
ABSTRACT
Introduction Sepsis incidence and mortality are increasing, yet sepsis appears to be under-recognised and under-reported. Accurate recognition and coding of sepsis allows for appropriate funding and accurate epidemiological representation.
Methods We implemented a discharge summary template for all patients discharged from our infectious diseases service and analysed sepsis documentation and coding before and after its introduction.
Results Beforehand, we found that 59% of 29 patients had sepsis, yet only 10% had it documented on their discharge summary, and 17% had it coded. Following implementation of the template, 38% of 52 patients had sepsis documented, yet only 20% of these had it coded. After delivery of a training session to the coders regarding the importance of sepsis, 38% of patients with a diagnosis of sepsis had it coded.
Discussion Despite requiring ongoing education and encouragement of clinicians and coders, implementation of the template was quick, cheap and easy and improved sepsis coding.
Introduction
Sepsis incidence is increasing annually; sepsis claims almost twice as many lives as lung cancer and more lives than breast, prostate and bowel cancer combined.1,2 However, in the National Confidential Enquiry into Patient Outcome and Death (NCEPOD) Just say sepsis! report, sepsis was only documented on 40.8% of death certificates from septic patients, implying that sepsis is under-recognised and under-reported in healthcare settings.2 Diagnosing ‘sepsis’ has significant effects on patient factors, such as prognosis and management, and also on administrative factors, such as epidemiology and funding.
There are more than 1.5 million episodes of the most common sources of infection giving rise to sepsis each year, and it is highly likely that a significant number of these will have sepsis but will not be coded as such.1 Considering the significant financial burden of sepsis, it is vital that these diagnoses be correctly coded. This allows for appropriate funding, and for accurate epidemiological representation. Indeed, studies have already shown an increasing use of explicit codes for sepsis and how significantly this will impact epidemiological estimates.3
Our aim was to identify the gaps that existed in our system when it came to sepsis diagnosis and accurate coding so that we could implement simple measures to improve our service.
Methods
We conducted multiple audit cycles reviewing the notes, discharge summaries and clinical codes of patients discharged from the infectious diseases service of a busy north-west London district general hospital. We wanted to ascertain if septic patients were correctly diagnosed, then if sepsis was documented on their discharge summary and subsequently coded as such. All cases in the first audit were discharged between April and September 2018. The second audit included cases discharged between October 2018 and March 2019. The third audit involved cases discharged between April and September 2019. Data were collected and analysed from the final set of patients in January 2020.
Firstly, it was important to consider an appropriate definition for sepsis to use in our audit. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) defined sepsis as a life-threatening organ dysfunction caused by a dysregulated host response to infection.4 This definition is used across our hospital. To define organ dysfunction, they advise using a Sequential Organ Failure Assessment (SOFA) score of 2 or more; this is a complex score with multiple variables that tends only to be measured in intensive care settings. To easily identify patients likely to have poor outcomes in the emergency department or on a medical ward, they advise using the quick SOFA (qSOFA) as a rapid bedside test. This represents three variables: respiratory rate of 22 breaths/min or greater, altered mentation or systolic blood pressure of 100 mmHg or less. A qSOFA score of 2 or more with evidence of infection is an efficient and effective method for clinicians to identify patients likely to have poor outcomes. It is vital that simple diagnostic criteria are established and disseminated among staff to ensure accurate recognition and reporting of sepsis. In this audit, in cases where sepsis was not documented in the notes, we used evidence of infection and a qSOFA of two or more as a trigger for reviewing whether organ dysfunction, and therefore sepsis, was most probably present during admission.
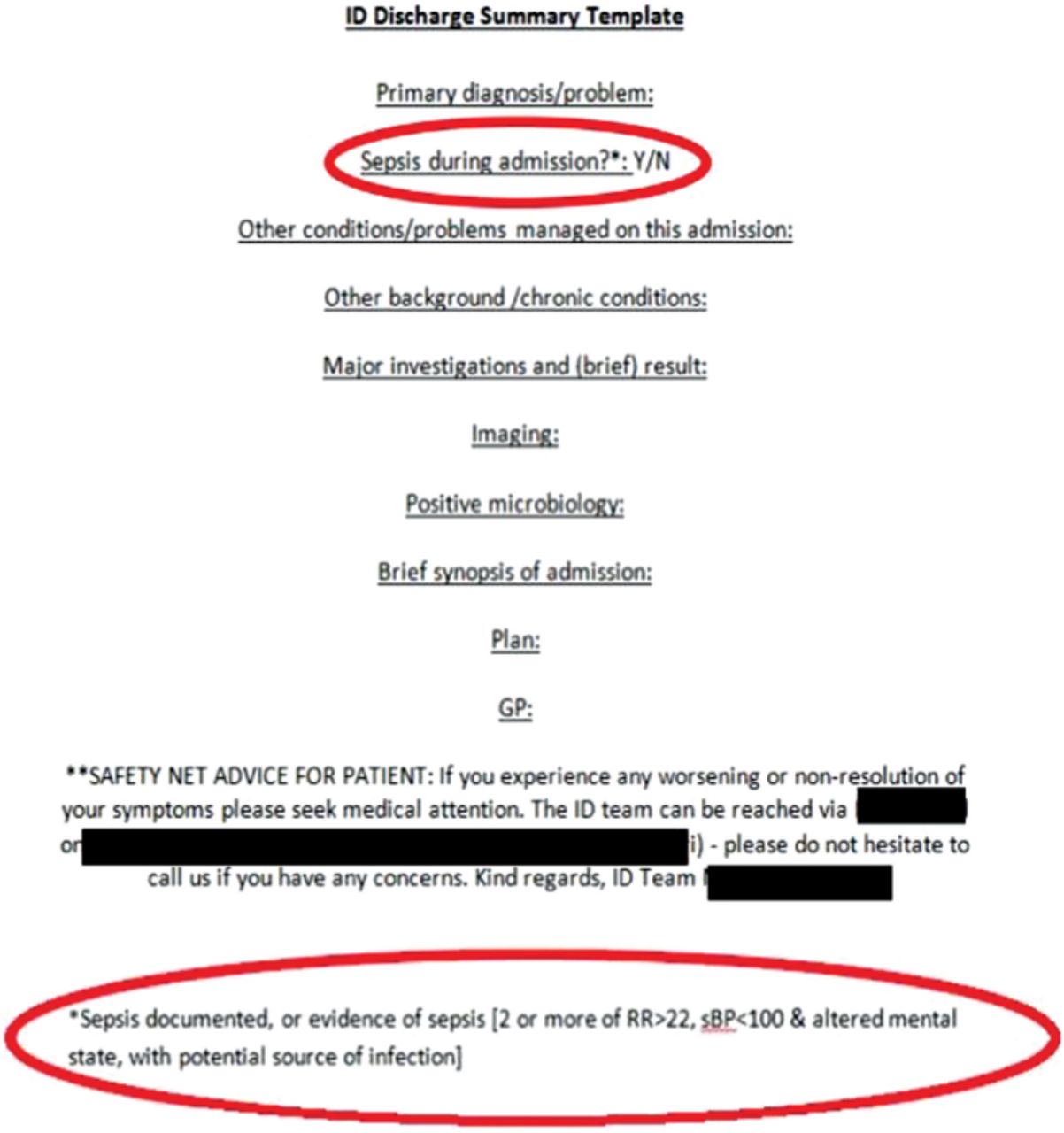
In order to improve sepsis diagnosis and coding, we decided to introduce a simple discharge summary template (Fig 1) for all patients discharged from the infectious diseases service, which included a specific question about whether sepsis had been documented during admission, along with a trigger for considering a diagnosis of sepsis if not already documented in the notes. Such a template would act as a prompt to clinicians to re-review whether their patient had sepsis during admission and provide coders with an immediate visual cue to aid in sepsis coding. The concept of the discharge summary template was introduced to all junior doctors during their induction prior to starting their infectious disease rotation and its implementation was encouraged for all discharged patients by senior members of the team.

The discharge summary template implemented to increase sepsis documentation and coding. Red circled areas indicate the newly introduced areas to indicate sepsis in the patient.
Coding in the trust is carried out by qualified clinical coders who use the National Clinical Coding Standards ICD-10 to enable them to code patient episodes.5 This is done by a review of the discharge summary and of the patient notes by the coding team, who then allocate multiple codes based on the information found in the notes. Any time a coder used a code pertaining to sepsis, we counted that as a case coded as sepsis. Coders are not clinicians so cannot make judgements on which patients with infections had sepsis and which did not. Therefore, they rely on clinicians to document clearly in the notes whether a particular infection has caused sepsis.
In our first audit cycle, we calculated how many of a random selection of discharged patients had sepsis during admission based on review of their clinical notes, and then how many of those had it documented on their discharge summaries and subsequently coded. In all subsequent cycles, we calculated how many patients had sepsis documented on their discharge summaries, and then how many subsequently received a clinical code relating to sepsis.
Results
The first cycle of our audit analysed a cohort of 29 discharged patients. A review of the notes revealed that 17 (59%) had evidence of sepsis at some point during admission and 15 (52%) had sepsis documented somewhere in their notes. However, sepsis was only documented on the discharge summaries of three (10%) of these patients, and only coded in five (17%) of these patients.
Six months after implementation of our discharge summary template, we reviewed the discharge summaries of 52 patients who had been discharged from the infectious diseases service. We found that 20 patients (38%) had a diagnosis of sepsis documented on their discharge summary, which is a massive increase compared with the 10% previously. Of these patients who had sepsis documented on their discharge summary, only four (20%) were given a clinical code relating to sepsis. Furthermore, one patient in this cohort was coded with sepsis but this was not documented on the discharge summary. On a subsequent review of this patient's notes, a diagnosis of sepsis was evident and sepsis documented throughout the notes, yet not on the discharge summary.
To further improve sepsis coding and encourage our coders to utilise our discharge summary template, we organised a brief training session with the coders. The training consisted of a single session lasting no more than 1 hour. The coding team were briefed on the importance of sepsis documentation and coding with regard to its implications for funding and epidemiological representation and we highlighted that the new discharge summary template now stated whether sepsis was evident during admission. Six months after the training session, we reviewed the discharge summaries of 146 patients discharged from the infectious diseases service. Of the 32 patients with a qSOFA score of 2 or more, 26 had evidence of sepsis when SOFA scores were calculated. Among these patients with sepsis, 38% (10/26) had a clinical code relating to sepsis, which is a significant increase compared with the 17% noted in our initial audit and 20% in our second audit.
Discussion
The initial results in our analysis demonstrate a significant gap in reporting of sepsis. It isn't clear whether this is due to a lack in recognition of patients with sepsis, or rather a reluctance to document sepsis itself in discharge summaries. Coders may carry out an extensive review of patient notes but, even then, less than one in three patients with ‘sepsis’ documented somewhere in the notes were actually given a clinical code related to sepsis. We must remember that coders are not clinicians, so they require very clear documentation to accurately assign clinical codes.
We hoped our discharge summary template would help to tackle each of the problems above. Firstly, it provides clinicians with an aide-memoir to enable them to consider a diagnosis of sepsis, and then encourages them to document any incidence of sepsis during the hospital admission. With a straight-forward question about sepsis documented on the discharge summary, coders can easily assign a clinical code relating to sepsis without an extensive review of patient notes to look for it.
The results after implementation of our discharge summary template demonstrate that the template encouraged doctors to think about and diagnose sepsis more than before, yet it was not being utilised by the coders. Given that there was one case where sepsis was not documented on the discharge summary despite a diagnosis of sepsis being present, we can deduce that clinicians are still not documenting all episodes of sepsis on the discharge summary. From this case, we also note that the coders were still extensively reviewing patient notes and not effectively utilising our discharge summary template for sepsis coding.
After delivering a training session to the coders, our audit results demonstrate that coding of sepsis has significantly improved. It is important to note that slightly fewer patients had a diagnosis of sepsis on their discharge summaries in this audit cycle, but it is reassuring that the coders are utilising the discharge summary template to enable better coding of sepsis compared to previous.
Similar studies in the literature have demonstrated how poorly sepsis is coded in administrative data. One study has shown that sepsis coding is significantly improved by optimising the ICD codes used by clinical coders, thereby increasing the sensitivity of such codes at the expense of slightly reducing the specificity.6 Other studies examining the validity of discharge codes for sepsis have shown various results depending on the diagnosis of interest; there was good agreement between sepsis coding and Gram-negative bacteraemia in one study but poor accuracy of sepsis coding in Staphylococcus aureus bacteraemia in another study.7,8 A study from Italy found that less than 50% of patients with positive blood cultures had a discharge diagnosis code of sepsis.9
It is important to remember that sepsis can occur without positive blood cultures and that a bacteraemia does not always cause sepsis, so the results above must be taken with caution. Our quality improvement project tried to encourage clinicians to consider the diagnosis of sepsis in patients with infection regardless of blood culture results.
It is clear that there is still work to be done regarding sepsis coding and finding the most appropriate definition of sepsis for use in this context.
Limitations
During this quality improvement project, we noticed some limitations regarding the internal validity of the work, as well as its generalisability.
One major drawback in both of the subsequent audit cycles is that we did not review the notes of each patient on these occasions, therefore, we could not determine exactly how many patients actually had sepsis. Instead, we relied on the clinicians who were writing the discharge summary to identify and document cases of sepsis. However, for those patients with a documented qSOFA score of 2 or more, we did calculate SOFA scores to determine presence of sepsis. As previously explained, while our discharge template has encouraged clinicians to more thoroughly review patient notes prior to documenting sepsis on the discharge summary, there is still some room for improvement from this perspective. We show that qSOFA leads to an overestimate of sepsis cases. Sepsis-3 encourages the use of qSOFA to screen patients initially, but then advises the use of the SOFA score to actually identify organ dysfunction and define sepsis.4 In subsequent analysis of a database of more than 74,000 patients, 75% of patients with a qSOFA score of 2 or more also had a SOFA score of 2 or more, therefore fulfilling the criteria for sepsis diagnosis.10 The qSOFA score on its own clearly identifies some patients who do not have sepsis, and fails to identify other patients that do.11 Though having a tick box for sepsis on the discharge summary increases awareness and documentation, we acknowledge that adhering to the Sepsis-3 definition is important to improve accuracy of sepsis epidemiology and coding. Going forward, we plan to further modify our discharge summary template to make it clearer that qSOFA score is simply a tool to raise suspicion for a diagnosis of sepsis, by changing the word ‘evidence’ to ‘suspicion’.
In terms of the generalisability of this template, while it is cheap and easy for trusts to implement, it does require continual training and encouragement of the doctors who will be using it and of the coders who will be reviewing it. The rate of sepsis in the infectious diseases service is probably greater than that on other wards, so doctors may not easily find the relevance in using such a template in an area that manages fewer cases of sepsis and, thus, actual sepsis diagnosis may be less accurate.
Conclusion
Implementation of the discharge summary template was quick, cheap and straight-forward. Its use requires continued training and encouragement of staff, as well as increased education and awareness of the coders. However, these are all simple measures for the accurate diagnosis and documentation of sepsis cases. This will result in appropriate allocation of funding for septic patients, and provide accurate epidemiological data for ongoing research into sepsis. We suggest that this simple approach should be implemented by all acute trusts to provide a more accurate and current picture of the sepsis battle we are fighting.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.