
ABSTRACT
Hydrogen therapy is a very promising treatment against several diseases due to its mild attributes, high affinity and inherent biosafety. However, there is little elaboration about current hydrogen treatment in liver diseases. This article introduces the administration of hydrogen and mechanisms of hydrogen therapy in vivo, including modulating reactive oxygen species, apoptosis and autophagy, and inflammation, affecting mitochondria, as well as protein transporters. The major focus is clinical hydrogen use and related mechanisms in liver dysfunction or diseases, including non-alcoholic fatty liver disease, hepatitis B, liver dysfunction caused by liver tumour and colorectal tumour chemotherapy. Further, the article reveals ex vivo hydrogen application in liver protection. Finally, the article discusses the current and future challenges of hydrogen therapy in liver diseases, aiming to improve knowledge of hydrogen therapy and provide some insights into this burgeoning field.
Introduction
Molecular hydrogen (H2) is atomically the smallest gas, with trace amounts in the atmosphere. It can diffuse readily through the body as well as cells.1,2 Hydrogen therapy has been reported to be effective in many kinds of disease.3–7 The possible mechanisms of hydrogen therapy can be attributed to its selective antioxidant and anti-inflammatory effects.8–13 Different administrative ways, molecular mechanisms and clinical applications of hydrogen therapy in liver diseases will be discussed.
Administration of hydrogen therapy in liver diseases
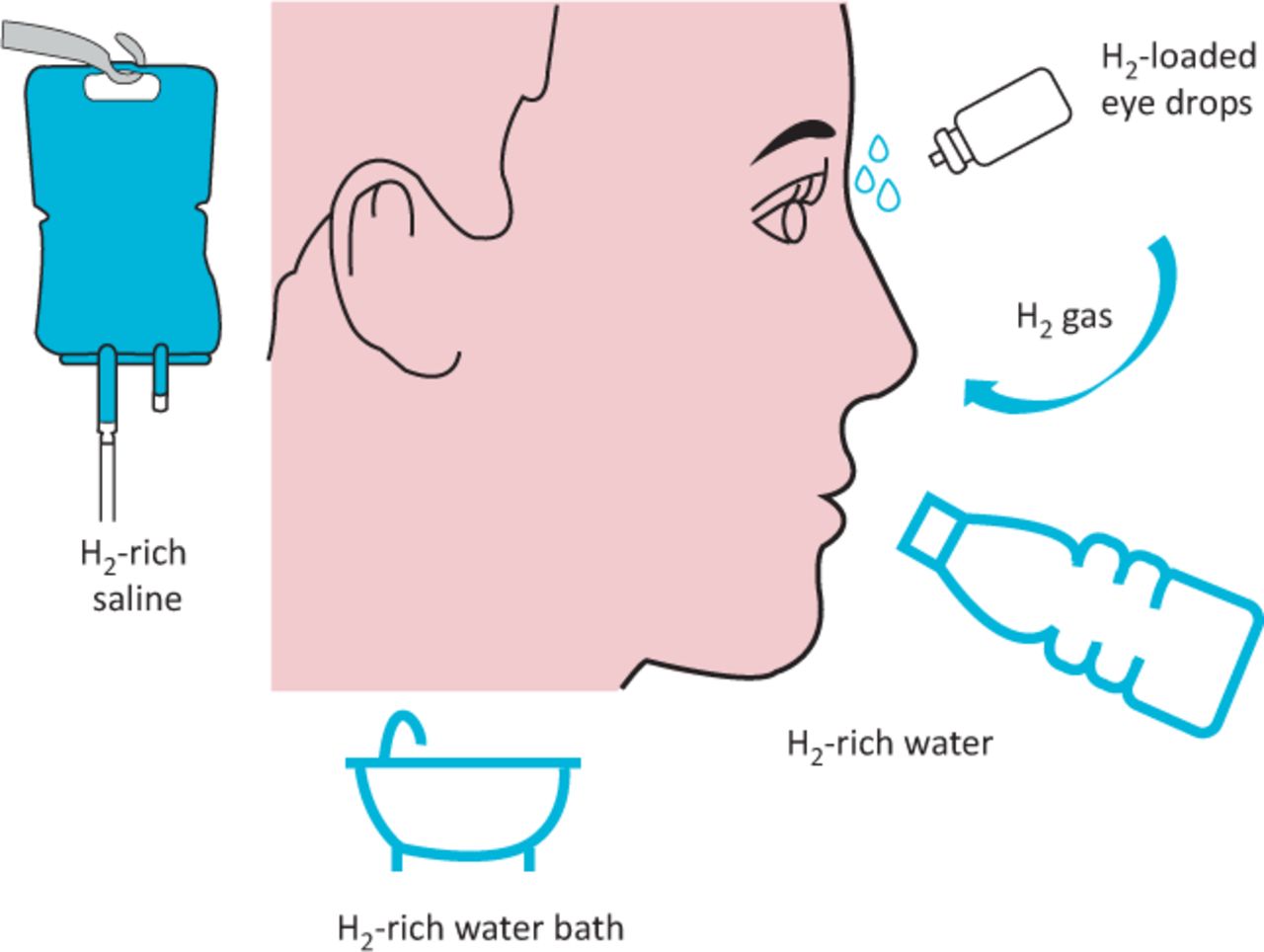
The most common ways to administer hydrogen as a treatment are injecting hydrogen-rich saline (HRS), inhaling hydrogen gas, drinking hydrogen-rich water (HRW), taking an HRW bath and dripping hydrogen-loaded eye drops (Fig 1). The first three are most frequently used for treatment of liver diseases. Hydrogen dissolved in a solution such as saline or another solution could be injected into the digestive tract or peritoneal cavity and applied in liver diseases. HRW is also called hydrogen-dissolved water or hydrogen-enriched water. It is produced by placing a magnesium stick into drinking water (Mg + 2H2O → Mg(OH)2 + H2) or by dissolving hydrogen gas in water under high pressure to a supersaturated level using an HRW-producing apparatus.14 HRS can be made by dissolving hydrogen in physiological saline solution (0.9%) under high pressure. HRS can provide accurate concentrations of hydrogen into the body. However, the most common method of hydrogen therapy administration is inhaling hydrogen gas, because it is can be inhaled through nasal cannulae, ventilators, facemasks or gas chambers very easily and has no peculiar smell.

Different methods of administration of hydrogen therapy. H2 = hydrogen.
Molecular mechanisms of hydrogen therapy
The exact molecular mechanisms of hydrogen therapy still have some academic controversies in the scientific community. Many recent studies have shown that hydrogen plays its biological role primarily through four main mechanisms: anti-inflammation, anti-oxidation, signal modulation and cytoprotection involved in mitochondria, endoplasmic reticulum and membrane proteins.
Hydrogen’s role as an excellent natural antioxidant and free radical scavenger has been confirmed by many previous studies.15–18 It can decrease reactive oxygen species (ROS) by reducing peroxynitrite (ONOO–) and hydroxyl radicals (•OH), or increasing superoxide dismutase (SOD) and malondialdehyde (MDA).19 Recently, it has been reported that hydrogen may be able to inhibit pathways such as GRP78, TRAF and IC3B-II as a result of its ability to participate in signal modulation and cytoprotection.20,21 It has also been shown that molecular hydrogen is able to serve as an effective therapeutic strategy for liver injury through the regulation of FUNDC1-dependent mitophagy.22 Also, hydrogen was reported to modulate pro- and anti-inflammatory factors including interleukin (IL)-6, IL-10, high-mobility group box 1 (HMGB1), caspase 1, vascular endothelial growth factor (VEGF) etc.23 These important pathways should be heavily investigated further since they are involved with inflammatory responses, gene regulation and apoptosis. Although hydrogen has been strongly implicated in reducing oxidative stress, it has been proposed that hydrogen affects signalling mechanisms and can also induce cytoprotective factors.24,25 A brief overview of molecular mechanisms based on the most recent achievements of research is shown in Fig 2.

Molecular mechanisms of hydrogen therapy. CAT = catalase; H2 = hydrogen; •OH = hydroxyl radicals; ONOO– = peroxynitrite; ROS = reactive oxygen species; SOD = superoxide dismutase.
Animal experiments
In a mouse model of acetaminophen-induced liver injury, drinking HRW resulted in a significant increase in the 5-day survival rate. HRW could produce a noticeable improvement in liver function. HRW could reduce the inflammation indicator IL-6 significantly. Furthermore, it could reduce acetaminophen-induced phosphorylation of Jun kinase (JNK) and activation of CYP2E1. Simultaneously, HRW could facilitate hepatocyte mitosis to promote liver regeneration.26 It is biologically safe under the condition of 20 mL/kg/day for 28 days via intragastric infusion in rats and is effective at suppressing hepatic injury caused by ischaemia–reperfusion through alleviating oxidative stress.27 The genes of oxidoreduction-related proteins, including hydroxymethylglutaryl co-enzyme-A reductase, were significantly enriched in the livers of rats after drinking HRW.28 Hepatocyte death induced by antimycin A was significantly suppressed after culturing in hydrogen-rich medium. However, this did not suppress hepatic stellate cell activation.29
In an animal model of non-alcoholic steatohepatitis (NASH), plasma alanine aminotransferase (ALT) levels, hepatic expression of tumour necrosis factor-α (TNF-α), IL-6 and oxidative stress biomarker 8-hydroxydeoxyguanosine (8-OHdG), and apoptosis marker terminal deoxynucleotidyl transferase-mediated dUTP–biotin nick end labelling (TUNEL)-positive cells in the liver were decreased in the HRW group. In a NASH-related hepatocarcinogenesis model, the number of tumours was significantly lower in the HRW group compared with control.14 These results indicate that HRW may be an effective treatment for NASH or liver cirrhosis.
In an animal model of lipopolysaccharide (LPS)-induced acute liver dysfunction, treatment with HRS prolonged the median survival time and reduced liver dysfunction. Also, HRS can significantly reduce pathological alterations in liver tissues, such as the level of serum IL-6, TNF-α levels, ballooned hepatocytes, and myeloperoxidase (MPO) and MDA levels in liver tissues (p<0.05). Cell apoptosis was detected in liver tissues after LPS treatment, and attenuated by HRS treatment.30 HRS also decreased phosphorylated extracellular signal-regulated kinase (p-ERK), phosphorylated Jun kinase (p-JNK), nuclear factor-kappa B (NF-κB), and second mitochondria-derived activator of caspase (Smac) levels, and increased p38 activation (p<0.05). Thereby, HRS may attenuate LPS-induced acute liver dysfunction in rats, possibly by reducing inflammation and cell apoptosis.31 In rats with 90% hepatectomy, HRS was also found to attenuate the massive hepatectomy-induced liver injury and the progression to acute liver failure, not only by the attenuation of oxidative damage but also by decreasing the production of inflammatory cytokines, such as TNF-α, IL-6 and HMGB-1, in part through the inhibition of NF-κB activation.32
In an obstructive jaundice rat model, liver injury was evaluated microscopically 10 days after bile duct ligation (BDL) and aspartate aminotransferase (AST) levels, tissue MDA content, myeloperoxidase activity, TNF-α, IL-1β, IL-6 and HMGB1 levels were all increased significantly by BDL. HRS reduced levels of these markers and relieved morphological liver injury. The protective effect of hydrogen in liver was revealed by liver haematoxylin and eosin pathological staining and detecting liver function in rats.33 Treatment for 2 weeks had significant protective effects on liver injury, namely improvement of haemodynamics, decreased fibrosis, increased NOSII activity, increased antioxidant enzyme activity, decreased lipid peroxide levels and circulating TNF-α levels.
In a cell culture model of hepatic steatosis, hydrogen could exhibit beneficial physiological effects on lipid metabolism. A high volume of hydrogen, such as in an atmosphere that contains 75% H2, 20% O2 and 5% CO2, has no obvious impact on viability of HepG2 cells. Hydrogen treatment can also reduce the expression of CD36 protein, while it has no significant effect on CD36 mRNA expression. The same result, ie that inhalation of hydrogen gas could reduce liver injury, was observed in swine that underwent 70% hepatectomy. In the group that inhaled 2% hydrogen by tracheal intubation, the level of inflammatory cytokines including TNF-α and IL-6 after hepatectomy was significantly lower; liver function was also ameliorated. Microphotometric evaluation of apoptotic index in TUNEL-stained tissue after hepatectomy indicated that the morphological change of liver injury was relieved.34,35 Further research used different concentrations of hydrogen gas (1, 2 and 3%) administered for 1, 3 or 6 hours. In rats that inhaled 2% hydrogen gas for 1 hour prior to liver transplantation, marked reductions in IL-6, TNF-α, Egr-1 and IL-1β expression as well as increased mRNA expression levels of NF-κB, anti-apoptotic genes HO-1, Bcl-2 and A20 were discovered. These results revealed that hydrogen gas activated the NF-κB signalling pathway.36 Hydrogen gas inhalation also attenuates sepsis-induced liver injury in a FUNDC1-dependent manner, which protects against sepsis-induced liver injury in vivo and ameliorates liver injuries through the regulation of mitophagy.37,38 Together, hydrogen gas presents wide potential use in liver diseases; however, more studies are needed to elucidate the method and amount of inhalation.
Clinical applications of hydrogen therapy in liver diseases
A large number of animal experiments have offered a substantive body of evidence that hydrogen therapy is a very promising treatment against liver diseases. In fact, the rational use of hydrogen has already solved a large number of clinical problems.
Oral intake of HRS for 1 month ameliorated systemic splanchnic hyperdynamic circulations and portal hypertension, decreased the circulating inflammatory cytokines, VEGF levels and mesenteric oxidative stress, decreased intrahepatic resistance and splanchnic vasodilatation, inhibited mesenteric angiogenic markers and angiogenesis, and inhibited HUVEC tube formation and migration.39 The experimental result indicated that HRS is an effective conservative method for the complications of cirrhosis.
There is also research about the effects of HRW in liver diseases in clinical studies. In patients with chronic hepatitis B (CHB), increases in xanthine oxidase (XOD) and MDA and decreases in SOD and glutathione S-transferase (GST) indicated that oxidative stress was obvious, and the liver function was also significantly impaired. The oxidative stress remained unchanged in the routine treatment group, while it was markedly improved in another treatment group in which patients received additional oral HRW (1,200–1,800 mL/day, twice daily) for 6 consecutive weeks. The HBV-DNA level and liver function has improved tendencies in the routine treatment group and the HW treatment group.40
Patients being treated with radiotherapy for liver tumours who drank HRW gained a reduced level of reactive oxygen metabolites in the blood and higher quality of life (QOL) scores than controls. However, there was no difference in tumour response to radiotherapy.14
Hydrogen treatment could significantly attenuate the severity of liver injury induced by ischaemia–reperfusion. A drop in AST and lactate dehydrogenase (LDH) levels after infusing lactated Ringer’s solution saturated with hydrogen (5 ppm) through the portal vein before reperfusion indicates that it may be applied in the clinical setting.41 The treatment group showed reduced serum ALT activity and markers of lipid peroxidation, and post-ischaemia–reperfusion histological changes were reduced. The treatment inhibited HMGB1 expression and release, reflecting a reduced local and systemic inflammatory response to hepatic ischaemia–reperfusion.36 HRS pretreatment relieved acute kidney injury after liver transplantation. It significantly ameliorated apoptosis by decreasing the apoptotic rate and inhibiting the expression of caspase 3 and cytochrome c. The expression of becline-1 and microtubule-associated protein light 3-II were upregulated, with the inhibition of p62 and lysosome-associated membrane protein-2. This indicates that hydrogen reduces apoptosis and is possibly involved in the modulation of p53-mediated autophagy.42 Researchers pointed out that HRS may have a similar regeneration-promoting effect to lactulose administration, with which excessive increases in inflammatory cytokines and a regeneration-promoting effect were observed.43 Almost all clinical researches of hydrogen were carried out as randomised and controlled studies. We propose that drinking HRW for more than 4 weeks very likely would benefit liver dysfunction or diseases such as non-alcoholic fatty liver disease (NAFLD), CHB and drug- or radiation-induced liver dysfunction. A brief overview of clinical applications of hydrogen in liver diseases is shown in Table 1.
Clinical application of hydrogen in liver diseases
Conclusion
Although research on using hydrogen in liver disease has been conducted in certain fields, in which the protective effect was associated with a reduction in both oxidative stress and inflammatory injury, there are still many areas that need exploring.
Administration methods of hydrogen therapy: Inhalation of H2 gas and administration of HRW or other solutions are tools to introduce H2 into the body; however, the former requires an adequate hospital and costly medical facilities, and preservation needs improving for the latter. Furthermore, it is not easy to supply a large amount of highly concentrated H2 into our bodies in a continuous manner using these tools in everyday situations. On the other hand, H2 production via large-bowel fermentation is a much more continuous means of supplying H2 in vivo. Also, the administration ways of hydrogen therapy may have different effects and criteria are needed to evaluate the amount of hydrogen intake for evaluating the dosage effect.41
Hydrogen therapy effect on liver diseases: In the context above, only one randomised controlled trial about the effect of HRS on patients with CHB can be powerful proof of the effect of hydrogen therapy in liver diseases. Other methods of hydrogen therapy, including inhaling hydrogen gas or drinking HRW, need further randomised trials in patients.
Although it is difficult to say whether hydrogen therapy has direct antiviral effects, it may be used to interfere with the immune inflammatory response of liver induced by viral hepatitis.
Last but not least, it is well worth developing clinical medicine research in fatty liver, autoimmune diseases and tumour chemical damage after radiotherapy in liver. Also, challenges include the need for more clinical trials and research to be carried out on the effectiveness of hydrogen therapy in liver diseases. We believe that hydrogen therapy merits further investigation of the underlying mechanisms for its potential antioxidant and anti-inflammatory effects in clinical treatment.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.