
ABSTRACT
The Royal College of Physicians’ COVID-19 study was conducted in 2020 as a collaboration of 19 English NHS trusts, the Association of Professional Healthcare Analysts and a data team in the Institute of Global Health Innovation at Imperial College London. The participating trusts had a combined catchment population of 10.46 million and looked after over 26,000 patients with SARS-CoV-2. The study involved 510 patient cases the majority of which were mortality reviews. The data were analysed both quantitatively and qualitatively and employed novel natural language processing methods. The quantitative data established that 96.5% of the care delivered was adequate, good or excellent. Poor care was uncommon. Qualitative data generated 24 common themes that were articulated by the creation of nine vignettes (four explored here). Six recommendations were created, and further analysis of specific recommendations is advised.
Introduction
A SARS-CoV-2 (COVID-19) pandemic was declared by the World Health Organization on 11 March 2020. One year later, 117 million people had been infected and approximately 2.6 million people had died from the disease. On the first anniversary of the declaration of the pandemic, over six and a half billion articles had been written about many aspects of the condition and its global effects. However, there have been limited reports of the systematic analysis of healthcare quality during the pandemic.
The Royal College of Physicians (RCP) invited NHS trusts to participate in this study in 2020, 40 trusts expressed an interest, and 19 English NHS trusts agreed to share non-identifiable patient reports of those who were treated in hospital with confirmed COVID-19. The study created thematic analysis, combined with a natural language processing technique. Vignettes, describing patient care, were constructed to articulate themes.
The quantitative elements of the study describe the demographic data, the analysis of scores given to care across the whole sample of patients and the associated subgroups.
Methodology
All the centres used a structured judgement review (SJR) methodology in the construction of their reports and, in addition, collectively supplied 241 individual anonymised reports, which were subject to further analysis. The majority of the patients in this study did not survive the illness, as sites were predominantly using SJR for mortality reviews. While this was a bias in the study, this does not reflect the survival experience of those hospitalised with COVID-19 in the pandemic.
The participating centres were asked to return standardised data, in the form of modified SJR (mSJR), and describe themes that emerged from the cases that they reviewed.
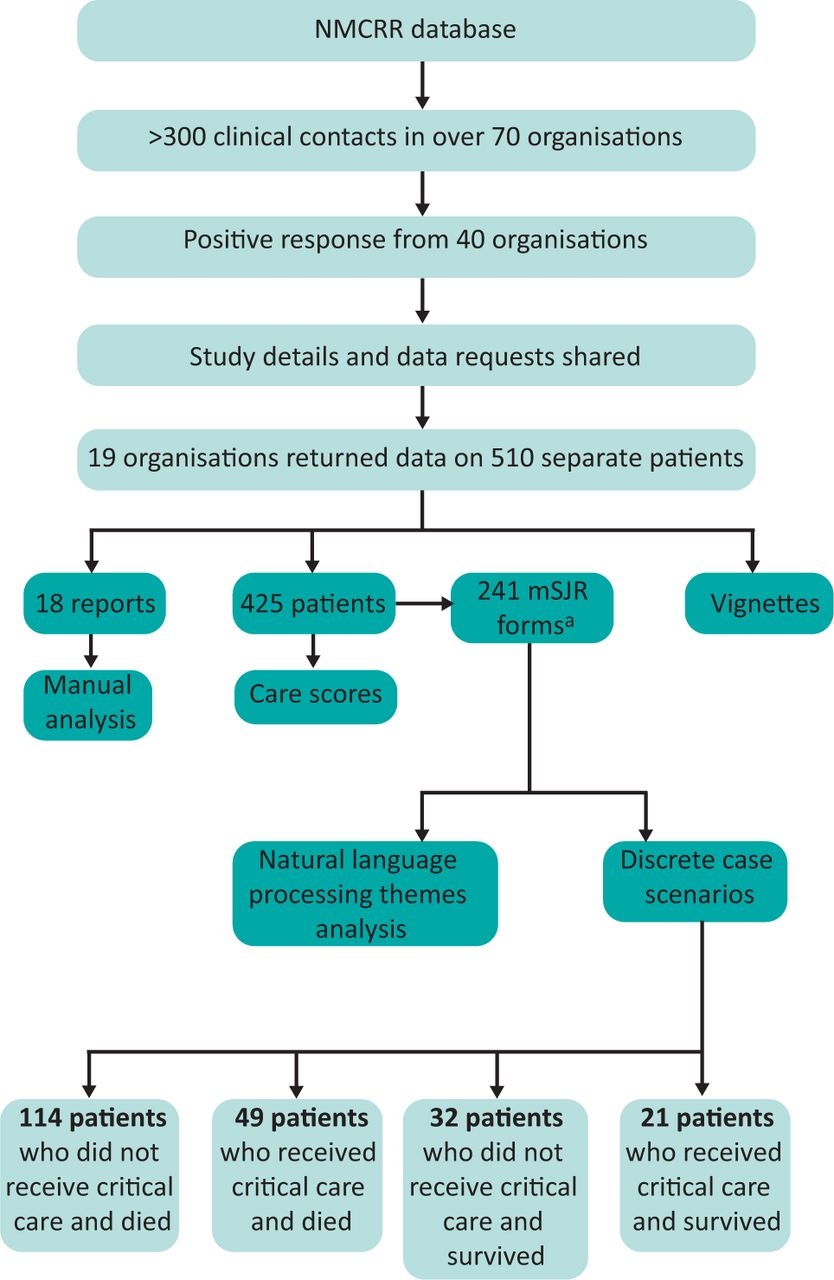
This overall process is visualised in Fig 1. It included a novel approach to analysis with natural language processing. The Latent Dirichlet Allocation (LDA) methodology was used to identify statistically different topics emerging from the analysis of the subgroups identified.
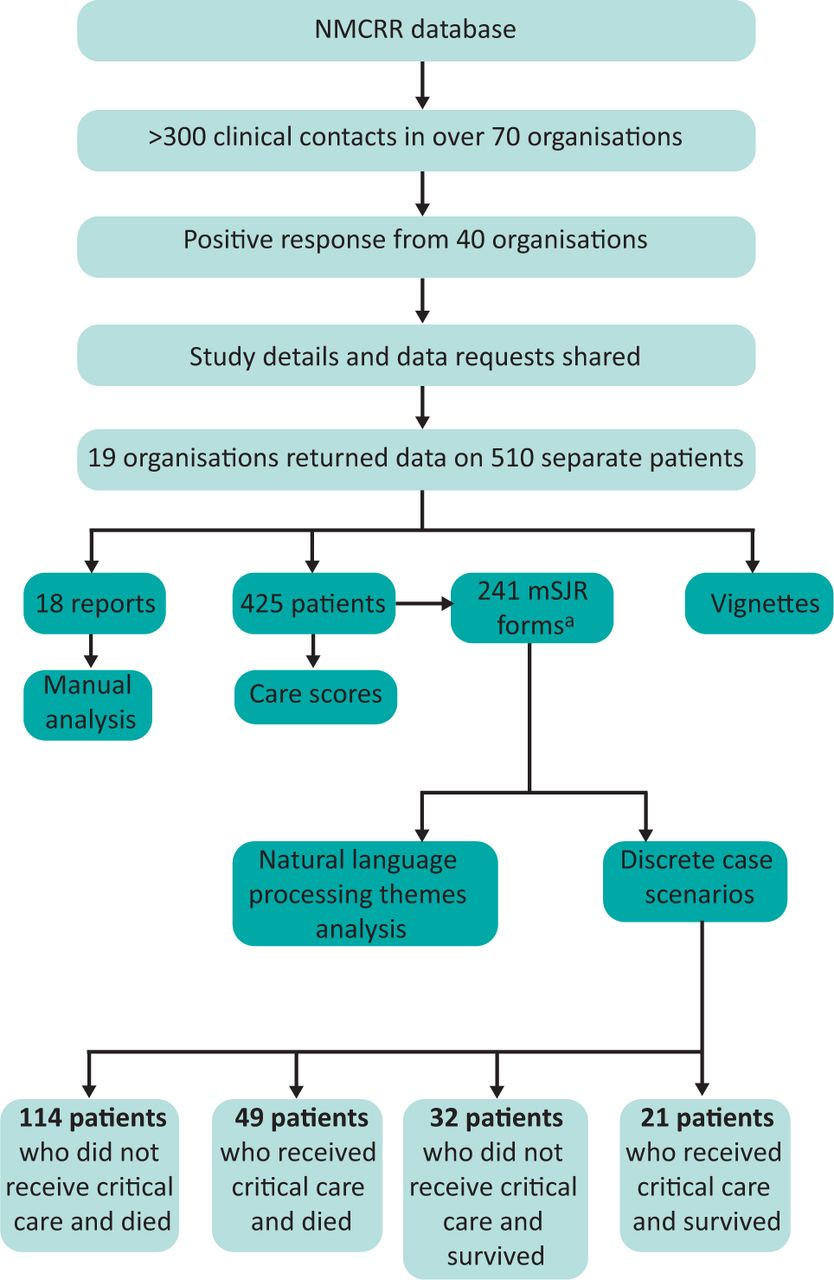
Overview of the study. aThis is a subset of the 425 patient cases, 216 cases were subject to analysis; NMCRR = National Mortality Case Record Review; mSJR = modified structured judgement review.
Results
Demographics
All seven health regions in England were represented (described in Box 1), while the demographic data of the study sample is in Table 1.
Total catchment population, numbers of deaths and the proportions of survivors in participating centres, n=19
NHS regions, cities and towns represented
The catchment population of the study of 10.46 million equates to approximately 19% of the population of England, which in 2019 was estimated by the Office for National Statistics as 56.23 million.
The number of hospital deaths from COVID-19 in the centres was a minimum of 6,389, which accounts for approximately one in seven acute hospital deaths from COVID-19 in 2020.
There is a range of 12% to 35% of the crude COVID-19 mortality between the 19 centres with a median of 24%. This variation is likely to be multi-factorial.
Only 18 of 510 cases (3.5%) had an overall care score of poor. None of the cases where care was scored poorly affected the outcomes for the patients. The commonest causes of poor care are described in Box 2.
Commonest causes of an overall care score of poor, n=18
Thematic analysis
Themes generated are in Table 2 and a commentary of the theme's description was created by analysing each comment in detail and ascribing a positive or negative sentiment to the theme.
Themes, with number of centres giving positive and negative comments
It is important to recognise that the negative commentary usually meant ‘what could have been improved’ but was not synonymous with ‘poor care’. Table 2 lists these themes together with the frequency of positive or negative comments made by the centres.
As can be seen, some themes attracted both positive and negative comments implying significant variability of care quality related to that theme. In addition, some themes were mostly positive and some themes almost wholly negative.
Care scores
The care scores within each report were generated for each individual phase of care by a trained reviewer. The 425 patient cases that allowed for detailed analysis are shown in Table 3.
Phases of care scores for admission, ongoing, end-of-life care / discharge and overall care
A subset of 216 case reviews allowed comparison of the care quality scores across four scenarios: whether the patient had received critical care or not, and whether they had survived or died. The patient characteristics of these four groups was also analysed. The care scores for these subgroups are in Table 4.
The analysis of the four subgroups
Table 4 shows that the quality of admission care across the four subgroups was of an adequate, good or excellent standard in 99% of the patients admitted, with only two cases not in this category. This suggests that despite the operational pressures, emergency departments were still able to provide high-quality care to patients with COVID-19.
In contrast to the admission phase of care, reviewers had concerns about the end-of-life care (EOLC) in those patients who died without admission to critical care, and this was different to the judgements of EOLC in a critical care setting. The proportion of the excellent care received in the ward setting was over 30%, which supports the hypothesis that there is a clear inconsistency or variability in the delivery of EOLC in this study.
This subgroup analysis demonstrates that there was no care judged to be poor or very poor in the 70 patients who were admitted to critical care and either survived (n=21) or died (n=49). The provision of critical care was always of an adequate standard or above. For the most part, the overall care was deemed good or excellent with only one case out of 70 scored as adequate (1.5%).
Vignettes
The common themes have been incorporated into several case vignettes (Vignettes 1–4). The vignettes reflect the outcomes described for all patient groups. A picture of the typical care received by the patients in this study is described in Vignette 1. It includes many of the recurring positive aspects of care experienced by patients during the COVID-19 pandemic in 2020.
Typical ward care received
Poor communication
Compassion in end-of-life care delivery
Documenting decisions, delays and escalation
Vignettes 2–4 illustrate other key themes commonly described by the participating centres. The themes highlighted here involve:
EOLC management
communication and documentation
compassion
delays
escalation decisions and documentation
critical care experience
learning disability.
Conclusion
From our detailed analysis we can conclude the following.
This study presents the quality of care delivered from a large sample of patients with COVID-19 treated in representative NHS hospitals in England during the COVID-19 pandemic in 2020.
The care delivered to patients with COVID-19 was of a high standard. It is depicted in a series of vignettes drawn from shared case studies and adapted to include common issues identified in the thematic analysis.
Learning from the review of good and excellent care, which was much more common, is equally valid to the learning derived from poor care.
There was no evidence for differential quality of care delivery between any of the four subgroups but those patients who died and were not escalated to critical care had poorer care scores across the phases of care. This may be due to a combination of hindsight bias and the absence of negative factors in the survivors who did not, for example, experience poor EOLC.
Care judged to be poor overall was uncommon. When it did occur, it was related to EOLC issues, nosocomial infections, delays in assessment, escalation, and issues of poor communication and poor documentation.
The experience of patients with a known learning disability appears to be different in respect of the rationale for escalation decisions. It is possible that the quality of their EOLC experience was different. Due to low case numbers, however, this finding should be treated with some caution. There were, however, clear examples where the reviewers were uncertain of the documentation and reasoning for important care decisions.
In the context of adequate, good and excellent care, many trusts described a lack of consistency for important aspects of care delivery to patients including:
EOLC experiences
assessment in emergency departments
documentation and communication
senior review
do not attempt cardiopulmonary resuscitation decisions
discharge planning.
A multidisciplinary approach and the importance of palliative care were uniformly celebrated and key to the successful delivery of high-quality care.
Care of patients with nosocomial infections was studied in 11 trusts. These patients accounted for approximately 8% of the mortality reviews in this study. All but one of the trusts described hospital-acquired infections as negative aspects of care, and many centres had already established investigations into the causes of these infections.
There was a variation between centres of crude mortality due to COVID-19 from approximately one in 10 cases to approximately one in three cases. Further analysis is required to explain these differences.
Using a natural language processing algorithm, as an emerging qualitative technique, provided additional supporting analysis to the study. This use of natural language processing will be subject to further research by Imperial College London.
Recommendations
Hospitals and teams that have delivered excellent care during the pandemic should analyse the factors that have enabled this to happen. They could share the learning from the key findings, locally or nationally, to support more consistent quality of care in the future and to raise awareness across the NHS and with the general public.
Healthcare professionals and organisations should strive to reduce the variation in care in key areas including:
EOLC in hospital
early assessment in acute care presentations
documentation and communication
senior review and decision making
treatment escalation planning, conversations and documentation
discharge planning
particular focus should be given to reducing variation for those with learning disabilities in these areas.
The guidance and standards published by the RCP covering many of these areas should be implemented and followed more consistently.
All NHS organisations are encouraged to pay particular attention to the quality of care, decision making, communication and documentation that is required for vulnerable people, including those with learning disabilities.
The NHS should further explore the reasons for the range of hospital mortality between areas during the COVID-19 pandemic.
The RCP and Imperial College London will further explore the role of natural language processing in the qualitative analysis of structured case record reviews.
Full report
The full report can be accessed on the RCP website:
www.rcp.ac.uk/projects/outputs/caring-hospital-patients-covid-19
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.