
ABSTRACT
Inpatient hyperglycaemia is associated with poor patient outcomes. The majority of inpatients with diabetes are admitted with non-diabetes-related conditions and are primarily cared for by a clinician who does not specialise in diabetes. We describe common inpatient hyperglycaemia scenarios and outline strategic management approaches for the general physician, enabling better frontline care for people with diabetes.
Key points
Patients with insulin-treated diabetes should be supported to continue to self-manage their diabetes in hospital if they are able to and it is deemed safe for them to do so.
Do not omit basal insulin in patients with type 1 diabetes.
When managing hyperglycaemia related to steroids it is important to consider the duration of action of the prescribed steroid when deciding which treatment to initiate.
Diabetic ketoacidosis and hyperosmolar hyperglycaemic state should be considered and excluded in hyperglycaemic inpatients or those on sodium-glucose cotransporter-2 inhibitors.
Patients receiving nasogastric feeding who are hyperglycaemic despite metformin therapy should be considered for subcutaneous insulin therapy as nasogastric absorption of other oral hypoglycaemic agents is not reliable.
Introduction
The global incidence of diabetes continues to rise with an estimated one in six inpatients having diabetes.1,2 Inpatient hyperglycaemia is associated with poor patient outcomes; the majority of inpatients with diabetes are admitted with non-diabetes-related conditions and are primarily cared for by a clinician who does not specialise in diabetes.3,4 Fluctuating glycaemic control is typically seen in acutely unwell patients. While most people with type 1 diabetes (T1D) are trained in self-adjusting insulin doses in response to hyperglycaemia, their ability to make these changes in hospital may be affected by multiple factors including access to insulin and their ability to reliably titrate insulin when unwell. Furthermore, treatment of acute illnesses in people with diabetes (for example, steroid therapy or alternative feeding) can lead to a deterioration in glucose control and may mandate changes to their diabetes treatment regimen. The National Diabetes Inpatient Audit (NaDIA) raised concerns about the frequency of hospital-acquired diabetic ketoacidosis (DKA) and hyperosmolar hyperglycaemic state (HHS) cases, highlighting the need for improved inpatient hyperglycaemia management.2
This article outlines therapeutic options for non-critical care adult inpatient management of hyperglycaemia in people with T1D on multiple dose injections (MDI) or with type 2 diabetes (T2D), patients on steroids and patients requiring alternative feeding.
Management of inpatient hyperglycaemia in T1D
All inpatients with T1D should have capillary blood glucose (CBG) levels checked at least four times daily (pre-meals and at bedtime). A CBG ≥12 mmol/L is considered hyperglycaemia and in the context of acute illness ketones should be checked. If capillary ketones are ≥1.5 mmol/L, DKA must be excluded. If the patient fulfils the diagnostic criteria for DKA (CBG >11.1 mmol/L; plasma ketones ≥3 mmol/L; pH <7.3 or bicarbonate <15 mmol/L), local DKA management protocols should be followed urgently.5 If the patient is not in DKA, a variable rate insulin infusion (VRII) can be started to ensure rapid clearance of ketosis and reduce the risk of a hyperglycaemic emergency. Long-acting insulin should be continued even if the patient is unable to maintain oral intake.
Many people with T1D are able to self-manage their condition and should be supported to continue doing so as an inpatient should they be safe to do so. When unwell, they may follow ‘dose adjustments for normal eating’ (DAFNE) sick day rules, which enables them to adjust their insulin dosage in response to hyperglycaemia or ketonaemia.6
Provided the patient has capillary ketones <1.5 mmol/L and is well enough, they can follow DAFNE principles to calculate and administer extra rapid-acting insulin (a ‘correction dose’) targeting CBGs of 6–10 mmol/L.5 This should be given with the patient's usual pre-meal insulin dose if they are eating or given without the mealtime insulin dose if they are not eating but are hyperglycaemic. A minimum of 2-hourly CBG and ketone monitoring is required with a low threshold to switch to VRII if ketonaemia persists, the patient is unable to maintain adequate hydration or they are vomiting or are unwell.
If the patient is unfamiliar with DAFNE principles or unable to self-manage, give 2–6 units of NovoRapid if the CBG is >18 mmol/L (accepting that 1 unit of NovoRapid will lower CBGs by 3 mmol/L).5,7 Repeat this after 4 hours if readings >18 mmol/L persist. If there is no improvement, then a VRII should be considered.
Management of inpatient hyperglycaemia in T2D
People with insulin-treated T2D who are hyperglycaemic should have their doses, regimen and glycated haemoglobin (HbA1c) reviewed during admission. It is important to exclude DKA and HHS (serum osmolality ≥320 mosmol/kg, blood glucose typically ≥30 mmol/L).8
Outside of a hyperglycaemic emergency, CBGs in people with T2D between 11.1–22 mmol/L will usually require 2–4 units of rapid-acting insulin as a correction dose.9 Two-hourly CBG monitoring is required following the correction dose; a further dose of rapid-acting insulin should not be given within 4 hours. Further treatment escalation should be discussed with the local diabetes team.
The patient's renal function should be taken into account when starting or administering additional doses of subcutaneous (SC) insulin. Poor renal function impairs insulin clearance and can lead to a prolonged insulin effect, necessitating lower insulin doses to prevent iatrogenic hypoglycaemia.10
Sodium-glucose cotransporter-2 inhibitors (SGLT-2i) should be temporarily discontinued during acute illnesses due to the risk of (euglycaemic) ketoacidosis. Patients on oral hypoglycaemic agents (OHAs) may require insulin depending on the degree of hyperglycaemia.3 The chosen insulin regimen should take into account patient characteristics, hypoglycaemia risk and local protocols and involve the specialist diabetes team. Patients newly initiated on SC insulin should have the long-term suitability of this reviewed pre-discharge. Additionally, they should receive a glucometer and appropriate education by a diabetes specialist nurse.
Fig 1 summarises the approach to assessing and managing an inpatient with hyperglycaemia.

The approach to assessing and managing hyperglycaemia in an adult inpatient with diabetes. aCorrection dose of insulin to be given as per DAFNE principles; if the patient is unable to follow DAFNE principles, then give 2–6 units of NovoRapid (accepting 1 unit will lower CBG by 3 mmol/L); repeat dose to be given after 4 hours if hyperglycaemia/ketonaemia persists. bDKA criteria: pH <7.3 and/or HCO3 <15 mmol/L, ketones ≥3 mmol/L and glucose >11.1 mmol/L. cHHS criteria: serum osmolality ≥320 mosmol/kg, CBG typically ≥30 mmol/L and hypovolaemia. CBG = capillary blood glucose; DKA = diabetic ketoacidosis; HHS = hyperosmolar hyperglycaemic state; T1D = type 1 diabetes; T2D = type 2 diabetes; VBG = venous blood gas; VRII = variable rate insulin infusion.
Scenarios 1 and 2 are worked clinical examples illustrating how clinicians may approach inpatients with T2D (Box 1) and T1D (Box 2) presenting with hyperglycaemia.
Scenario 1
Scenario 2
Management of hyperglycaemia in patients commenced on steroids
Management of steroid-exacerbated or -induced hyperglycaemia is affected by the duration of action of the prescribed steroid; for example, the hyperglycaemic effect of once-morning (OM) prednisolone (>5 mg) will typically last until the end of the day with a fall in CBGs by the following morning, while longer-acting steroids like dexamethasone may result in persisting hyperglycaemic effects throughout the 24-hour period (Table 1).11 Patients with pre-existing diabetes should have CBGs monitored pre-meals and at bedtime, while patients without diabetes should have CBGs checked at least once daily (pre-lunch or dinner), increased to four times daily if hyperglycaemia (glucose >12 mmol/L) is detected.12 Early input from the local diabetes team is recommended in these patients.
Commonly prescribed steroids, time taken for hyperglycaemic effects to resolve and most suitable insulin to manage hyperglycaemia11
Prednisolone-exacerbated hyperglycaemia in patients on MDI regimens should be managed by increasing the morning intermediate-acting (eg Humulin I or Insulatard) insulin by 10%–20% every 48–72 hours to achieve acceptable glucose readings with CBG monitoring before bed and at 2am. In patients not prescribed intermediate-acting insulin in the morning, the lunch- and dinner-time rapid-acting insulin doses should be increased by 10%–20%. Evening basal insulin doses should not routinely be increased due to the risk of nocturnal and early morning hypoglycaemia.
Patients on twice-daily mixed insulin prescriptions (eg Humulin M3, NovoMix 30 or Humalog Mix50) should increase the morning insulin dose in 10%–20% increments every 48–72 hours until target CBGs are achieved.
In patients managed with diet or OHAs, a course of a short-acting sulphonylurea (SU) such as gliclazide alongside prednisolone could be prescribed to combat the daytime hyperglycaemia caused. A starting dose of 40 mg (immediate release) OM increased in 40 mg intervals to a maximum dose of 240 mg OM is recommended.12 If hyperglycaemia remains problematic on this regimen or SUs are not suitable, then an OM intermediate-acting insulin is an alternative at a starting dose of 10 units. Input from the diabetes team or a VRII may be required depending upon the degree of hyperglycaemia.
Owing to the COVID pandemic, the use of dexamethasone has increased. For patients on dexamethasone, once daily long-acting or twice daily intermediate-acting insulin (started at 0.1–0.2 units/kg) may be more appropriate.13–15 The same approach can be used for patients on multiple daily steroid doses if hyperglycaemia is evident throughout the day and night.
The diabetes team should be informed prior to cessation of steroid therapy, in order to formulate a plan for appropriate adjustment of the patient's diabetic medication.
Management of hyperglycaemia in patients on alternative (enteral or parenteral) feeding
Alternative feeding is required in many hospitalised patients. Consensus guidelines for the management of diabetes in these circumstances is lacking. Given the range of feed regimens, all patients with diabetes on alternative feeding should be managed with input from the specialist diabetes team.
The Joint British Diabetes Societies (JBDS) have produced guidelines on the management of hyperglycaemia during enteral feeding in stroke patients, and many of these principles can be extrapolated to patients requiring enteral feeding for other conditions and those parenterally fed.16
Patients on continuous enteral or parenteral feeding should have CBGs checked at least every 4–6 hours. Targeting CBGs of 6–12 mmol/L may be more appropriate in these patients given the risk of hypoglycaemia.16
In the absence of contraindications, patients with T2D can receive metformin, in liquid or powder form, via a nasogastric (NG) tube. The NG absorption of other OHAs is unreliable. If suboptimal glycaemic control persists despite metformin, or the patient was already established on insulin or is on parenteral nutrition, insulin at the start of the feed will be required. The choice of insulin should be discussed with the specialist diabetes team and could include short-, rapid-, mixed, intermediate- or long-acting preparations depending on the feed duration.3,16,17
Patients with T1D requiring alternative feeding must continue their long-acting insulin.18 Depending on the type of feed (continuous vs bolus), they are likely to require additional doses of rapid-acting insulin at the start of the feed and at set intervals thereafter.16,18 If the feed is withheld, it is safest to commence a VRII with dextrose alongside long-acting insulin.16
Once established on SC insulin regimens, doses should be adjusted (by 10%–20% every 48 hours) to achieve CBG targets.
The medical and dietetics team must liaise closely, as any changes to the feed (composition or duration) will impact the insulin prescription. Furthermore, patients on alternative feeding are at risk of hypoglycaemia during rest periods necessitating closer CBG monitoring during this time. If the feed is interrupted after administering SC insulin there is increased risk of hypoglycaemia; therefore, CBG monitoring should increase to 1 hourly ± intravenous 10% dextrose commenced.3,16
Fig 2 summarises the approach to assessing and managing an inpatient commencing alternative feeding.16
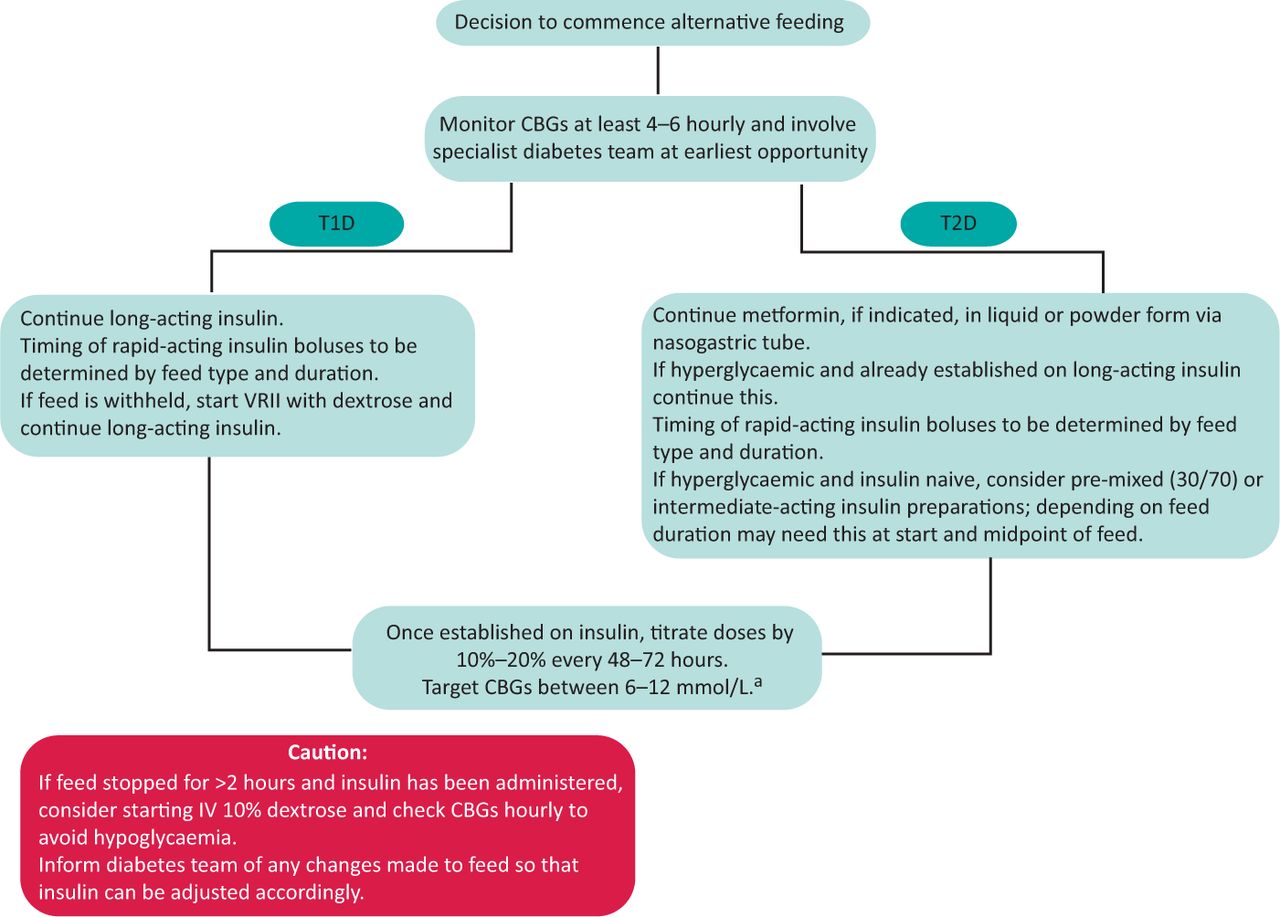
The approach to assessing and managing an adult inpatient with diabetes commencing alternative feeding.16 aTarget capillary blood glucose should be individualised. CBG = capillary blood glucose; T1D = type 1 diabetes; T2D = type 2 diabetes; VRII = variable rate insulin infusion.
Conclusion
Hyperglycaemia in adult inpatients is common and may be due to a number of factors including acute illness and prescribed interventions. Optimising glycaemic control in the hospital setting is required to improve patient outcomes and reduce the risk of preventable hyperglycaemic emergencies. While glucose readings of 6–10 mmol/L are acceptable for most inpatients, this should be individualised as some (eg frail elderly patients, those at risk of falls or patients at the end of life) may not require such tight control.12 Given the rising incidence of diabetes, general medical physicians should be aware of the common causes of inpatient hyperglycaemia and how to safely manage this in the acute setting pending specialist diabetes team input.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.