
ABSTRACT
Over 50 systemic conditions may affect the pleura and, thus, unilateral pleural effusions may present for a variety of reasons. Investigating the cause is essential to providing appropriate management. Various pleural interventions are available in current practice, but have varying diagnostic sensitivity. It is, therefore, vital to consider the intervention with the highest diagnostic yield appropriate to the particular clinical situation. The diagnostic pathway in unilateral pleural effusion is increasingly outpatient based, avoiding hospitalisation, which is particularly relevant with the recent COVID-19 pandemic.
Key points
Patients with pleural effusions may present with breathlessness due to impaired gas exchange, reduced ventilatory capacity and abnormal movement of the thoracic cage and diaphragm.
Investigation of a unilateral pleural effusion should be carefully considered, taking into account the likely underlying aetiology, the patient's clinical condition and the need for further investigation and/or intervention.
Thoracic ultrasound is essential prior to all interventions for pleural effusion and should be performed by trained operators.
Local anaesthetic thoracoscopy aids diagnosis in exudative pleural effusions of unknown aetiology.
An indwelling pleural catheter may be a useful first-line intervention in suspected or confirmed cases of malignant pleural effusion.
Introduction: case presentation
A 67-year-old man with a background of atrial fibrillation on edoxaban presented with a 4-week history of worsening breathlessness. There is a 40-pack-year smoking history with previous asbestos exposure as a builder. The World Health Organization performance status is 0 and the general practitioner arranged a chest X-ray (CXR; Fig 1).

Initial chest X-ray.
What is the cause of this patient's symptoms?
This patient has a unilateral moderate sized right pleural effusion.
Some patients with pleural effusion may have minimal symptoms, but others may experience breathlessness with reduced exercise capacity. This can be associated with normal or reduced oxygen saturation. The physiology of breathlessness associated with pleural effusion is not well understood but it is likely to be contributed to by reduced ventilatory capacity and gas exchange as well as by abnormal movement of the respiratory muscles with reduced expansion of the thoracic cage and splinting of the diaphragm.1,2
What is the cause of the pleural effusion?
Although the aetiology of this patient's pleural effusion is unknown, certain risk factors (including the smoking history and asbestos exposure) would suggest that a malignant pleural effusion is most likely. Ipsilateral chest pain may suggest malignant mesothelioma.
Pleural effusions are classified by their biochemical properties into exudative and transudative effusions but can also be due to blood, pus and chyle (Table 1).3 Applying Light's criteria may be helpful to diagnose an exudative effusion (Box 1).4 However, 25% of transudates are misclassified as exudative effusions and, therefore, calculating the serum to pleural fluid albumin gradient may be necessary to avoid misdiagnosis.4 Exudative effusions are commonly caused by infection, malignancy and inflammatory disorders, such as rheumatoid arthritis. Malignant pleural effusions (MPE), more common in lung and breast malignancies, affect up to 15% patients with cancer.5 Transudative effusions, often bilateral, are usually caused by an imbalance in hydrostatic and oncotic pressure and are associated with cardiac, renal or hepatic failure. Non-malignant pleural effusions have been shown to carry high 1-year mortality rates.5 Up to 30% of pleural effusions are multifactorial and therefore accurate aetiological diagnosis is essential as it directs subsequent management.6
Common causes of exudative and transudative pleural effusions
Light's criteria for exudative effusions
The patient attends the ambulatory pleural clinic for assessment the following week.
What is the most appropriate intervention?
In patients with suspected undiagnosed malignant effusion, a therapeutic pleural aspiration may be performed while planning ahead for further intervention in the event of non-diagnostic pleural fluid cytology. Edoxaban was withheld for 48 hours prior to the procedure due to bleeding risk. The patient improved symptomatically following 1.1 L aspiration. The pleural fluid was sent for biochemical (protein, lactate dehydrogenase (LDH) and glucose), microbiological and cytological analysis.
Intervention in pleural effusions can be performed for diagnostic and therapeutic purposes. Where the cause of an effusion is unclear, a decision on the most appropriate intervention should be considered carefully based on:
the patient's symptoms and/or clinical condition
whether the aetiology of the pleural effusion has been established
whether further investigation may be required.
It should be noted that, when performing pleural procedures for fluid, it is essential to use immediate or real-time thoracic ultrasound (TUS). This followed the 2008 National Patient Safety Alert (NPSA) report that highlighted cases of death and severe harm resulting from chest drain insertion.7 The British Thoracic Society (BTS) has recently published training standards in TUS for respiratory clinicians that also addresses the provision of acute and emergency ultrasound.8 In addition, non-urgent procedures should not be performed if coagulopathy is present. The BTS advises to avoid procedures in anticoagulated patients until international normalised ratio <1.5; direct oral anticoagulants should be withheld for 24–48 hours dependent on renal function and risk of bleeding, and therapeutic low-molecular weight heparin should also be withheld for 24 hours.9,10
Diagnostic thoracocentesis
Diagnostic thoracocentesis is an appropriate initial investigation in most patients. Performed under ultrasound guidance, it is a minimally invasive procedure that enables pleural fluid analysis to aid diagnosis. Pleural fluid cytology has variable diagnostic sensitivity in MPE. Previous BTS guidelines quoted a diagnostic accuracy of 60%, however, a recent study found that overall pleural cytology sensitivity is approximately 45%–55%.11,12 Diagnostic sensitivity is higher in ovarian, breast and lung (adenocarcinoma) malignancy at 95%, 71% and 82%, respectively. In malignant mesothelioma, previous studies suggested diagnostic sensitivity between 16% and 73%.13,14 Although, Arnold et al recently showed that it was closer to 6%.12 In addition, while BTS guidelines advise a minimum volume of 20–40 mL pleural fluid is required for diagnosis, it has been found that a minimum volume of 75 mL increases diagnostic sensitivity.15,16 Even if a diagnosis is obtained, the material may not always be sufficient for molecular markers / driver mutations, which will aid in decision making for appropriate immunotherapy or targeted molecular therapy.
Therapeutic thoracocentesis
Therapeutic thoracocentesis performed under ultrasound guidance allows for pleural fluid analysis to aid diagnosis, as well as removal of a larger volume of pleural fluid to provide symptom benefit. The procedure avoids the insertion of a chest drain and, therefore, can be performed on ambulant patients in an outpatient setting to avoid hospitalisation. If pleural fluid cytology is non-diagnostic, residual pleural fluid enables further invasive procedures to be performed including image-guided pleural biopsy or local anaesthetic thoracoscopy.
Intercostal chest drain
Intercostal chest drain (ICD) insertion performed under ultrasound guidance enables pleural fluid analysis, complete drainage of the pleural effusion and administration of intrapleural agents, if required. Commonly, talc slurry pleurodesis is administered through the ICD to prevent recurrence of probable or confirmed MPE. Talc slurry pleurodesis has a failure rate of 24%.17 This option may be appropriate for symptomatic patients with large volume pleural effusions who are non-ambulant with poor performance status where further invasive tests may not be appropriate or where the aetiology of the effusion is known.
The BTS guidelines advise caution if removing >1.5 L of pleural fluid on a single occasion due to the risk of developing re-expansion pulmonary oedema (RPO), a condition that can lead to cough, chest pain and even cardiovascular instability and collapse.18 Following 16 cases of RPO between 2017–2020, an NPSA alert has highlighted the need to ensure controlled drainage following ICD insertion to avoid this potential complication.19 Clinicians should be mindful that interventions for pleural effusion, despite the use of thoracic ultrasound, should be avoided out-of-hours unless in an emergency to minimise unnecessary errors and complications.
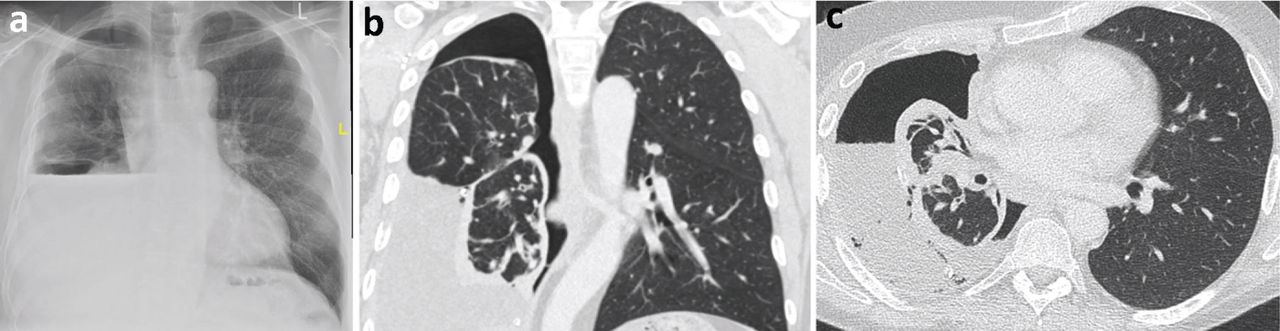
A CXR following therapeutic thoracocentesis revealed a hydropneumothorax (Fig 2a), raising the possibility of a non-expandable lung (NEL). Pleural fluid analysis suggested an exudative effusion (protein of 40 g/L and LDH of 620 IU). Cytology revealed a lymphocytic effusion with no malignant cells seen. Computed tomography of the chest (Fig 2b and 2c) demonstrated a parietal pleural rind predominantly encasing the right lower lobe, likely causing the NEL.

a) Chest X-ray post-thoracentesis demonstrating hydropneumothorax (air and fluid in the pleural cavity). b) Computed tomography of the chest, coronal view. c) Computed tomography of the chest, axial view.
What is the next most appropriate intervention?
As the pleural fluid cytology was non-diagnostic, the patient proceeded to a thoracoscopy under local anaesthetic and moderate sedation, also known as local anaesthetic thoracoscopy (LAT), medical thoracoscopy or pleuroscopy.
LAT is a medical procedure, performed by respiratory physicians, involving internal examination, biopsy and/or administration of intrapleural agents within the pleural cavity. It is done under moderate sedation and local anaesthesia. The main indication for LAT is in the investigation of exudative effusions of unknown aetiology, particularly when there is no pleural target for CT-guided biopsy and pleurodesis is being considered. LAT is also useful in the diagnosis of pleural tuberculosis with a combined culture/histology sensitivity of up to 100%, depending on prevalence.20
The efficacy of LAT in the diagnosis of malignancy is as high as video-assisted thoracoscopic surgery (VATS) biopsy.21 VATS biopsies are performed by thoracic surgeons, usually under general anaesthesia, with single lung ventilation.
LAT can also be used for therapeutic indications. Pleurodesis by talc poudrage can be undertaken if the pleura appears abnormal on direct inspection. It is as effective as talc slurry in achieving pleurodesis with increased efficacy in patients with lung or breast cancer.16 LAT may also be useful in pleural infections, allowing for division of septations and adhesions and aiding in accurate chest drain placement.22
LAT can be performed using a semi-rigid thoracoscope (Fig 3a), which is of similar design to a flexible video bronchoscope or a rigid thoracoscope (Fig 3b); both yield similar diagnostic accuracy.23

a) Semi-rigid thoracoscope. Reproduced with permission from Olympus Europa SE & Co. b) Rigid thoracoscope.
The patient underwent local anaesthetic (medical) thoracoscopy. This showed extensive nodularity over the visceral and parietal pleural (Fig 4a). A decision was made to insert an indwelling pleural catheter (IPC) at the time of thoracoscopy for likely NEL (Fig 4b).

a) Parietal pleura biopsies taken during a thoracoscopy and thoracoscopic view of a malignant nodule. b) Chest X-ray post-thoracoscopy.
What is the role of indwelling pleural catheters?
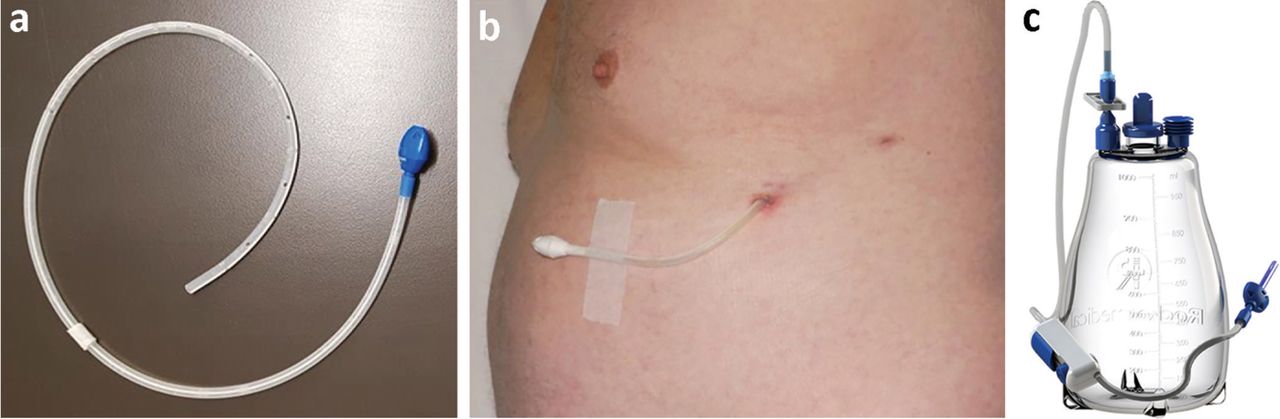
IPCs have established themselves as an important tool in the management of pleural effusions. An IPC is a soft, flexible silicone tube with multiple fenestrations (Fig 5a). It is tunnelled subcutaneously before entering the pleural cavity (Fig 5b). The external portion contains a one-way valve that connects to a closed drainage system with vacuum (Fig 5c).
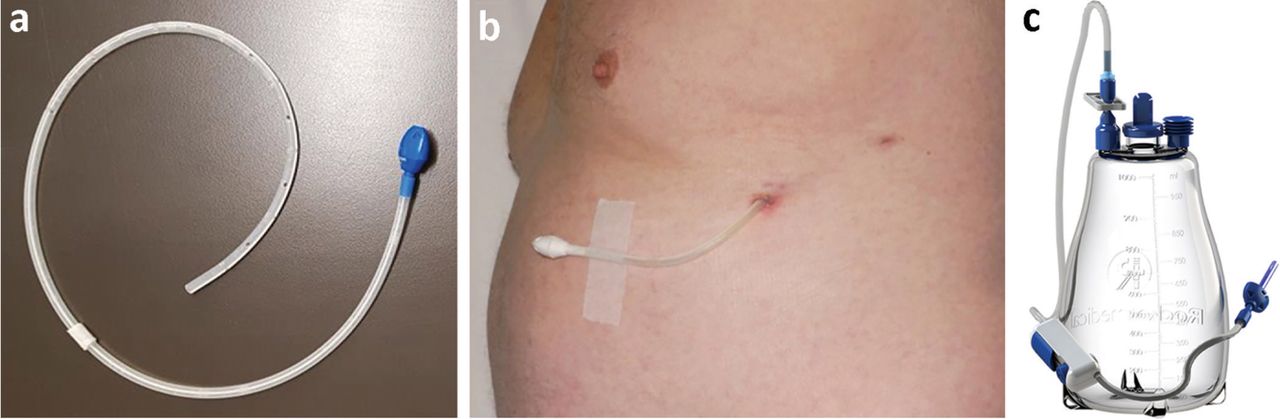
a) The components of an indwelling pleural catheter. b) A tunnelled indwelling pleural catheter. Reproduced with permission from Rocket Medical. c) An indwelling pleural catheter drainage system. Reproduced with permission from Rocket Medical.
IPCs were initially designed as a second-line treatment for patients who have MPE with NEL or failed pleurodesis and can remain in the pleural cavity and outlive the patient. NEL (or trapped lung) occurs when the lung cannot expand after fluid drainage, either because of endobronchial obstruction or visceral pleural encasement by tumour.24
The role of IPCs in pleural effusion management saw a paradigm shift with the publication of the TIME2 and AMPLE trials supporting their use as a first-line treatment.25,26 Depending on patient preference, IPCs may be offered as a first-line treatment in MPEs and are usually done as an elective day case procedure. They are safe and reduce length of hospital stay in patients who would traditionally have needed prolonged and often multiple admissions. IPCs have shifted the management of pleural effusions to a more outpatient-orientated setting.
The drainage of IPCs is supported by district nurses but patients are encouraged to drain and manage their own devices. Drainage frequency is commonly two to three times per week but can be tailored to meet the patient's needs. If the aim is palliation, then symptom-guided drainage may be appropriate.27 However, if the aim is to achieve rapid pleurodesis with subsequent drain removal, then daily drainage may lead to a higher rate of autopleurodesis and faster time to IPC removal.28 Autopleurodesis is defined as spontaneous pleurodesis without the use of a chemical agent. Although not the objective of IPC insertion, it can be observed in up to 51% of patients with MPE.25 Additionally, aggressive drainage with administration of talc via the IPC can result in two-fold higher rates of pleurodesis compared with IPC alone.29
The role of IPCs in non-malignant pleural effusions is less well defined and needs to be tailored to the patient. The first randomised trial on refractory transudative pleural effusions concluded that IPCs did not offer superior control of breathlessness compared with as required therapeutic thoracentesis, with the IPC arm experiencing higher adverse events.30 In hepatic hydrothorax, IPCs can be offered with palliative intent to patients who have exhausted medical management and are not transplant candidates or in some patients as a bridging therapy to manage effusions prior to transplantation.31,32
As IPC use becomes more widespread, clinicians may encounter more IPC-related complications that may occur in 10%–20% of patients.33 Pleural infection, catheter blockage and symptomatic loculations tend to be the most common and can be managed.34 In oncology patients, there is good evidence that there is no increased risk of IPC-related infection by chemotherapy or an immunosuppressed state.35,36
The pleural biopsies revealed malignant epithelioid mesothelioma. Following discussion in the lung multidisciplinary team meeting, the patient was referred to oncology for systemic treatment. The patient continued to drain his IPC three times weekly and subsequently achieved autopleurodesis. The IPC was removed soon after.
Summary
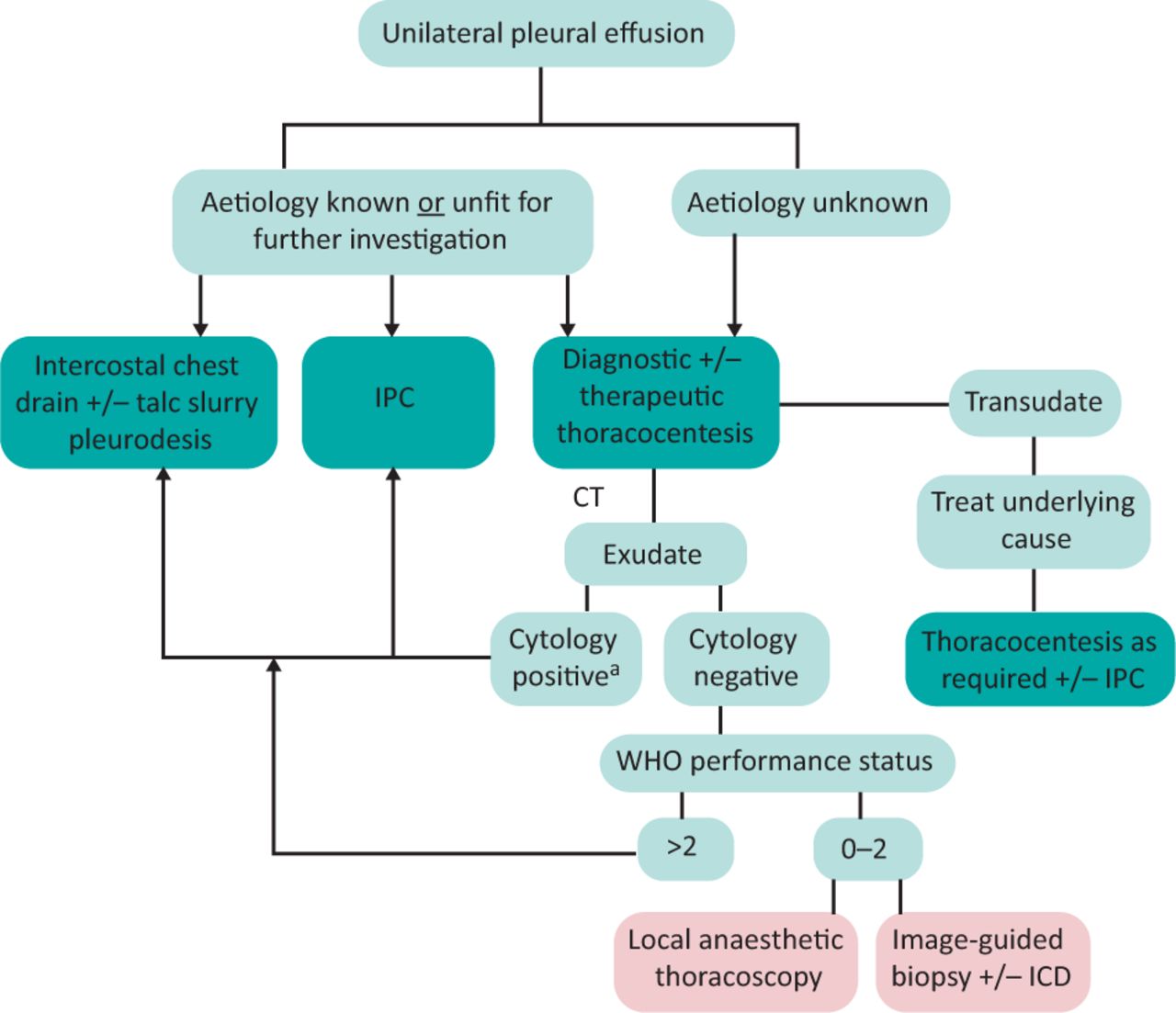
Investigation of a unilateral pleural effusion is a common clinical scenario faced by general and respiratory physicians alike. With the high prevalence of MPE associated with advanced-stage lung cancer and other malignancies, it is increasingly important to perform the correct, as well as most useful, investigation for the patient (Fig 6). This is particularly relevant with recent advances in oncological therapy, whereby diagnosis on pleural cytology alone may be insufficient, and supplementary pleural histology may provide additional information (including molecular analysis) to guide treatment.

Pathway for investigation of a unilateral pleural effusion.aIf further tissue required for molecular testing, consider local anaesthetic thoracoscopy; CT = computed tomography; IPC = indwelling pleural catheter; WHO = World Health Organization.
As with many aspects of modern patient care, the investigation and management of patients with pleural effusions is increasingly managed in an ambulatory fashion. With the adoption of same-day emergency services and pleural clinics in many hospitals, this provides patients with streamlined, efficient and effective care. This has been particularly relevant during the COVID-19 pandemic and reduces cost and risk of hospital-associated infection to the patient. This, together with devices (such as the IPC) that have been designed specifically for patients wishing to remain at home, has allowed the emergence of a modern approach to pleural medicine.
Acknowledgements
The authors acknowledge review of the manuscript by Prof Jonathan Bennett, consultant respiratory physician and honorary professor at University Hospitals of Leicester NHS Trust and chair of the British Thoracic Society.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- Key points
- Introduction: case presentation
- What is the cause of this patient's symptoms?
- What is the cause of the pleural effusion?
- What is the most appropriate intervention?
- What is the next most appropriate intervention?
- What is the role of indwelling pleural catheters?
- Summary
- Acknowledgements
- References
- Figures & Data
- Info & Metrics