
ABSTRACT
Objective To review advance care planning (ACP) practice during the COVID-19 pandemic, evaluating the number of plans created, patient participation, cardiopulmonary resuscitation recommendations and variation between different population groups.
Design A retrospective analysis and comparison of routinely collected data from electronic recommended summary plan for emergency care and treatment (ReSPECT) records documented in April 2020 and January to December 2019.
Setting/participants Electronic ReSPECT documents completed for adult patients at a large, acute hospital trust in the UK.
Results The number of plans created per 1,000 admissions in April 2020 was 333.0% higher than in 2019. A greater proportion of plans created during April 2020 were discussed with the patient and the proportion containing a ‘for cardiopulmonary resuscitation’ recommendation was higher across all population groups. A greater proportion of plans were created for younger adults and Black and minority ethnic groups during the pandemic.
Conclusion Increased ACP during a crisis can be achieved alongside increased patient participation in decision making. A tool such as ReSPECT that supports recommendations for, as well as limitations on, treatment may have enabled the expansion of ACP observed.
Introduction
People with serious illnesses are at risk of worse outcomes following COVID-19 infection and may not benefit from all possible treatments. Advance care planning (ACP), the agreement of treatment recommendations ahead of clinical deterioration, is therefore a key part of the pandemic response.1,2 This process involves a holistic person-centred approach in which individualised care preferences and treatment recommendations are discussed ahead of potential clinical deterioration. ACP increases the likelihood that interventions are concordant with individual preferences and of clinical benefit.3,4 When facilitated with compassion, adopting an individualised approach, ACP empowers patients and improves experience of care.5 However, concern has been expressed about ‘blanket’ treatment limitation, such as ‘do not attempt cardiopulmonary resuscitation’ (DNACPR) recommendations, that target specific and have been made without consultation or ignore the individual's circumstances, views and preferences.6
To evaluate ACP at the onset of the pandemic, as part of quality assurance and improvement processes, investigators in a large acute hospital trust retrospectively analysed routinely collected data from recommended summary plan for emergency care and treatment (ReSPECT) plans for adult patients (16 years and over). ReSPECT is an ACP initiative in the UK that includes a standardised form for the documentation of treatment recommendations irrespective of diagnosis and prognosis.7 ReSPECT was implemented digitally within the trust's electronic record in 2018. We compared ReSPECT forms completed or initiated during the month of April 2020 with the previous year (1 January to 31 December 2019).
At the onset of the pandemic, in the setting of a potentially fatal illness, clinicians were encouraged at both national and local level to consider timely, patient-centred discussions addressing advance care planning. This was of particular importance in patients at risk of significant clinical deterioration, including the elderly and those living with severe frailty or underlying health conditions such as hypertension, diabetes, cardiovascular disease or chronic lung disease. The outcomes of ACP discussions were documented in ReSPECT plans within patients’ electronic health records.
Methods
Data were collected and analysed on 18 June 2020 using a Microsoft Analysis Services reporting tool that collates selected data from both digital ReSPECT plans and the hospital patient administrative system. Only plans initiated or amended during the specified periods were analysed. Those created before the periods, but not amended during them, were excluded.
The following variables were extracted: age (>65 and <65 years old); ethnicity (as per Office of National Statistics principles); sex; setting (inpatient/outpatient); patient participation; and cardiopulmonary resuscitation (CPR) recommendations.8,9 Due to the rapidity of the review, and quality improvement focus, investigators did not directly assess plans, analyse raw data or include additional data items not extracted by the reporting tool.
Rarely, a patient had two current iterations of ReSPECT, either because they had a pilot-phase plan and a plan created after the pilot, or because they had dual records that had been consolidated. As there were more ReSPECT plans than patients, patient characteristics are presented as a proportion of the total number of patients with ReSPECT while information from ReSPECT is presented as a proportion of the total number of plans.
Results
Number of ReSPECT plans and patients
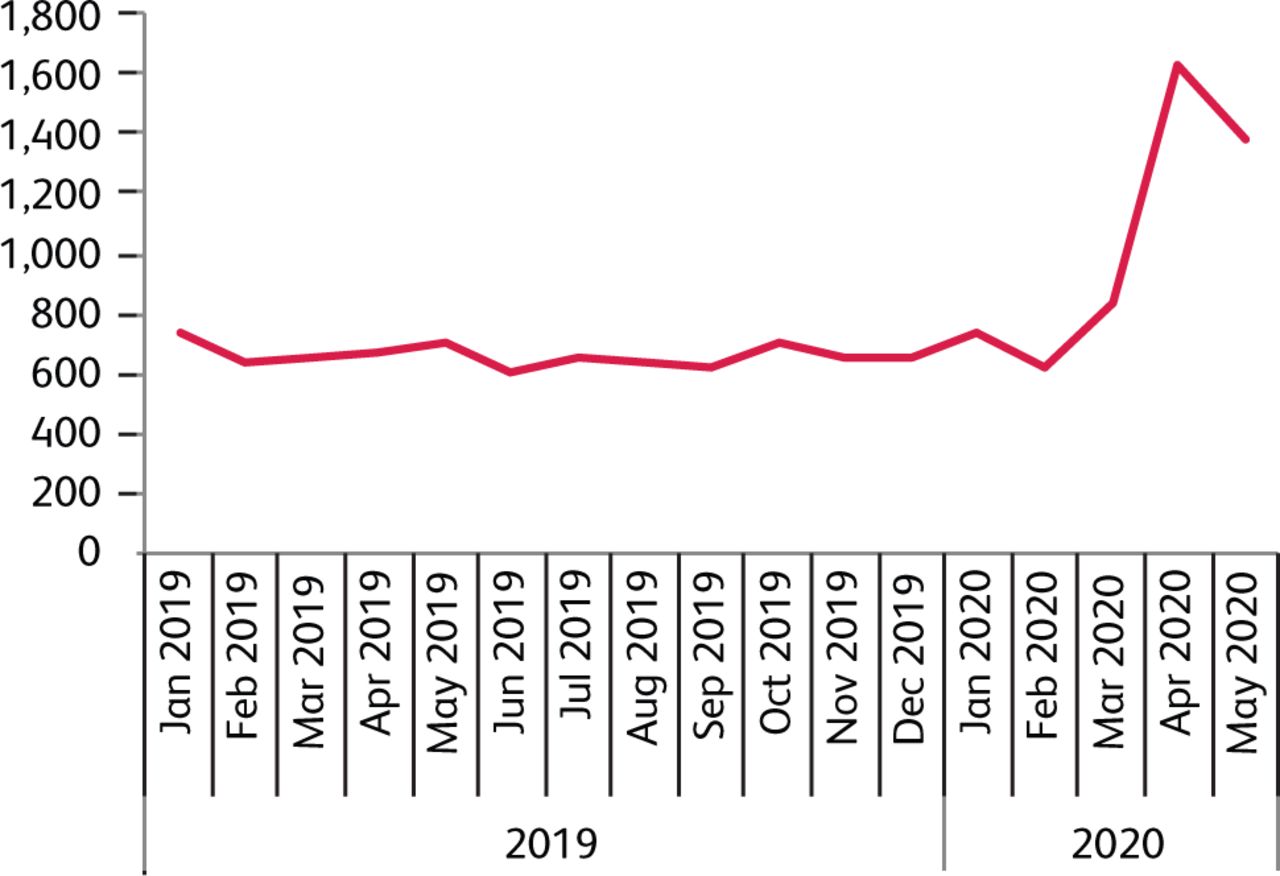
In April 2020, 1,636 patients had ReSPECT initiated or amended, generating 1,637 plans, compared to 7,868 patients and 7,875 plans, 655.7 patients/month, at baseline (Fig 1). The majority were new plans initiated in the respective periods; 1,499/1,637 (91.6%) in April 2020 and 7,670/7,875 (97.4%) in 2019.

Total number of patients with ReSPECT plans initiated/amended per month, demonstrating an increase in the number of patients with ReSPECT plans initiated/amended during the first surge in the COVID-19 pandemic. In April 2020, 1,636 patients had ReSPECT initiated or amended, generating 1,637 plans, compared to a total of 7,868 patients and 7,875 plans during 2019, 655.7 patients per month at baseline.
The prevalence of ACP among hospital inpatients increased by 333.0% during the pandemic: in April 2020, 4,009 adults were admitted and 1,118 inpatient plans were made, amounting to 278.9 ReSPECT plans per 1,000 inpatients compared 84.0 plans per 1,000 patients (7,875/93,751) at baseline.
Demographics
In April 2020, 1,052 (64.3%) patients were over 65 years old compared to 6,788 (86.3%) in 2019. In April 2020, 793 (48.5%) were female compared to 4,357 (55.4%) in 2019. The proportions of people from different ethnic groups in April 2020 and 2019 overall were:
White: 1,372 (83.9%) and 7,235 (92.0%)
Asian: 67 (4.1%) and 211 (2.7%)
Black: 59 (3.6%) and 90 (1.1%)
Mixed: 10 (0.6%) and 18 (0.2%)
Other: 23 (1.4%) and 45 (0.6%)
Unknown: 105 (6.4%) and 269 (3.5%)
The ethnic make up of the population the trust serves is comparable to National data (Table 1).10
Comparative ethnicity data for Leeds (the population served by the hospital trust) and national estimates10
Patient participation in ReSPECT
In April 2020, 1,196 (73.1%) of ReSPECT plans were made with the patient, compared to 4,558 (57.9%) in 2019. During the pandemic, 426 (26.0%) plans were made in the best interests of patients who lacked capacity compared to 3,224 (42%) in 2019.
In April 2020, 575 (72.5%) of women's plans were made with their participation compared to 621 (73.6%) of men's plans. In 2019, 2,521 (58.0%) and 2,032 (58.0%) of plans were made with female and male patients respectively. 497 (85.1%) of plans for those 16–65 years of age were made with their participation compared to 646 (59.7%) in 2019. Though the proportion made with, rather than for, patients over 65 in April 2020, 699 (64.5%), was lower than those under 65, this was an increase on 2019 when only 3,912 (57.6%) plans for those over 65 years were made with patient participation.
During the pandemic, 1,000 (72.8%) plans for White ethnic populations were made with their participation. The proportions of plans made on this basis for other populations in April 2020 and 2019 were:
Mixed: 10 (100%) and 12 (66.7%)
Asian: 49 (73.1%) and 83 (39.3%)
Black: 40 (67.8%) and 38 (42.2%)
Other: 20 (87.0%) and 12 (66.7%)
Unknown: 77 (73.4%) and 125 (45.6%)
CPR recommendation
In April 2020, 1,039 (63.5%) plans contained a DNACPR recommendation compared to 7,670 (97.4%) in 2019. The remaining CPR recommendations in April 2020 and 2019 overall were:
For attempted CPR: 591 (36.1%) and 116 (1.5%)
No formal recommendation: 1 (0.1%) and 28 (0.4%)
Not completed: 6 (0.4%) and 61 (0.8%)
In April 2020, a greater proportion of women's plans recommended DNACPR, 534 (67.3%), compared to 505 (59.8%) of men's plans. In 2019 4,255 (97.6%) and 3,404 (97.2%) of plans for women and men respectively recommended DNACPR.
In April 2020, 149 (25.5%) plans for those aged 16–65 years recommended DNACPR compared to 701 (84.5%) plans for those aged over 65 years. In 2019 this was 1,029 (95.0%) plans for those aged 16–65 years and 6,641 (97.8%) plans for those aged 65 years or over.
922 (67.2%) plans for the White ethnic group specified DNACPR in April 2020 and 7,060 (97.5%) in 2019 compared to the following proportions for other groups:
Asian: 30 (44.8%) and 199 (94.3%)
Black: 11 (40%) and 86 (95.6%)
Mixed: 2 (20.0%) and 17 (94.4%)
Other: 10 (43.5%) 42 (93.35)
Unknown: 52 (49.5%) and 266 (97.4%)
In April 2020, fewer plans, 644 (53.8%), made with the participation of the patient recommended DNACPR than those made for patients without capacity, 385 (90.4%). The proportion of plans for those without capacity recommending DNACPR had fallen from 2019 baseline of 3,161 (98.1%)
Those plans made for patients without capacity recommending DNACPR were discussed as follows in April 2020 and 2019 overall:
Discussed with relative and/or carer: 292 (75.8%) April 2020 and 2,806 (88.7%) 2019
Emergency decision and unable to contact patient representative: 75 (19.5%) and 266 (8.4%)
Discussed with patient: 18 (4.7%) and 89 (2.8%)
Conclusion
In this single centre, the proportion of patients who received ACP increased during the pandemic. A greater proportion of ReSPECT plans were made with the patient during this period when compared to baseline. This increase was seen across all demographic groups analysed. The proportion of patients who participated in ACP during the pandemic increased from baseline notably more for patients aged 65 years and under.
The patient group who received ACP during the pandemic were younger and more ethnically diverse than at baseline. This may reflect changing characteristics of people accessing hospital care due to reduced non-COVID-19 activity and the differential impact of COVID-19 on people from Black, Asian and minority ethnic populations.9,11 As ReSPECT supports recommendations for interventions, as well as advising limits on treatment, and can be created for anyone irrespective of prognosis and diagnosis, its use may have enabled the expansion of advance care planning seen in response to the pandemic.
The proportion of plans containing a DNACPR recommendation was lower in all demographic groups during the pandemic. This may be partially explained by the reduced proportion of patients over 65 years who received ACP, as advancing age is associated with worse CPR outcomes and more DNACPR recommendations.12,13
During the pandemic, those aged over 65 had a notably higher proportion of DNACPR recommendations, Black, Asian and minority ethnic groups had a lower proportion compared to the majority White population and women had a higher proportion than men. While differences based on age, gender and ethnicity have been observed in other studies the discrepancy between men and women, and younger and older groups widened during the pandemic.14,15
The proportion of plans containing a DNACPR recommendation fell irrespective of the level of patient participation. However, the fall was greatest among plans made with patients compared to those made for patients without capacity. While lack of capacity correlates with older age and multimorbidity, both associated with worse CPR outcomes, this in itself does not explain the increasing discrepancy in pandemic period.16 The proportion of plans for patients without capacity specifying DNACPR that were made on an emergency basis was higher during the pandemic than baseline. This may reflect the high risk of rapid deterioration and challenges contacting patient representatives due to restricted visiting.
This study evaluates ACP practice across a large NHS organisation. The findings may not reflect other settings and therefore further detailed evaluation across care settings, capturing broader demographic and clinical information alongside patient experience, is necessary to understand the impact of the pandemic on practice.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}