
ABSTRACT
Klinefelter syndrome (KS) is the most common sex chromosome disorder in males. It is the result of two or more X chromosomes in a phenotypic male. In addition to primary hypogonadism affecting male sexual development, it is associated with a series of comorbidities such as osteoporosis, psychiatric and cognitive disorders, metabolic syndromes, and autoimmune diseases. A broad spectrum of phenotypes has been described and many cases remain undiagnosed throughout their lifespan. In this case report, we describe a case of mosaic KS unmasked by acute vertebral fracture.
Case presentation
A 56-year-old man presented to the emergency department with worsening back pain of a 2-week duration despite rest and analgesia prescribed by his family physician. The injury was sustained after an accidental fall from standing height. He had been diagnosed with major depressive disorder, hypertension and hyperlipidaemia. On examination, his vitals were stable with intact neurological function of his lower limbs and normal anal tone.
Radiological investigation confirmed a T7 vertebral compression fracture. To exclude the possibility of a malignancy-related pathologic fracture, computed tomography (CT) of the chest, abdomen and pelvis was performed, which did not detect any sinister lesion. Surprisingly, biochemical evaluation for a secondary cause of osteoporosis revealed severe hypogonadism due to primary testicular failure (Table 1). Bone densitometry demonstrated disproportionately lower bone mineral density (BMD) in the lumber spine than hip (Table 2).
Initial investigations done for secondary osteoporosis
Bone mineral density at baseline and 1 year after initiation of treatment
On further review, the patient reported having sexual dysfunction for many years, including the loss of libido, reduced erections and ejaculation. These symptoms were affecting his sexual activity frequency and satisfaction in his current relationship, which contributed to his depression. Of note, he did not have any biological children from his previous marriage of more than a decade. Additionally, he had been troubled by poor energy level and concentration, which he had attributed to ageing, mood disorder and antidepressant therapy. As a child, he had learning difficulties and dropped out of school at the age of 11 years. Otherwise he was not able to recall the onset of puberty and other pubertal changes during adolescent years. With regards to the aetiology of primary hypogonadism, there was no history of testicular trauma or infection. He was not taking any medications that inhibit androgen biosynthesis. He had no previous exposure to radiotherapy or chemotherapy.
Physical findings were most striking for the presence of eunuchoid body proportions (arm span greater than height by 5 cm), central adiposity (waist circumference of 108 cm), gynaecomastia (Fig 1) and small testicular volume of <3 mL bilaterally as measured by a Prader orchidometer. Furthermore, body hair was sparse on the axilla and pubic region, with particular absence of facial hair despite having not shaved for months. His body weight was 60.2 kg (body mass index of 24.1 kg/m2).

Patient presenting with eunuchoid proportions, gynaecomastia, central adiposity and sparse pubic hair.
Progress
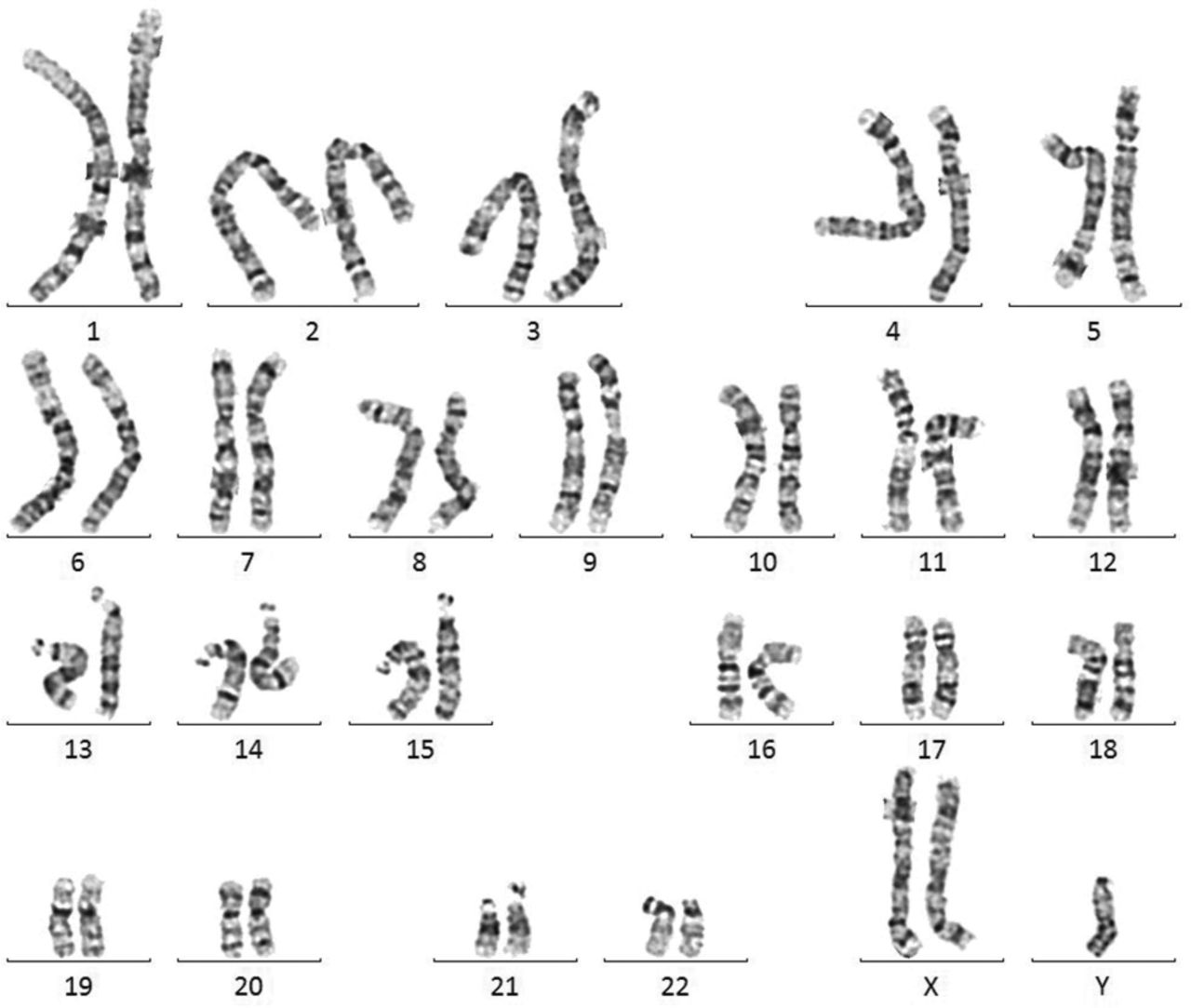
Given the unequivocal laboratory profile of hypergonadotropic hypogonadism, and the lack of previous testicular insult, he was suspected and investigated for Klinefelter syndrome (KS). Karyotyping using peripheral blood lymphocytes confirmed suspected sex chromosome disorder. Interestingly, the karyotype demonstrated 47, XXY / 46, XY mosaicism (Fig 2), diagnosing the patient with mosaic KS instead of the much more common non-mosaic KS (47, XXY).
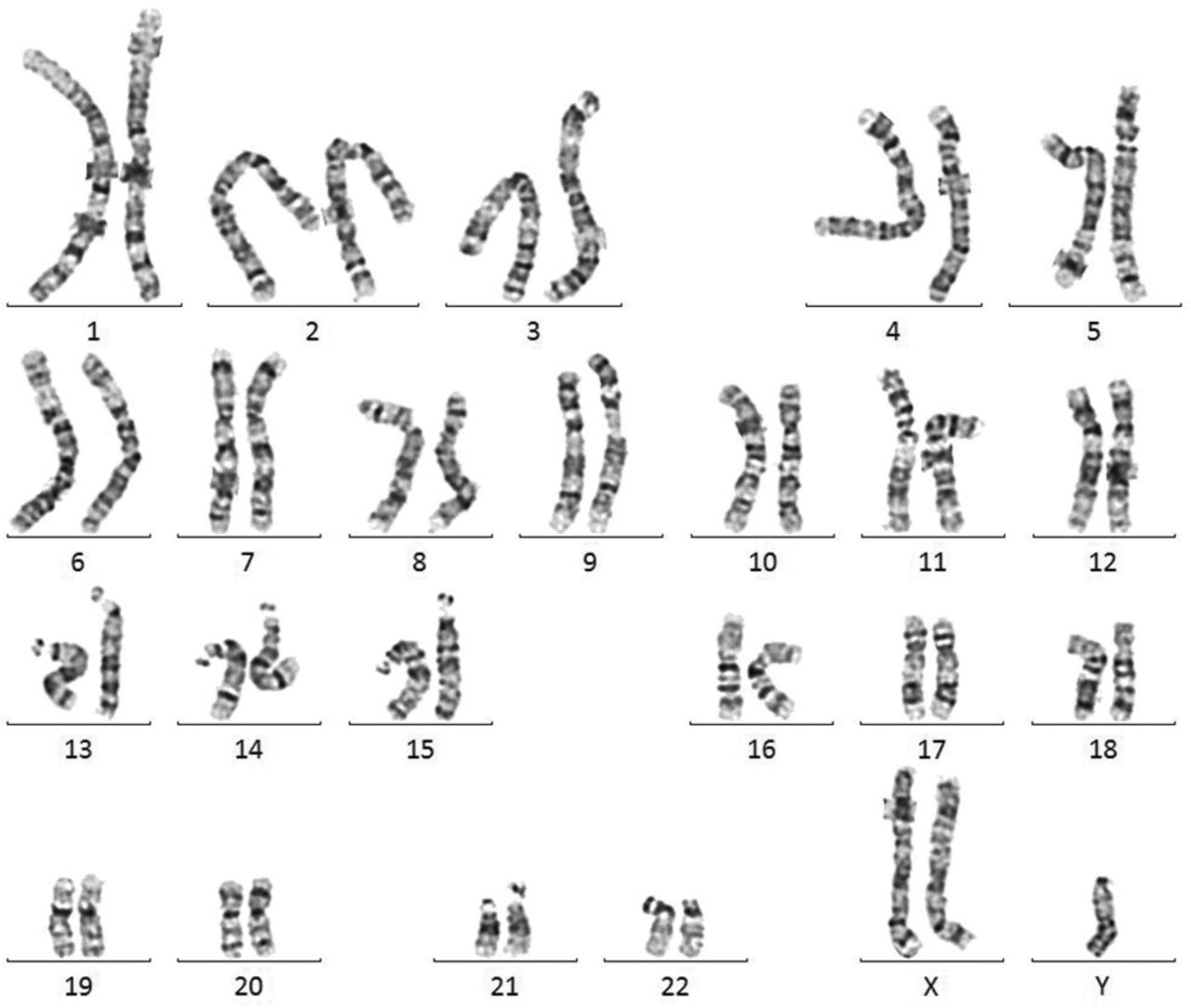
Karyotype demonstrating 47, XXY / 46, XY mosaicism.
The diagnosis and the health implications, including reproductive considerations, of KS were sensitively explained and discussed with the patient. He expressed no desire in fertility, which would otherwise necessitate involvement of reproductive medicine specialists. Long-term testosterone replacement therapy (TRT) was well accepted by him, and long-acting intramuscular depot testosterone undecanoate injection at 3-monthly intervals was commenced shortly after. He reported significant improvement in his sexual symptoms and fatigue in the ensuing 3–4 months of TRT initiation, accompanied by marked resolution of his depressive symptoms such that his antidepressant was successfully discontinued by his psychiatrist.
Specific to his vertebral compression fracture, oral alendronate therapy and cholecalciferol supplementation were started for secondary prevention. Remarkably, in combination with adequate testosterone replacement as guided by serial serum testosterone levels, significant improvement in both spine and hip BMD was observed after 12 months (Table 2). Safety parameters including serum haematocrit and prostate specific antigen (PSA) were reassuring at all his follow-up visits.
Discussion
Over half of men with osteoporosis complicated by vertebral fracture are found to have secondary causes, of which, hypogonadism contributes to 20% of these cases.1 In a study of 87 consecutive men with KS from tertiary endocrine centres, nearly one in five was found to have a vertebral fracture, and that was significantly associated with higher age at diagnosis, likely implying the greater risk of poor bone health with delayed diagnosis and treatment.2 Another important finding was the lack of difference in Fracture Risk Assessment Tool (FRAX) score between those with fracture and without fracture, highlighting the inadequacy of traditional assessment method in determining fracture risk in hypogonadal men.2 The theoretical application of the FRAX algorithm to this patient prior to his spine fracture would only yield 10-year probability of 1.8% for major osteoporotic fracture and 0.2% for hip fracture, well below the thresholds for intervention.
Our patient was found to have mosaic KS, which is rarely encountered in a clinical setting. Only approximately 10% of men with KS have mosaicism (47, XXY / 46, XY) with 47, XXY present in some tissues and the normal karyotype in other tissues, which is due to post-fertilisation mitotic nondisjunction during early foetal development.3,4 Not surprisingly, milder disease including higher testosterone level and larger testicular volumes are typically observed in KS mosaicism.5 In addition, patients with 47, XXY / 46, XY mosaicism are diagnosed later in life between 14.5 and 62 years.6 Nevertheless, the profound testosterone deficiency and associated fragility fracture in this patient illustrates the wide spectrum of disease manifestations possible in mosaic KS.
Key points
It is important to consider and evaluate for secondary causes of bone loss in men diagnosed with osteoporosis.
Variable phenotype can often lead to delayed diagnosis and atypical presentation in mosaic KS patients.
The combined use of TRT with alendronate for a hypogonadal KS patient with severe osteoporosis was effective in improving BMD.
Acknowledgements
We would like to thank cytogenic laboratory, Singapore General Hospital, for sharing the karyotype of our patient.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.