
ABSTRACT
Objectives Reactive axillary lymph nodes (ALN) may occur post-COVID-19 vaccination. This may be confused with malignant nodal metastases on oncological imaging. We aimed to determine the reactive ALN incidence and duration on 18F-fluorodeoxyglucose positron emission tomography – computed tomography (18F-FDG PET-CT), and its relationship with gender, age and vaccine type.
Methods A retrospective study was performed. Two-hundred and four eligible patients had 18F-FDG PET-CT between 01 January 2021 and 31 March 2021, post-vaccination with Pfizer-BioNTech or Oxford-AstraZeneca vaccine. Image analysis was performed on dedicated workstations. SPSS was used for statistical analysis.
Results Thirty-six per cent of patients had reactive ALN until 10 weeks post-vaccination; reducing in frequency and intensity with time. Women were more likely to have reactive ALN compared with men. The frequency and intensity were higher in patients aged <65 years compared with those aged ≥65 years. However, no difference was found between both vaccine types in our study cohort.
Conclusions Physicians’ awareness of COVID-19 vaccine-related reactive ALN on 18F-FDG PET-CT is important to avoid inappropriate upstaging of cancers.
Introduction
The COVID-19 pandemic has rapidly spread around the world causing devastating effects to millions of people. While this situation is still ongoing, the resilience of the global society is constantly being challenged. In response to the pandemic, unprecedented investments have been made in vaccine development.
The UK had the international lead in rolling out the COVID-19 mass vaccination programme on 08 December 2020.1 The Medicines and Healthcare products Regulatory Agency gave regulatory approval for the Pfizer-BioNTech vaccine in the UK on 02 December 2020, followed by the Oxford-AstraZeneca vaccine on 30 December 2020.2,3
Like all vaccines, COVID-19 vaccines carry a potential to cause side effects, of which, the most common being local inflammation at the injection site. Local enlarged lymphadenopathy can also occur, however, this is reported as being uncommon at <1 in 100 administrations.2,3
There is emerging data that describe the effect of COVID-19 vaccine on the 18F-fluorodeoxyglucose positron emission tomography – computed tomography (18F-FDG PET-CT) imaging appearances. This modality uses a glucose analogue to image metabolic activities of various pathologies, predominately tumours, but also inflammation and infection. A number of published case reports illustrate increased 18F-FDG uptake in ipsilateral axillary lymph nodes (ALN) after administration of COVID-19 vaccines in the deltoid muscle.4–7 However, paucity of data means that the incidence and expected duration of uptake is not well established, particularly with different vaccine types.
The appearance of the reactive ALN may be confused with malignant nodal metastases on oncological imaging. Therefore, establishing accurate data regarding the vaccine effect is of extreme importance to avoid inappropriate management of patients with cancer.
We performed a study documenting the effect of the COVID-19 vaccine on the incidence of reactive axillary lymphadenopathy on 18F-FDG PET-CT at different time points post-vaccination with two different vaccine types.
Materials and methods
Study sample and data collection
The study was performed at a major tertiary hospital. It was approved by the institutional COVID-19 research committee and research and development department. The need for written informed consent was waived due to the retrospective and observational nature of the study.
Eligible subjects were patients who had an 18F-FDG PET-CT at our institution after receiving their COVID-19 vaccination. PET-CT were performed as part of the routine clinical care with a range of indications falling within the Royal College of Radiologists’ guidelines.8 Our nuclear medicine department started routinely documenting the details of the vaccination at the beginning of January 2021 to aid clinical interpretation of the PET-CT. Therefore, data were collected from 01 January 2021 until 31 March 2021.
Exclusion criteria were inadequate vaccination information, and patients with ALN pathologies or with conditions impairing the interpretation of ALN findings (Table 1).
Detailed exclusion criteria
COVID-19 vaccine
All patients in this study received either the Pfizer-BioNTech or the Oxford-AstraZeneca vaccine. On 30 December 2020, the UK declared a deviation from the recommended vaccination schedule for the Pfizer-BioNTech vaccine, prolonging the interval between doses from 3 to 12 weeks. The same decision was made for the Oxford-AstraZeneca vaccine, for which a longer gap between doses had been shown to improve efficacy in some age groups.9
The main priority for the vaccination programme was to prevent mortalities and maintain the health and social care systems. Therefore, the UK Joint Committee on Vaccination and Immunisation (JCVI) recommended to offer the vaccine based on priority groups (supplementary material S1).10
Imaging method
All scans were acquired on a GE Healthcare 64-slice Discovery PET/CT 710 (GE Healthcare, Chicago, USA). The same protocol was followed for all patients, which included fasting for 6 hours prior to injection of 4 MBq/Kg 18F-FDG (±10%). The target fasting blood glucose was between 4.0 and 8.3 mmol/L. The departmental protocol suggests an uptake period of at least 50 minutes, but the uptake period was not recorded in the study data. PET were acquired at 3 minutes / bed position.
Data collection
Variables collected from the patient electronic records were the patients’ demographics (gender and age), vaccination details (1st vs 2nd dose, type and site) and primary indication of the PET-CT. The maximum standardised uptake value (SUVmax) and size of ALN (ipsilateral and contralateral to vaccination site) were collected using an Advantage Workstation version 4.6 with 3D volume viewer software 11.3 (GE Healthcare, Chicago, USA). This provides an automatically delineated volume of interest (VOI) using an isocontour threshold method based on SUV. A VOI was drawn over the most avid ipsilateral ALN and over a representative contralateral ALN to obtain SUVmax values. The size of the ALN on both sides were measured on CT and recorded as either non-enlarged if <1 cm or enlarged if >1 cm.
Statistical analysis
Normally distributed continuous variables are presented as mean ± standard deviation (SD). Categorical variables are presented as numbers and percentages.
Student's t-test was used for the normally distributed continuous variables. The chi-squared test was used for categorical variables. Statistical significance was defined as p<0.05.
The contralateral ALN SUVmax was used to control for background activity by subtracting it from the ipsilateral ALN SUVmax. This gave the difference in SUVmax (dSUV) between ipsilateral and contralateral ALN. One SD of the contralateral ALN mean SUVmax was used as a cut-off for considering dSUV as positive for reactive lymphadenopathy.
Statistical analysis was performed using IBM SPSS, version 26 (IBM, Armonk, USA).
Results
A total of 319 patients had 18F-FDG PET-CT after receiving their COVID-19 vaccination. After excluding 115 patients who did not meet the study's eligibility criteria, a total of 204 patients were included in the study (Fig 1). The characteristics of the study population are summarised in supplementary material S2.

Included and excluded patients.18F-FDG PET-CT = 18F-fluorodeoxyglucose positron emission tomography – computed tomography; ALN = axillary lymph nodes.
Avidity in ipsilateral vs contralateral ALN
The mean SUVmax in the ipsilateral ALN (1.9 g/mL; SD 1.7) was higher than in the contralateral ALN (1.1 g/mL; SD 0.7; p<0.001). Using the latter SD, the cut-off for positive reactive ALN was determined to be dSUV >0.7 g/mL.
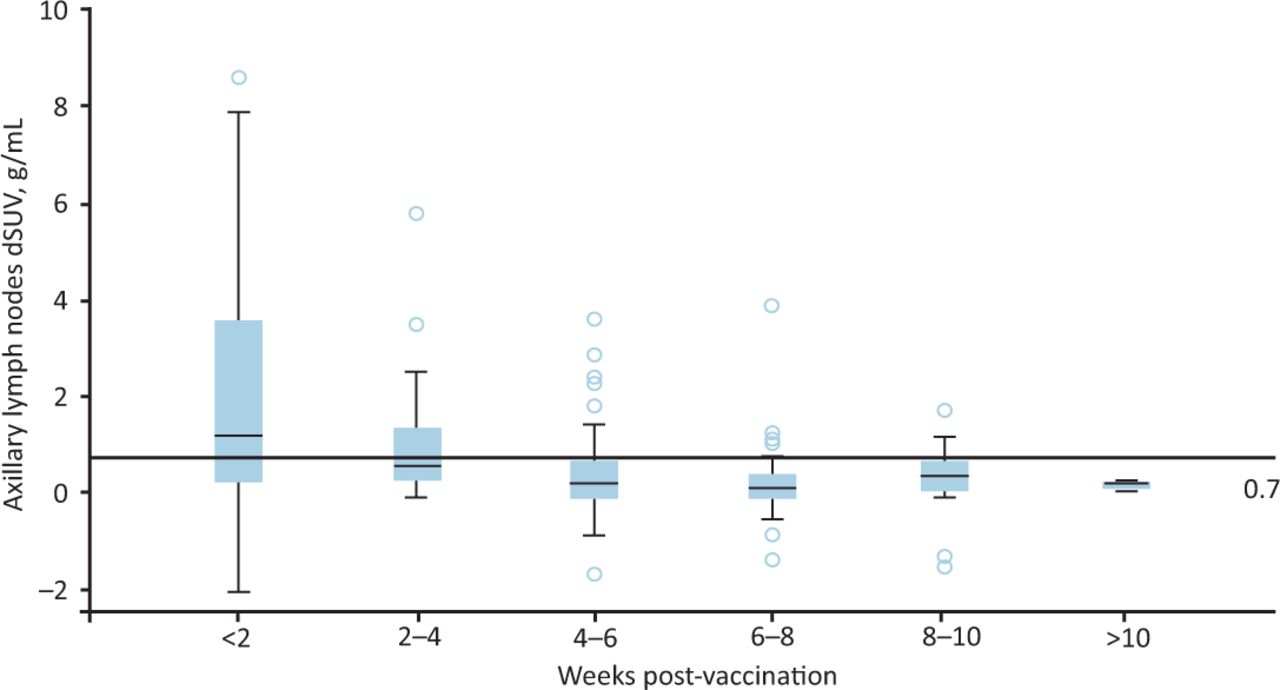
Seventy-four out of 204 patients (36%) had avid ipsilateral ALN which was seen up to 10-weeks post-vaccination (Fig 2), however, reducing in frequency and intensity with time. No positive ALN was seen after 10-weeks post-vaccination (Fig 3; Table 2). None of the avid lymph nodes in our study sample was enlarged by size criteria.
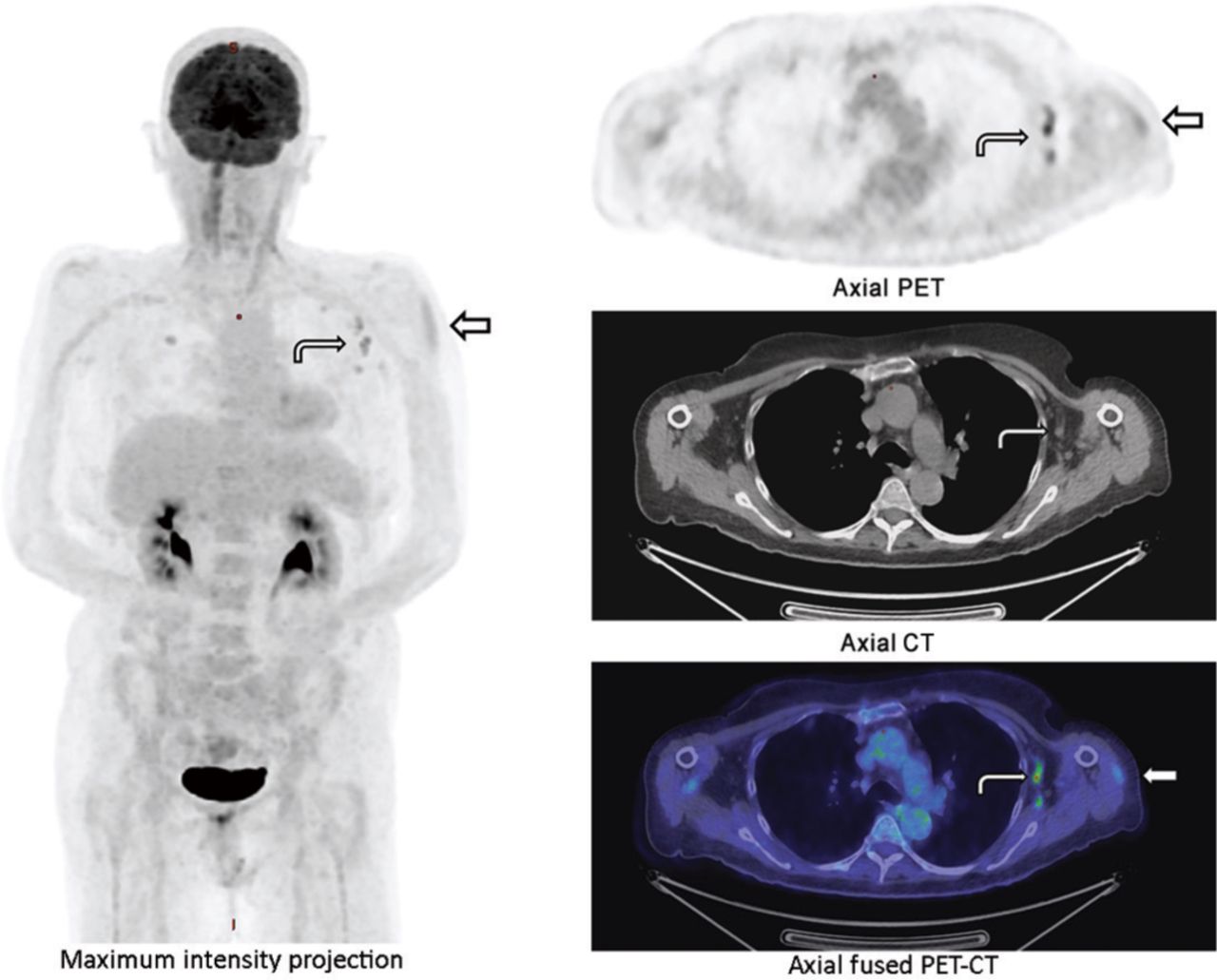
Typical appearance of reactive axillary lymph nodes post-COVID-19 vaccination in one of the study patients. Straight arrow = injection site inflammation in left deltoid muscle (not necessarily seen in all cases); curved arrow = reactive ipsilateral axillary lymph nodes; CT = computed tomography; PET = positron emission tomography.
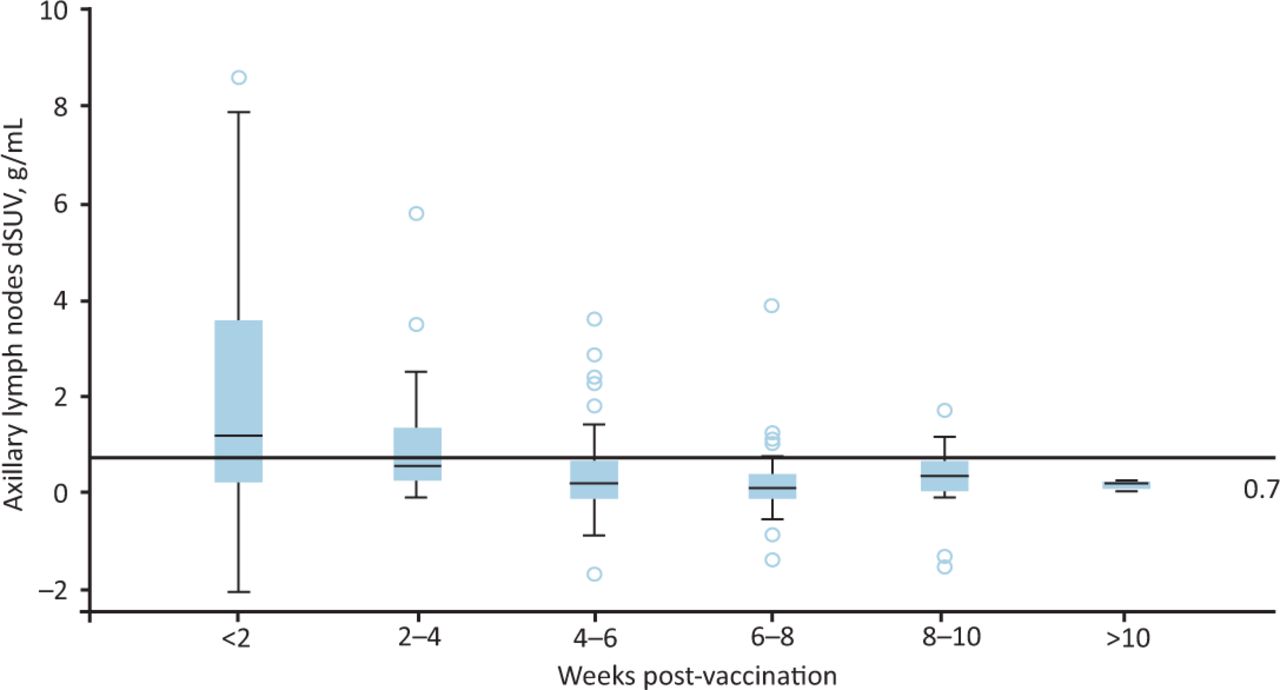
Relation between axillary lymph nodes dSUV and post-vaccination duration (above the 0.7 line indicates avidity).
Total patients with avid ipsilateral axillary lymph nodes post-vaccination
Gender
Within 6 weeks of vaccination, the mean dSUV was higher in women (1.3 g/mL; SD 1.8) compared with men (0.9 g/mL; SD 1.7). This did not achieve statistical significance (p=0.26). However, there was a statistically significant higher percentage of women who had positive reactive ALN compared with men (p=0.04; Table 3).
Subgroup analysis of patients with avid ipsilateral axillary lymph nodes post-vaccination
Age
Within 6 weeks of vaccination, the mean dSUV in patients aged <65 years (1.6 g/mL; SD 2) was higher than in patients aged ≥65 years (0.8 g/mL; SD 1.6; p=0.021). Moreover, a higher percentage of patients aged <65 years had positive reactive ALN compared with those aged ≥65 years (p=0.03; Table 3). All these differences were statistically significant.
Vaccine type
The vaccine type was available for 105/204 (51%) patients: 62/105 (59%) had the Pfizer-BioNTech vaccine and 43/105 (41%) had the Oxford-AstraZeneca vaccine. Within 6 weeks of vaccination, patients who received the Oxford-AstraZeneca vaccine showed higher mean dSUV in the ipsilateral ALN (1.1 g/mL; SD 1.5) than those who received the Pfizer-BioNTech vaccine (0.8 g/mL; SD 1.7; p=0.43). Similarly, a higher percentage of the patients who received the Oxford-AstraZeneca vaccine showed positive ALN compared with those who received the Pfizer-BioNTech vaccine (p=0.08; Table 3). None of these differences reached statistical significance.
Discussion
This study assessed the incidence of 18F-FDG uptake at various time points following one of two different COVID-19 vaccine types: an mRNA vaccine or an adenoviral vector vaccine. The cohort includes patients at varying times post-vaccination; with several who had vaccination >10 weeks prior to their PET-CT. The data show that reactive 18F-FDG avidity is seen in the ALN ipsilateral to the vaccinated arm in the majority of patients within the first 2 weeks post-vaccination, with a gradual reduction in the intensity of avidity and number of patients showing this effect over a 10-week period. We strictly excluded patients with pathology that might involve the ALN to avoid false positive cases.
Several case reports have already described reactive 18F-FDG uptake in ALN ipsilateral to the vaccinated arm secondary to local inflammation and immune response.4–7 This has been a well-recognised process with other vaccinations prior to the COVID-19 pandemic.11–13 However, given the nature of the mass vaccination in COVID-19, this feature is now seen routinely in clinical practice and may impair the clinical interpretation of 18F-FDG PET-CT. Prior to the COVID-19 pandemic, the published evidence described vaccine-related 18F-FDG uptake in ipsilateral ALN up to 2 weeks post-vaccination for influenza.11–13 However, the evolving evidence demonstrates that the duration is longer with COVID-19 vaccine. McIntosh et al observed 18F-FDG uptake in ipsilateral ALN 4–6 weeks post-vaccination.7 Our study shows that avidity in the ipsilateral ALN can be seen up to 10 weeks post-vaccination.
None of the patients in our study population had size enlarged ALN >1 cm. This is compatible with the current available data listing palpable lymphadenopathy as an uncommon side effect of the COVID-19 vaccine.2,3 Therefore, we suggest regarding enlarged local lymph nodes as suspicious until proven otherwise. These could be investigated further with follow-up imaging or ultrasound-guided biopsy if this would impact on patient management.
Gee et al reported that COVID-19 vaccine side effects occurred more in women compared with men (78.7% vs 20.1%, remainder of unknown gender), and in people aged <65 years compared with those aged ≥65 years (90.4% vs 6.2%, remainder of unknown age).14 Our data are in line with this as it shows that avid ALN occurred with more frequency and intensity in those two groups of patients. This could be due to sex hormone mediation of immune response, as Potluri et al showed higher immune responses to influenza vaccination in women due to oestradiol. The beneficial effect of the raised oestradiol on immune response in women was reduced with age in that study.15
Each of the Pfizer-BioNTech and the Oxford-AstraZeneca vaccines use different technology. The Pfizer-BioNTech vaccine uses an mRNA platform whereas the Oxford-AstraZeneca vaccine uses an adenovirus vector.2,3 Despite this difference, our data did not show a significant difference in vaccine-related 18F-FDG avidity between both vaccine types.
18F-FDG PET-CT appearances after COVID-19 vaccination are important to recognise to avoid inappropriate upstaging of cancer cases. This also has to be taken into consideration when these cases are presented at the various multidisciplinary team meetings (MDMs).
Moreover, there are reports in the literature describing post-COVID-19 vaccine reactive ALN uptake in patients having PET-CT with non-FDG tracers; including 68Ga-DOTATATE, 18F-fluciclovine and 11C-choline. These are mainly case reports and, in the case of 11C-choline, a small study of 13 patients.16–19 Awareness of this is also important and further research is required to establish the incidence and duration of this reactive uptake in large patient cohorts.
Given the importance of information obtained from imaging, we recommend that both the patients and vaccine clinics are educated about the importance of avoiding the vaccine in the arm ipsilateral to the tumour drainage site. Administration of the vaccine to the vastus lateralis of the thigh is an alternative route within the Public Health England and Centers for Disease Control and Prevention guidelines, although drainage into the inguinal and pelvic nodal groups could potentially cause similar reactive avidity.20,21 Another option is to schedule 18F-FDG PET-CT with a 6 week delay after vaccination, although this would depend on the clinical urgency of the test. Our data suggest that, in patients who had vaccination more than 6 weeks before PET-CT, up to 14.5% only would have reactive avidity in the ALN ipsilateral to the vaccination site.
The majority of the patients in our study had their scan after the 1st vaccine dose. Perhaps, this is because the UK has recommended a 12-week gap between both vaccination doses.9 Therefore, a mass population receiving the 2nd vaccination dose was not seen in the study period. Further studies would be required to establish the duration of avidity after the 2nd dose as the side effects are reported to be more intense for some vaccine types.22 Dedicated studies based on the vaccine type and duration between the two doses would be needed as there may be a difference based on these factors.
The main limitation of our study was the retrospective nature and absence of data on confounding factors that may affect 18F-FDG uptake; for example, data on recent chemotherapy was not collected. As the majority of patients in the cohort had a known malignancy, there may be a significant proportion who have had recent chemotherapy that could reduce the immune response. However, in our standard clinical practice, 18F-FDG PET-CT is scheduled with a gap of at least 14 days since the latest chemotherapy to minimise such effect. Furthermore, the cohort is representative of patients having 18F-FDG PET-CT under the UK guidelines only.
Another limitation of the study was that patients were vaccinated in stages according to the UK JCVI priority groups. With exception to health and social care workers and those living in care homes, the initial prioritisation was based on older age groups. However, the study still included a wide age range, as the fourth priority group included ‘clinical extremely vulnerable patients’ regardless of the age; this group encompasses many patients referred for PET-CT, such as patients with cancer on chemotherapy.
Finally, the COVID-19 vaccine type was available in only 51% of the study subjects, which has led to a relatively small patient cohort with known vaccine type. Therefore, despite no significant difference found in our study between both vaccine types in the vaccine-related 18F-FDG avidity, further research is needed to support this finding.
Conclusion
This study shows that COVID-19 vaccines can cause reactive avidity in the ALN ipsilateral to the vaccination site on 18F-FDG PET-CT within the first 6 weeks post-vaccination; this may persist for up to 10 weeks. Women and those aged <65 years are more likely to have this effect. This should be accounted for not only by the PET reporting radiologists but also by all the clinical teams reviewing these scans at the various MDMs. This is crucial to avoid inappropriate upstaging of cancer cases.
Summary
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – COVID-19 vaccine priority groups based on UK Joint Committee on Vaccination and Immunisation recommendations.
S2 – Baseline characteristics of the patients included in the study.
Acknowledgements
We would like to acknowledge the support of the University Hospitals Coventry and Warwickshire COVID-19 Vaccine Action Centre.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
{kind=link}