
ABSTRACT
Varicella zoster reactivation is a known risk following stem-cell transplantation, but has become more infrequent since universal antiviral prophylaxis. We report an unusual case of late, disseminated reactivation in a 27-year-old man with positive pre-transplant serology, and discuss implications for post-transplant prophylaxis and immune monitoring.
Case presentation
A 27-year-old man presented with diffuse abdominal pain, nausea and constipation. Abdominal imaging revealed oedematous pancreatitis and non-obstructive cholecystitis. Eight months earlier, he had undergone myeloablative, haplo-identical, allogeneic stem cell transplantation (SCT) for treatment of acute lymphoblastic leukaemia (ALL). Post-transplant immunosuppression had been stopped 4 months prior to admission and his regular medication comprised ranitidine (150 mg once daily (od)), and prophylactic aciclovir (400 mg twice daily (bd)), co-trimoxazole (960 mg three times a week) and phenoxymethylpenicillin (250 mg bd).
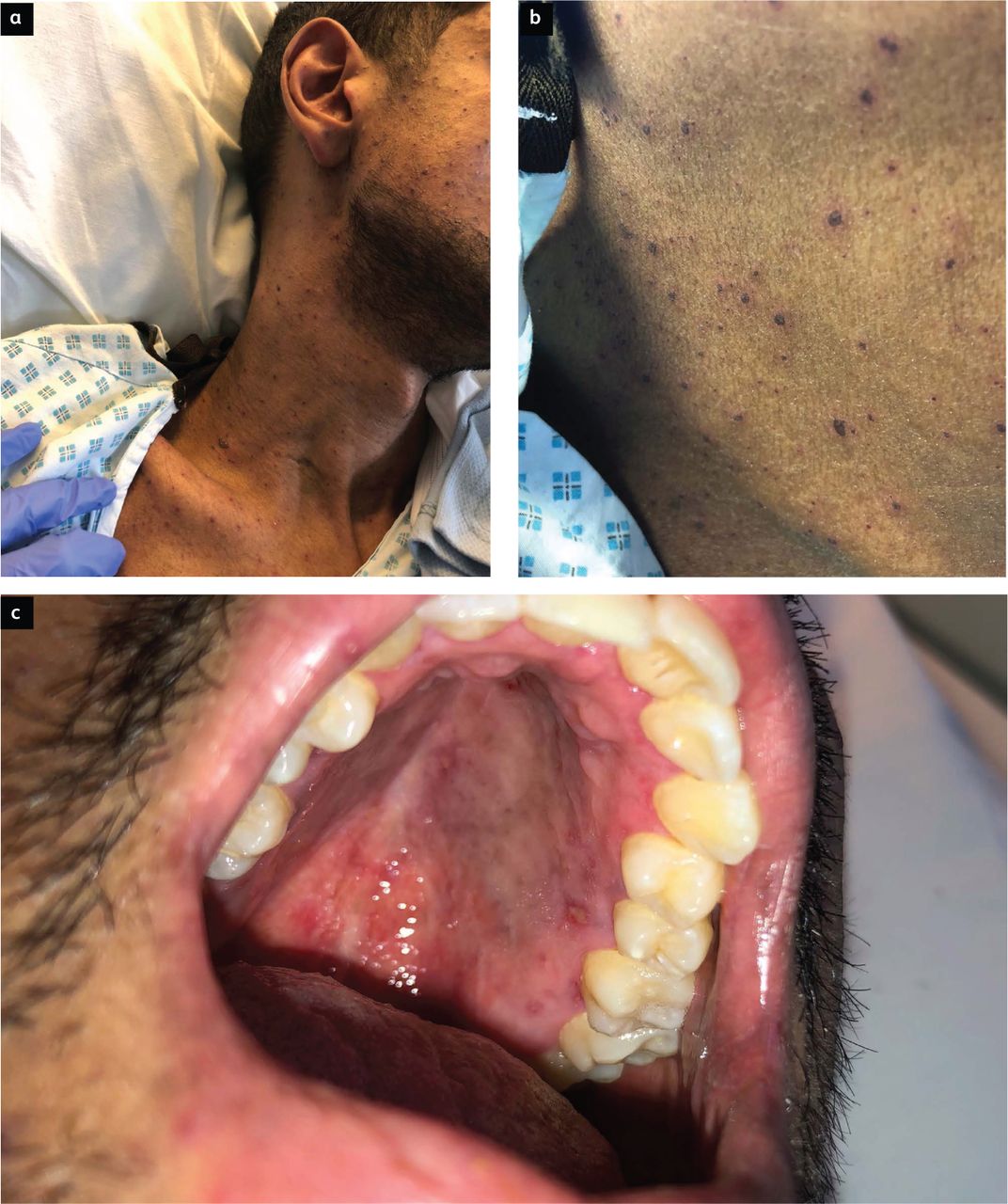
Intravenous (IV) fluids and antibiotics (co-amoxiclav and gentamicin) were commenced. Two days into his admission, a painless, non-pruritic, vesicular rash emerged, which spread from his face to involve his trunk, arms, thighs and hard palate (Fig 1). He also developed profuse diarrhoea. On examination, he was febrile (39.6°C) and appeared unwell. His pulse rate was 102 beats/min and blood pressure was 102/64 mmHg. Heart sounds were normal, and his chest was clear on auscultation. His abdomen was soft with generalised tenderness and active bowel sounds. There were no focal neurological signs and examination of the eyes was unremarkable. There was a diffuse rash affecting his face, trunk and limbs but sparing palmar and plantar surfaces; lesions were dark, haemorrhagic vesicles of 1–4 mm diameter over an erythematous base (Figs 1a and b). Pigmented lesions were also noted over the hard palate, with some ulceration (Fig 1c).
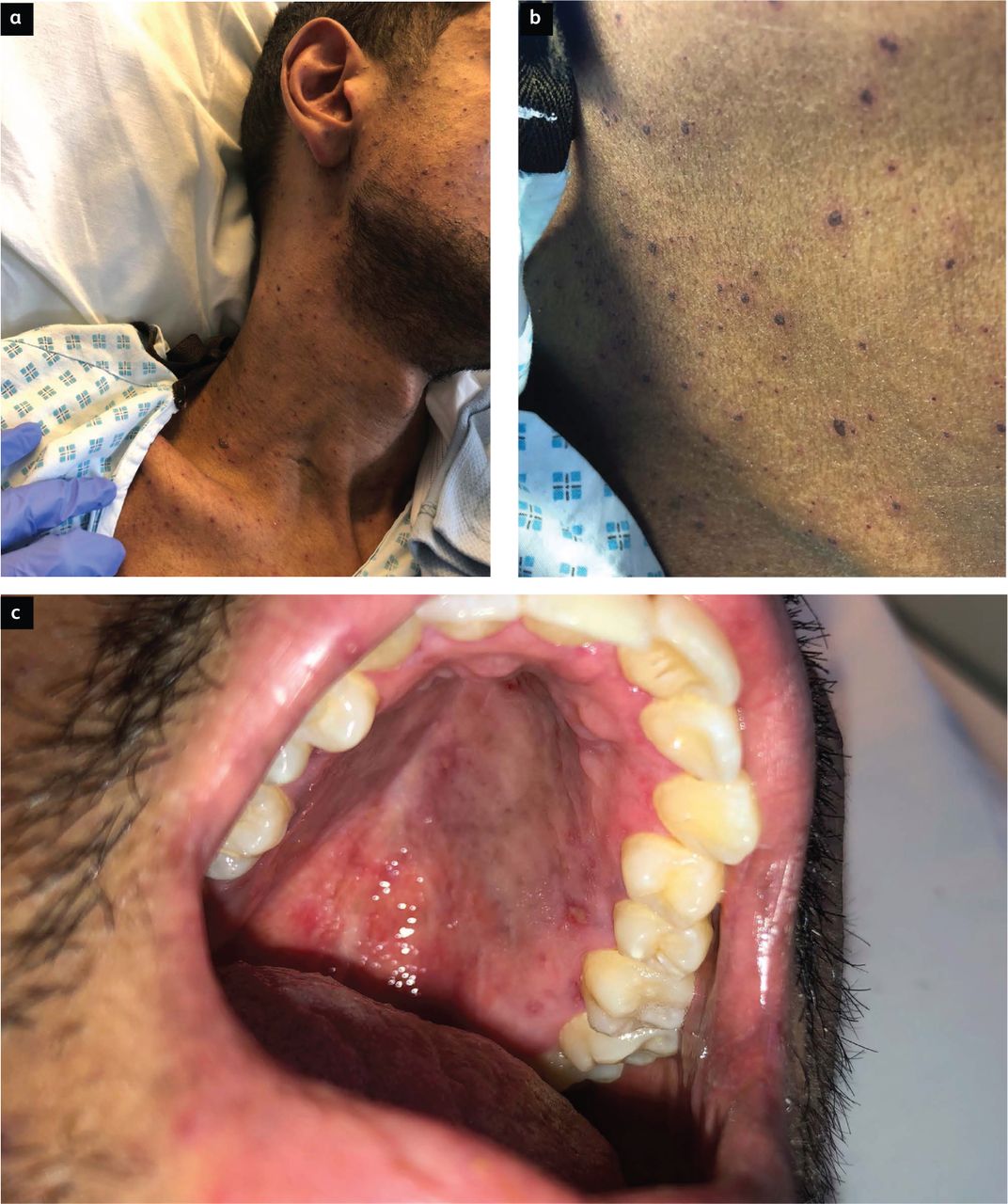
A diffuse painless, non-pruritic, vesicular rash consisting of dark 1–4 mm haemorrhagic vesicles. a) Rash across the face, neck and chest. b) Close-up image of the vesicles. c) Pigmented, ulcerated lesions on the hard palate.
Admission blood tests are shown in supplementary material S1. These were remarkable for hyponatraemia (sodium of 125 mmol/L), hypocalcaemia (adjusted calcium of 2.11 mmol/L) and marked transaminitis. C-reactive protein (CRP) and lipase were mildly elevated at 42 mg/L (<4 mg/L) and 98 U/L (<60 U/L), respectively.
With concerns that his presentation may have been due to graft versus host disease (GvHD), IV methylprednisolone was commenced at 1 mg/kg od. Co-amoxiclav was changed to piperacillin-tazobactam to cover the possibility of gut translocation in the setting of acute gastrointestinal GvHD and in case the skin lesions were ecthyma gangrenosum. He was also started on IV aciclovir 10 mg/kg three times daily (tds) in case the skin lesions were due to herpes simplex virus (HSV) or varicella zoster virus (VZV). Given that the patient had previously been a resident in the tropics, he was also given a dose of ivermectin in case this presentation was due to disseminated infection with Strongyloides stercoralis. Swabs of skin and palatal lesions were sent for viral polymerase chain reaction (PCR) and bacterial culture and an extensive infection screen was completed, including enterovirus, adenovirus, herpes PCR and biopsy of one of the skin lesions (supplementary material S2).
Investigations confirmed disseminated VZV infection, with identification of VZV viraemia and positive VZV PCR from skin and palatal lesion swabs. The abdominal symptoms and skin rash improved after several days of aciclovir treatment, and methylprednisolone was weaned. Antimicrobials were de-escalated after 7 days and prophylactic co-trimoxazole and phenoxymethylpenicillin recommenced. He was discharged on the 14th day after admission.
The patient had had no unwell contacts and no contact with children before admission. He did not recall a history of chickenpox but had positive VZV serology both pre- and post-transplant, with titres of 3,320 and 182 mIU/mL, respectively, at levels deemed to represent adequate humoral immunity. Further immunological investigation revealed a CD4+ lymphopenia, with an absolute CD4+ count of 56 × 106/L (normal range 455–1,320; supplementary material S3).
Discussion
VZV reactivation is a significant risk following haematopoietic (H)SCT.1 Rates of 20–45% during the first year post-transplant were reported in the absence of antiviral prophylaxis, depending upon transplant conditioning and the presence or absence of GvHD.2–4 The majority of reactivation occurs within 9–12 months, although cases of herpes zoster (HZ) have been reported as late as 3 years post-transplant.3,5 Antiviral prophylaxis with aciclovir is now universal post-transplant and has reduced first-year reactivation rates to 2–5%. VZV reactivation typically presents as dermatomal HZ, but less commonly manifests as disseminated infection with widespread cutaneous, mucocutaneous and, at times, visceral involvement.
Visceral involvement in disseminated VZV has been reported but is a challenge to diagnose. Acute severe abdominal pain may be the presenting feature of visceral infection.6 Abdominal symptoms (most commonly epigastric pain, nausea, vomiting, diarrhoea, and elevated hepatic and pancreatic enzymes) can precede skin eruptions by several days and may also occur in the absence of cutaneous disease.7,8 Neurological and respiratory manifestations of disseminated zoster are also important to identify, the latter accounting for most fatal cases of disseminated disease.9
Clinical diagnosis of disseminated zoster post-transplant can be challenging, as immune suppressed patients are more likely to present with atypical mucocutaneous or visceral disease that may mimic other infections, drug reactions or GvHD.10 As for our patient, laboratory testing is becoming the standard for confirmation in such cases. Although VZV was not definitively confirmed as the cause of abdominal symptoms in the case we present, it is likely that, in the context of severe disseminated viral reactivation and without alternative explanation, these symptoms represented visceral VZV infection.
Primary VZV infection induces both humoral and cellular immune responses.11 Cell-mediated immunity is more important than humoral in preventing viral reactivation.12 This is reflected in the increase in rate of HZ with advancing age in the immunocompetent population, as although antibody titres remain relatively stable over time, virus-specific cell-mediated immunity wanes.13 Specifically, a VZV-specific T-cell response is required to prevent symptomatic reactivation of endogenous virus, as well as infection after exogenous re-exposure.11,13 There is growing evidence for a predominant CD4+ T-cell response in VZV infection, and a proven role of CD4+ cells in suppressing viral replication.14 However, as yet, there is no reliable way to measure VZV-specific cell-mediated immunity and so the presence of humoral immunity in the form of an anti-VZV antibody titre is used as a surrogate. This case highlights that serum VZV immunoglobulin (Ig) G is not an entirely reliable indicator of protection against reactivation, and that the presence of VZV IgG should not dissuade clinicians from considering the diagnosis of VZV reactivation.
Antiviral prophylaxis with aciclovir is now universal post-transplant and has been demonstrated to significantly reduce VZV reactivation risk.15 However, as highlighted in this case, severe infection due to cutaneous and disseminated reactivation may still occur despite prophylaxis.1 The reasons for this are unclear, and may include lack of adherence, impaired absorption and evolution of antiviral resistance. Most cases of VZV reactivation occur following discontinuation of antiviral prophylaxis, with reactivation rates of 31–33% reported within 3 months of discontinuation.4,16 In the absence of a test to measure VZV-specific cell-mediated immunity, adopting an approach based on CD4+ cell count recovery may offer a more nuanced and biologically relevant approach than the current time-based strategy for discontinuing aciclovir prophylaxis. T-cell immune reconstitution may be expected around 3–4 months following allogeneic SCT, with CD4+ cells known to reconstitute later than CD8+.17 However, this is highly variable, as demonstrated in our patient in whom reconstitution was incomplete at 8 months post-transplant. This raises the questions of whether lymphocyte subsets should be measured routinely, and if the duration of antiviral prophylaxis should be extended until complete reconstitution, with CD4+ count consistently greater than 200 × 106/L is confirmed.4,18
Key points
Severe, disseminated VZV reactivation is possible in the context of post-transplant immunocompromise, even with positive serology, ongoing antiviral prophylaxis and following the cessation of immunosuppressive therapy.
High clinical suspicion is necessary for diagnosis of disseminated infection in such cases, both in the presence and absence of a characteristic skin eruption; with PCR of vesicle fluid and/or blood samples being the key diagnostic test.
Abdominal symptoms may be the first and, sometimes, only clinical feature of disseminated VZV infection, and visceral VZV reactivation should be on the differential diagnosis list for any patient post-transplant with abdominal pain and/or a transaminitis; with a PCR on ethylenediaminetetraacetic acid (EDTA) blood being the key diagnostic test.
Lymphocyte subsets should be measured in transplant patients presenting with possible unusual infections, as the degree of immune compromise will influence the range of potential pathogens and should influence the use of antimicrobial prophylaxis.
There may be an argument for extending aciclovir prophylaxis in patients with positive pre-transplant serology until they have a CD4+ cell count consistently greater than 200 × 106/L. Tests of pathogen-specific cell-mediated immunity are now available for cytomegalovirus, and a similar assay for VZV would be helpful.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Haematology and biochemistry results on admission.
S1 – Summary of infection investigation results.
S1 – Summary of immunological investigations.
Acknowledgements
The authors would like to thank the patient for allowing us to publish this case report.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.