
ABSTRACT
Lung cancer continues to be the leading cause of cancer death globally. Delayed diagnosis is a major contributing factor to poor outcomes and remains a key challenge to overcome. While debate around the implementation of lung cancer screening for asymptomatic high-risk individuals continues, rapid access to relevant diagnostic tests is essential. The new National Optimal Lung Cancer Pathway describes ‘diagnostic standards of care’ in an effort to implement best practice, reduce variation and improve delays in diagnosis, staging and treatment of lung cancer. Lung cancer treatment continues to develop with new surgical techniques, radiotherapy options and more drugs being licensed as part of standard treatment. We provide an overview of the core lung cancer diagnostic steps, recognition and management of acute presentations as well as the latest treatment options.
Introduction: the need for speed
Lung cancer remains the leading cause of cancer death worldwide and is responsible for over 1.6 million deaths per year.1 This accounts for approximately 20% of all cancer deaths, and is more than the combined total for breast, colon and prostate cancer.2 In the UK, there are 45,000 newly diagnosed cases every year leading to approximately 35,000 deaths.3 Early-stage disease remains asymptomatic and, therefore, approximately 70% of cases are diagnosed at an advanced stage when cure is no longer possible. In the UK, over a third of lung cancers are diagnosed as an emergency presentation, of which, almost 30% will die within months.4 This is a major contributing factor to current poor survival outcomes, with a 5-year survival rate of just over 15%.3 In contrast, global 5-year survival for early stage T1a tumours (≤1 cm) is as much as 92%. This drops to 83% and 77% for T1b (>1 to ≤2 cm) and T1c (>2 to ≤3 cm) tumours, respectively (Fig 1), demonstrating that every millimetre counts.5 Table 1 outlines how the overall lung cancer stage is calculated based on tumour size (T), nodal involvement (N) and the presence/absence of metastatic disease (M), as per international guidelines.5 A key challenge to therefore overcome in order to improve lung cancer outcomes is earlier diagnosis.
Overall lung cancer stage groupings based on tumour size, nodal involvement and metastases location
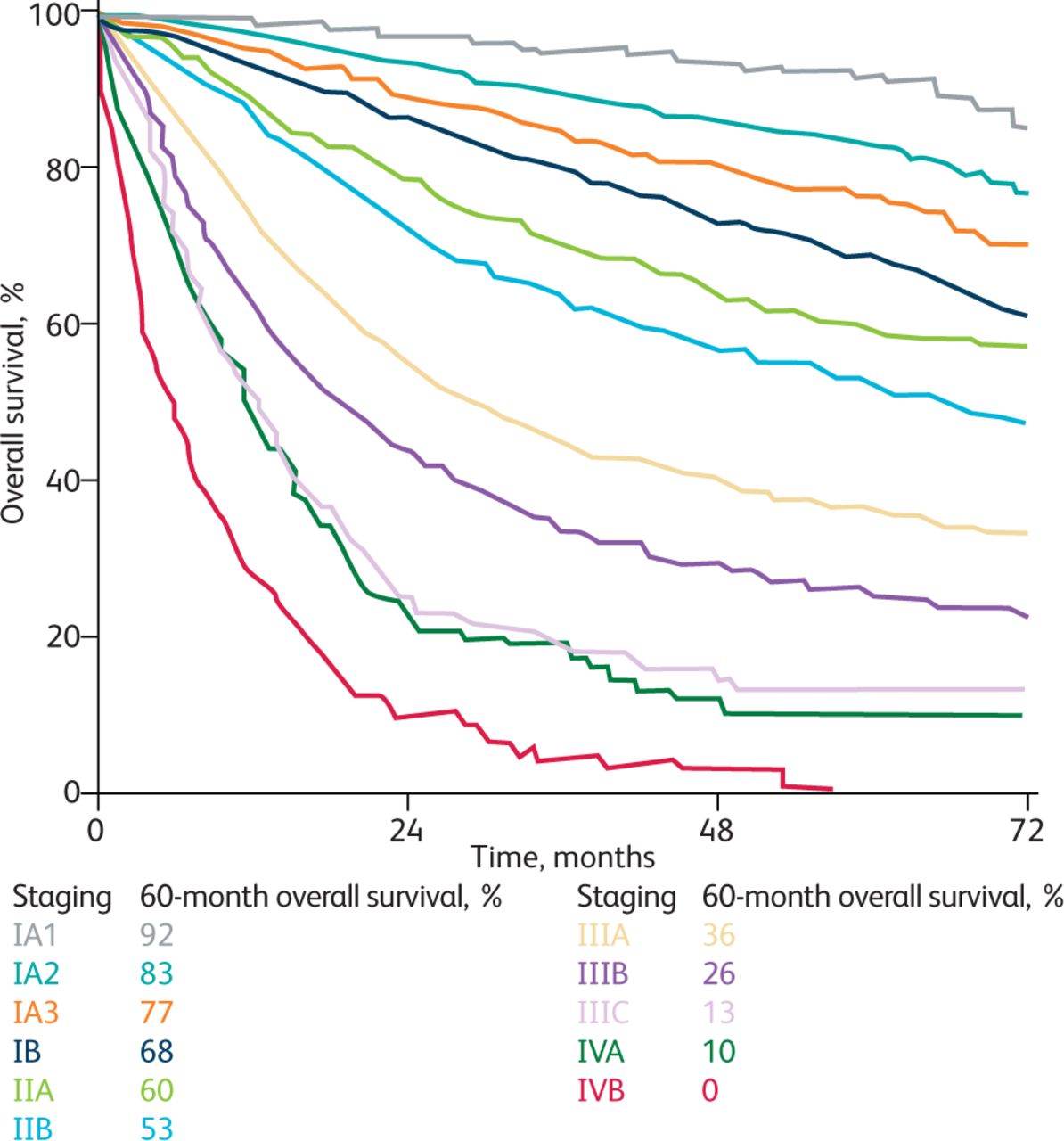
Overall survival by clinical stage according to International Association for the Study of Lung Cancer 8th edition staging. Adapted with permission from Goldstraw P, Chansky K, Crowley J et al. The IASLC Lung Cancer Staging Project: Proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J Thorac Oncol 2016;11:39-51.
While debate around the implementation of lung cancer screening for asymptomatic high-risk individuals continues, practising physicians need to remain vigilant, to have a high index of suspicion for lung cancer in individuals with the relevant risk factors (particularly smoking) and to have a low threshold for initiating investigations either through ‘suspected cancer pathway referral’ into their local diagnostic centres or by undertaking computed tomography (CT), if available.
Investigations: proactive, not reactive
Rapid access to diagnostic tests through accelerated pathways is a central component of the national cancer programme.6 The new National Optimal Lung Cancer Pathway was introduced in an effort to implement best practice, reduce variation and improve delays in diagnosis, staging and treatment of lung cancer.7 Patients with suspected lung cancer are expected to complete all their diagnostic tests to confirm or refute suspicion within 28 days. Reducing diagnostic pathways from an average of 30 days to 14 days is associated with a significant improvement in median overall survival.8 The key initial investigation remains CT. When CT confirms suspected lung malignancy, the pattern of disease on initial CT should drive the subsequent diagnostics tests guided by ‘diagnostic standards of care’ (DSOCs), summarised in Table 2. These are readily available and free online with clear diagrammatic descriptions.7 The DSOCs outline all the diagnostic investigations required for the multidisciplinary team to accurately diagnose and stage the disease, and to assess fitness for treatment. This more ‘proactive’ approach, as opposed to the conventional ‘reactive’ approach that lent itself to delays, avoids variation in practice and ensures all relevant tests are done in a timely manner. The real-world implementation of such rapid diagnostic standards has already been demonstrated in UK settings.9
Summary of the diagnostic standards of care to guide appropriate investigations for suspected lung cancer7
Emergency presentations: reasons for admission and management priorities
As outlined earlier, a significant proportion of lung cancers present as an emergency with advanced symptomatic disease. Here, we discuss some of the more common reasons for admission and outline initial management priorities.
Endobronchial obstruction
Patients may present with breathlessness due to lobar collapse, or even whole lung collapse, and/or pneumonia secondary to endobronchial obstruction. Initial management will usually be with antibiotics, if required and appropriate. Non-pharmacological measures may include oxygen for hypoxaemia, chest physiotherapy for breathlessness and morphine where appropriate. Some patients may later, after appropriate investigation and work-up, be considered suitable for radiotherapy or endobronchial debulking / stent placement, but this is often not required as an emergency and such decisions should be overseen by the lung cancer multidisciplinary team.10
Haemoptysis
Low-volume haemoptysis can occur in lung cancer but, fortunately, massive haemoptysis is rare and more commonly associated with non-malignant conditions (such as bronchiectasis and aspergilloma). Most patients with small-volume bleeding due to lung cancer can be discharged safely for outpatient management. Definitions of massive haemoptysis vary, but expectoration of 100-200 mL of blood in a 24-hour period should raise concern. In such cases, the priority is standard resuscitation measures, including ensuring that the airway is secure. In some instances, this may require intubation if appropriate and occlusion of the affected main bronchus with a dual-lumen endotracheal tube. The patient should be managed lying on the affected side (‘good lung up’). Correction of any coagulopathy is important and tranexamic acid is often used. CT angiography can help to identify the exact site of bleeding. Radiologically-guided embolisation of a target vessel, radiotherapy or surgery can all be possible methods of treatment depending on the precise source of bleeding and on what facilities are available locally.11 Depending on the stage of the lung cancer, a more palliative approach may be appropriate in more advanced disease with a poor outlook.
Superior vena cava obstruction
Symptoms of superior vena cava obstruction (SVCO) include facial swelling, headaches, plethora and venous distension over the anterior chest wall and neck. It is caused by extrinsic compression of the SVC, and occasionally by intraluminal clot, and lung cancer accounts for around 70% of cases.10 It is an oncological emergency and usually requires inpatient admission, investigation and treatment. Urgent contrast CT should be undertaken to identify the cause as the definitive management is treatment of the underlying condition. In those patients with suspected malignancy, urgent biopsy (either radiologically guided or endobronchial) is the key investigation as this will inform subsequent treatment selection, such as urgent chemotherapy for small-cell lung cancer (SCLC) or stent +/− radiotherapy for non-small-cell lung cancer (NSCLC).10 In general, the use of steroids before biopsy is not advocated as this can reduce the yield from histological samples but, in severe cases, dexamethasone can be considered.
Spinal cord compression
Spinal cord compression and cauda equina syndrome should always be considered in lung cancer patients with progressive back pain, especially when associated with neurological symptoms. There should always be a high index of suspicion, and these patients should be admitted as an emergency for urgent magnetic resonance imaging (MRI) of the whole spine with onward referral to the local acute oncology services if cord compression is confirmed as urgent treatment with radiotherapy or surgery might be required to preserve neurological function. Treatment with high-dose dexamethasone should be initiated from the outset.10
Hypercalcaemia
Hypercalcaemia is most commonly, though not exclusively, related to squamous-cell lung cancer and is usually due to production of parathyroid hormone-related peptide (PTHrP), although it can also be caused by bone metastases. It is usually associated with a poor prognosis. Initial management is with fluid replacement (1-3 L initially) and intravenous (IV) bisphosphonates (zoledronate or pamidronate). Many centres will have their own local treatment guidelines. Definitive management is treatment of the underlying malignancy.
Hyponatraemia and syndrome of inappropriate antidiuretic hormone secretion
The syndrome of inappropriate antidiuretic hormone secretion (SIADH) is common in patients with extensive SCLC, which should be suspected in the hyponatraemic patient with abnormal chest radiology.12 Diagnosis is made by comparing serum sodium and osmolality (low) with urine sodium and osmolality (inappropriately high). Initial management involves fluid restriction and withdrawal of any exacerbating medications. Options for SIADH unresponsive to fluid restriction are the antibiotic demeclocycline (which induces nephrogenic diabetes insipidus) and the competitive selective vasopressin receptor 2 antagonist tolvaptan (caution in liver disease and diabetes).10 Local protocols and drug formularies should be followed. Demeclocycline is often used as a first-line treatment in the UK, with tolvaptan reserved for those cases not responding to demeclocycline or those unable to tolerate it, although tolvaptan may be a first-line treatment in other countries. The definitive management of malignant SIADH is the treatment of the underlying cause so, if appropriate, urgent tissue diagnosis should be obtained when malignancy is suspected.
Pleural effusion(s)
This is covered in detail in an accompanying article, but pleural effusions are a common cause of breathlessness in the patient with lung cancer. In general, the presence of a malignant effusion is often indicative of more advanced disease with a poorer prognosis, and symptomatic relief should be prioritised. Many centres now have access to efficient ambulatory pathways for the management of pleural effusions and these patients should be managed in an outpatient setting whenever possible, occasionally requiring symptomatic drainage prior to discharge. This should always be ultrasound guided.
Lung cancer treatment
Treatment for lung cancer depends on the stage of the cancer, the tumour sub-type and the performance status / comorbidities of the patient. Management decisions are made by the multidisciplinary team.
Non-small-cell lung cancer
Surgery
Surgery remains the preferred treatment in early-stage NSCLC, affording patients the greatest chance of cure. Resection rates in the UK have been increasing, from around 9% in 2006 to 18% in 2018. More patients than ever before are now being assessed as suitable for surgical resection since minimally invasive surgical techniques (such as video-assisted thoracoscopy (VATS) and robotic techniques) have become more widely available.
Radiotherapy
Patients with early-stage NSCLC (stage I-IIA) who choose not to have surgery, or who are not considered to be good surgical candidates (often due to poor physiology and/or associated comorbidities), should be offered radical radiotherapy in the form of stereotactic ablative radiotherapy (SABR).13 SABR directs multiple narrow beams of radiation at the tumour from different angles. The tumour receives a higher dose of radiation whereas the surrounding tissues receive a much lower dose, reducing the risk of damage to healthy tissue. Small studies suggest SABR may be comparable with surgery in selected patients.14 The number of fractions required depends on the size and location of the tumour. Currently, it is largely delivered in specialist centres but there is a push to make SABR available more widely to make it easier to access for patients. If SABR is contraindicated, either conventional or hyper-fractionated radiotherapy should be offered, but outcomes are less good compared with surgery or SABR. Palliative radiotherapy also has a significant role in the treatment of thoracic symptoms (for example haemoptysis) and bone metastases.
Systemic anticancer treatment
As with many other cancers, this is a fast-moving field as more drugs are licensed either as monotherapy or in various combinations. The National Institute for Health and Care Excellence (NICE) has adopted a regular review process of their systemic therapy algorithm to reflect this. Where possible, conventional chemotherapy is replaced by biological treatments that target specific mutations / genetic re-arrangements. Immune checkpoint inhibitors are also recommended either alone or in combination with chemotherapy depending on the presence of the immune marker (programmed death ligand 1 (PD-L1)) on tumour cells for both adenocarcinoma (those without a target mutation) and for squamous cell carcinoma. Table 3 summarises the current known targets, the agents available for use in each instance and the more common side effects of each. The non-respiratory physician should be aware of the more common and important side effects of the more frequently used of these drugs (particularly immune checkpoint inhibitors) since patients taking them may present acutely to the general medical take in some hospitals. Fig 2 summarises the adverse side effects associated with cancer immunotherapy.
Summary of currently approved targeted therapy for lung cancer and associated side effects
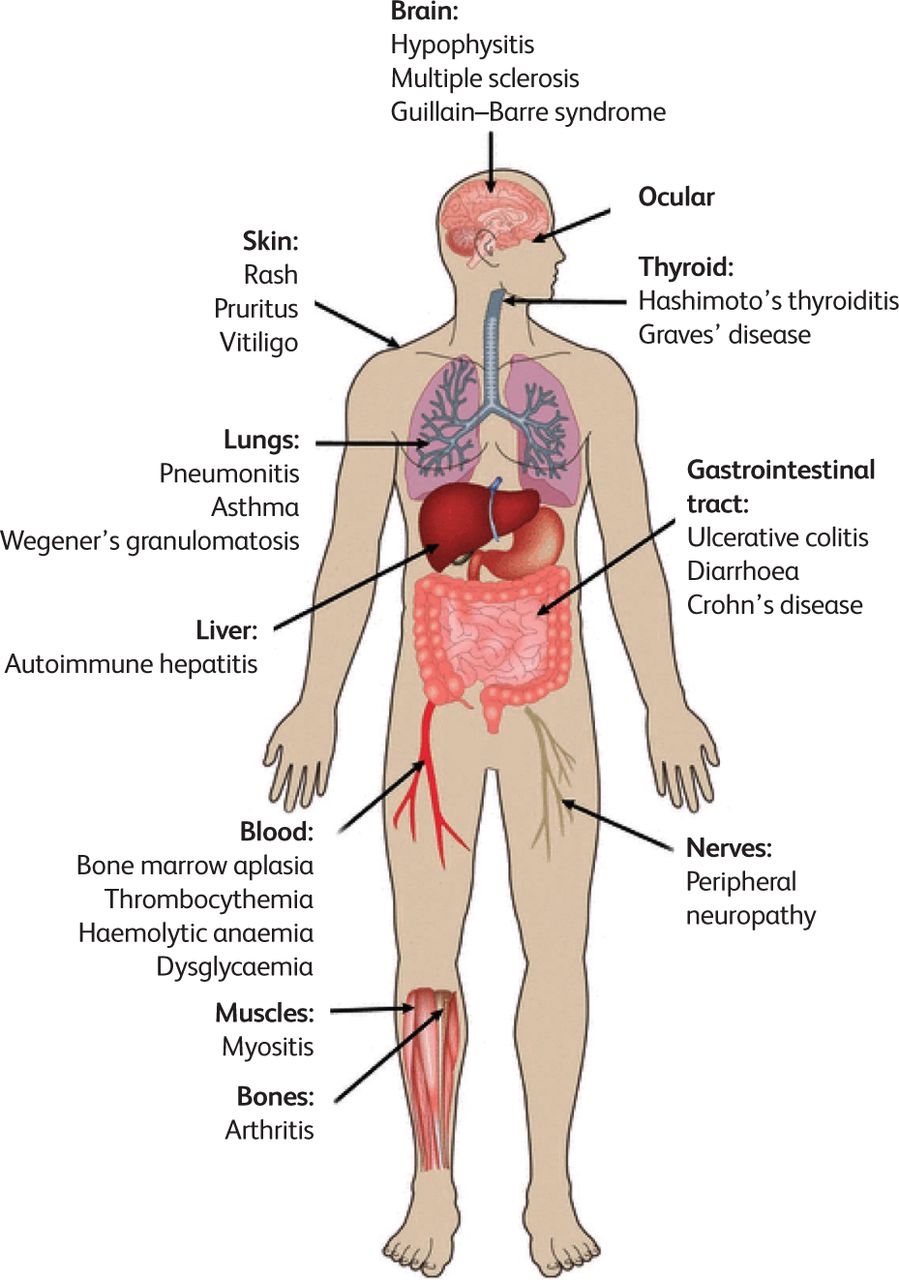
Adverse events side effects associated with cancer immunotherapy. Adapted with permission from Wakabayashi G, Lee Y-C, Luh F et al. Development and clinical applications of cancer immunotherapy against PD-1 signaling pathway. Journal of Biomedical Science 2019;26:96 under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0).
Multimodality treatment
Increasing numbers of patients are offered multimodality treatment. Adjuvant postoperative chemotherapy is offered to patients with completely resected stage II and III lung cancer and a good performance status. NICE recommends considering the use of combination chemoradiotherapy followed by surgery for a small sub-set of suitable patients with operable stage IIIA disease. Patients with stage II or III NSCLC for whom surgery isn't suitable or who decline surgery should be offered combined chemoradiotherapy if they are fit enough. This may be followed by durvalumab monotherapy within the Cancer Drugs Fund for those who meet a strict list of eligibility criteria, as this has been shown in trials to improve progression-free and overall survival.
Small-cell lung cancer
Around 10% of lung cancers are SCLC. This is a more aggressive disease than NSCLC and patients often present at an advanced stage. Patients with very early disease (tumours < 3 cm and no nodal spread) may be considered for surgery followed by adjuvant chemotherapy. Those with good performance status and disease that could be encompassed within a radiotherapy field may be offered chemoradiotherapy. In patients with extensive disease, the priority is to commence chemotherapy as soon as possible. The response to chemotherapy is often good but, unfortunately, long-term outcomes remain very poor as early relapse is usual. The recommendation is that all patients with SCLC should be seen by an oncologist within 1 week of the decision to commence treatment.
Enhanced supportive care
All patients with advanced lung cancer should be offered enhanced supportive care input. Enhanced supportive care involves the prevention and management of adverse events from cancer and its treatment. Early involvement of the palliative care team not only improves quality of life, but has been shown to have a survival benefit of up to 2 months.15
Smoking cessation
All patients who are current smokers should be offered smoking cessation support. It is of particular significance in those undergoing treatment with curative intent, as it reduces the risk of post-operative and systemic treatment-related complications and, in addition, reduces the chance of cancer recurrence.16,17
Conclusion
While lung cancer survival remains poor, improved access to standardised diagnostic tests, along with advancements in treatment options, are beginning to show encouraging trends for the better and provide us with hope for improved outcomes in the future. Recognition and management of lung cancer and, particularly, its acute presentations continues to be important for those practising in primary and secondary care who should maintain a high index of suspicion for the disease. With the continuing and significant advancements in lung cancer treatment, early referral for appropriate diagnostic workup is essential. The ‘diagnostic standards of care’ should be adhered to routinely so that best practice is always implemented, variation between centres is reduced and patient progression through diagnostics, staging and management is as rapid as possible.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.