different backgrounds may provide some balance to discussions and could be used as a strategy to reduce the influence of intellectual CoIs on CPGs. In addition, the recent ACP update on management of CoIs does have a method for dealing for non-financial CoIs (for example, a moderate-level CoI could be ‘an intellectual interest that might lead to cognitive bias or relationships with entities that might profit by association with the guidelines’) and this leads to exclusions in authorship and voting for guidelines (though permits participation in discussions).17
Conclusion
Financial CoIs are frequent among doctors that author influential clinical practice guidelines, as well as among researchers that produce studies used to support recommendations for pharmaceutical agents in the guidelines.
Summary
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- National Institute for Health and Care Excellence (NICE) guidance on heart valve disease
- National Institute for Health and Care Excellence (NICE) guidance on heart valve disease
- Quality of reporting among systematic reviews underpinning the ESC/ACC guidelines on ventricular arrhythmias and sudden cardiac death
- Balancing conflicts of interest during cardiology training: why does industry buy your lunch?