
Case presentation
A 19-year-old woman, previously fit and well, was admitted 4 days postpartum with a 2-day history of headache, abdominal pain and vomiting. She denied diarrhoea. Her family history was remarkable for her father having lupus and immune thrombocytopenia.
This was her first pregnancy and she delivered at term by normal vaginal delivery. She suffered a minor postpartum haemorrhage (800 mL), but recovered well. Rising proteinuria (urine protein/creatinine ratio 382 mg/mmol) was noted toward the end of the third trimester, but she remained normotensive throughout and had an otherwise unremarkable pregnancy.
On assessment, she was hypertensive at 156/92 mmHg. She was oligoanuric. Neurological examination demonstrated subtle generalised hyperreflexia.
She was found to have a severe acute kidney injury (AKI) associated with a microangiopathic haemolytic anaemia. Her creatinine was 528 μmol/L from a baseline of 53 μmol/L. Her platelet count was low at 25 × 109/L, with a haemoglobin (Hb) of 48 g/L and schistocytes seen on the blood film. Her coagulation screen was normal. Lactate dehydrogenase (LDH) was markedly elevated at 4,836 U/L. Liver function tests demonstrated elevation of bilirubin at 30 μmol/L, with an alanine transaminase (ALT) of 55 U/L and an aspartate transaminase (AST) of 105 U/L.
Diagnosis
The most likely diagnosis was initially thought to be either haemolysis, elevated liver enzymes and low platelet count (HELLP) syndrome or postpartum pre-eclampsia with severe features, given the abnormal liver function tests, the hyperreflexia and the timeline of events.
Other potential differential diagnoses included thrombotic thrombocytopenic purpura (TTP), atypical haemolytic uraemic syndrome (aHUS), retained products of pregnancy and postpartum haemorrhage. The other less likely diagnoses included systemic lupus erythematosus and antiphospholipid syndrome. It is also possible to get thrombotic microangiopathy (TMA) secondary to malignant hypertension of any cause.1
Initial management
The patient was transferred to the intensive care unit for blood pressure control with intravenous labetalol. Pending her ADAMTS13 level result, she was commenced on plasma exchange for possible TTP. Continuous veno-venous haemofiltration was started due to oligoanuric AKI. She was also given intravenous magnesium sulphate for presumed pre-eclampsia.
Her ADAMTS13 result returned as normal at 43%, excluding a diagnosis of TTP. Escherichia coli O157 stool culture was negative, discounting a diagnosis of Shiga toxin-producing E coli haemolytic uraemic syndrome (STEC-HUS). Immunology was negative, including normal antiphospholipid antibody screen and normal antinuclear antibody.
Given the above results, we felt that the patient should commence eculizumab for possible pregnancy aHUS. Her case was promptly discussed with the National Renal Complement Therapeutics Centre in Newcastle upon Tyne, who agreed that we had to consider it as a possible cause of the presentation. The centre's approval is required to obtain eculizumab in the UK and they have a 24/7, consultant-led on-call service. Details can be found on their website at www.atypicalhus.co.uk/emergency-referrals. Within 24 hours she had received her first dose of eculizumab. She was also commenced on prophylactic antibiotics and vaccinated against meningococcus.
Progression and outcome
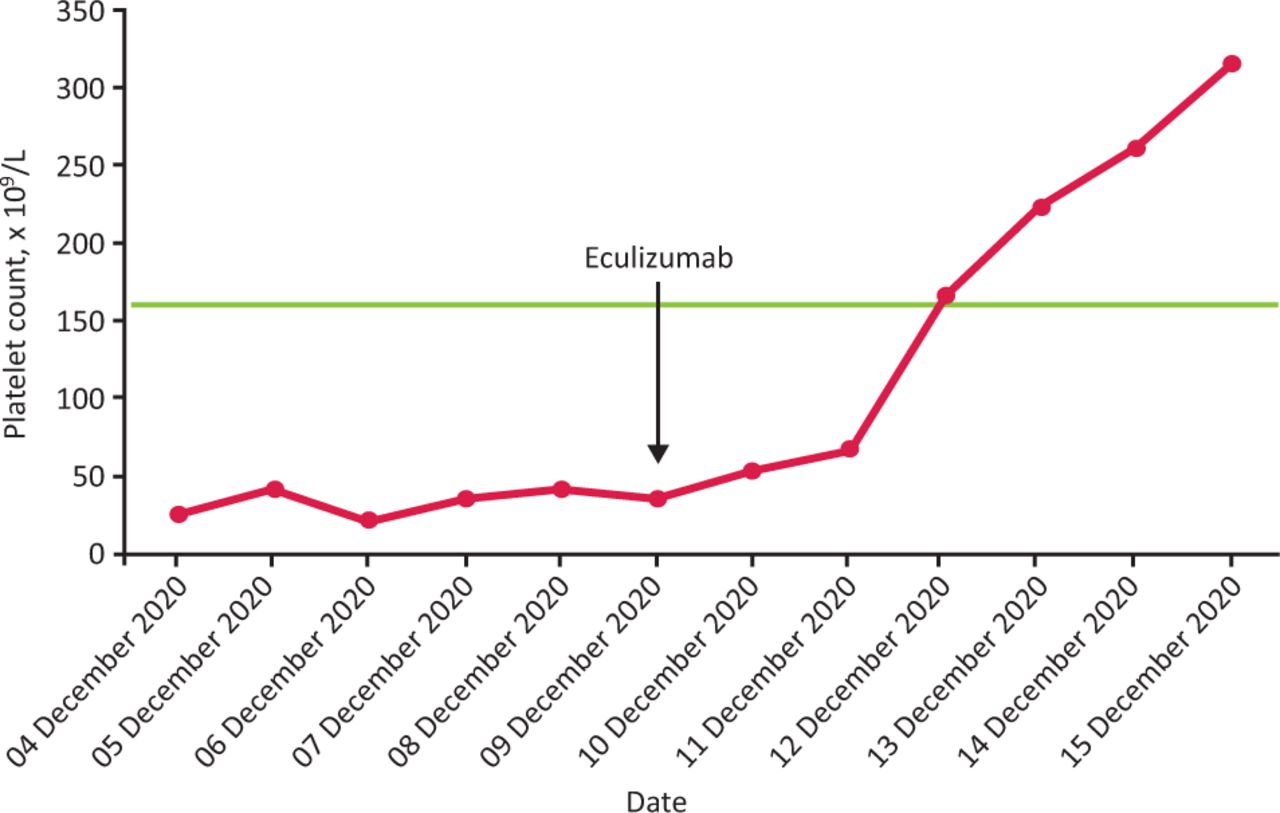
Following the first dose of eculizumab, the patient's blood pressure normalised and she was transferred to the nephrology ward. Her platelet count rapidly climbed to normal levels within days (Fig 1).
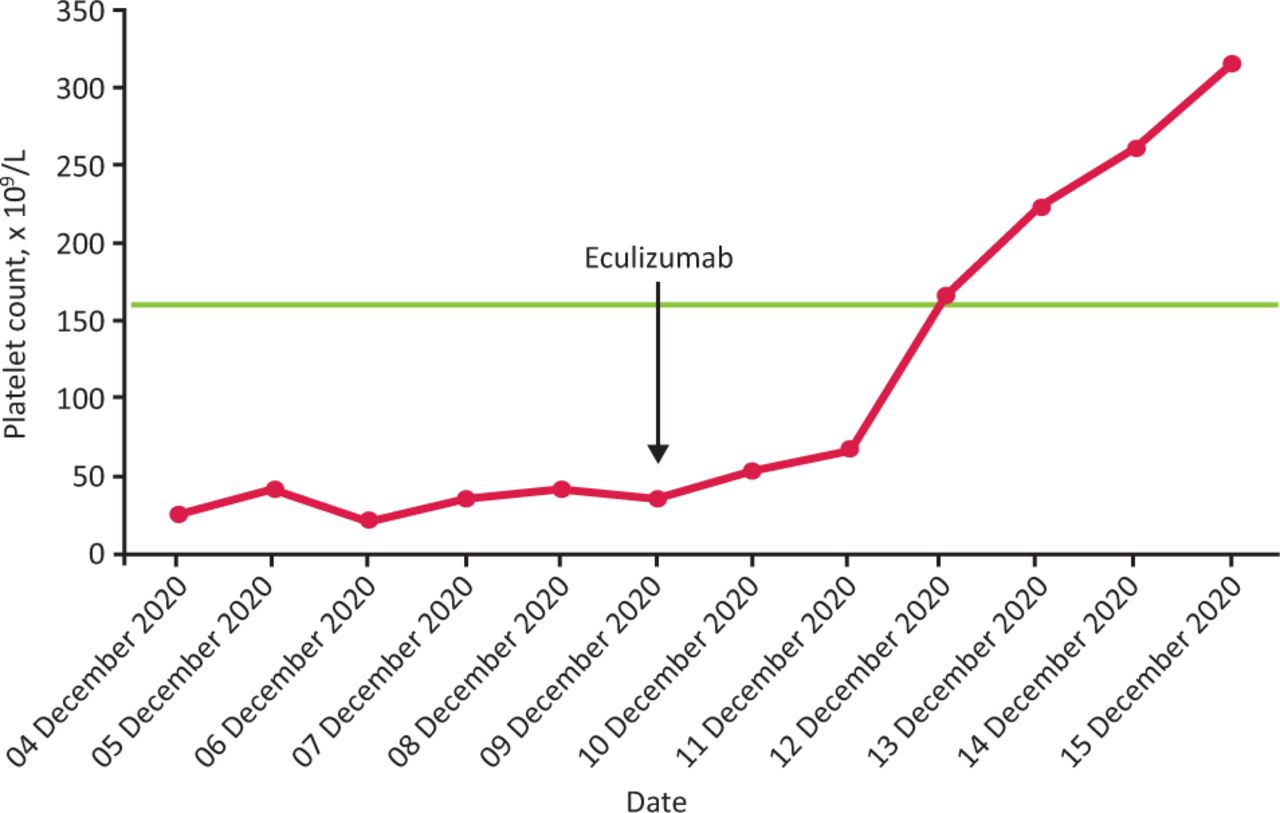
Platelet count progression before and after eculizumab administration. The green line indicates the lower end of the normal range.
She remained dialysis dependent and anuric; therefore, a tunnelled dialysis catheter was inserted. The patient declined a renal biopsy due to the risk of further delay in getting home to her baby.
Remarkably, 4 weeks later, her renal function had almost completely recovered (creatinine of 86 μmol/L), which allowed the discontinuation of dialysis. Her blood pressure was 117/77 mmHg on no treatment.
Further communication with Newcastle led to genetic complement analysis, revealing a complement factor H (CFH) mutation – c.182delA p.(Asn61fs) – for which she is currently maintained on fortnightly outpatient eculizumab infusions. Her family are being counselled on genetic testing.
Discussion
TMA is a group of disorders characterised by a triad of intravascular microangiopathic haemolytic anaemia, thrombocytopenia and vascular thrombosis.2 In the postpartum period, TMA is usually found in association with HELLP syndrome or pre-eclampsia, but can rarely be due to pregnancy aHUS or TTP.3
Due to similar features, differentiating between aHUS/TTP and pre-eclampsia or HELLP syndrome can be difficult, but an open mind is required, guided by clinical clues (Table 1). Making the correct diagnosis is critical, as there are specific therapies for TTP and aHUS which need urgent initiation (Table 1).3 The challenge with aHUS is that a definitive diagnosis through genetic testing takes many weeks. Treatment, which is expensive and (in the UK) requires approval from Newcastle, cannot be delayed during this time.
Differentiating clinical signs between atypical haemolytic uraemic syndrome and pre-eclampsia / haemolysis, elevated liver enzymes and low platelet count syndrome
aHUS is a rare, genetically determined dysregulation of the alternative pathway of the complement cascade. A trigger to activate complement is required to manifest the disease, with pregnancy and delivery both being powerful triggers.4 Our patient had a CFH mutation. CFH is a plasma protein that regulates the alternative pathway. Over 120 CFH mutations have been identified in patients with aHUS.5
Treatment of aHUS involves complement blockade. Eculizumab is a recombinant monoclonal antibody that inhibits terminal complement activation at the C5 protein and thereby reduces haemolysis and TMA. Treatment is potentially lifelong, although research is underway into the risk of relapse on treatment cessation. Patients require vaccination against Neisseria meningitidis and prophylactic antibiotics.6
Key points
TMA in pregnant or postpartum women is potentially a life-threatening condition.
Where clinically suspected, the priority is to exclude TTP and (in the UK) to have timely discussion with Newcastle to streamline investigations and allow prompt treament with eculizumab.
In complex or critical cases, we recommend a multidisciplinary team discussion involving critical care, haematology, obstetrics and nephrology to expedite diagnosis and treatment, which could be life-saving.
Early treatment with eculizumab was critical in our patient's renal recovery.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.