
Introduction
It has been established that COVID-19 viral pneumonitis is associated with chest X-ray (CXR) changes, predominantly peripheral and basal patchy ground glass opacities.1 However, what was less clear was what to expect after recovery from acute illness and the subsequent resolution which made follow-up pathways more difficult to establish. In severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome coronavirus (MERS-CoV) 65% in radiological follow-up demonstrate complete CXR resolution at a median of 43 days.2,3 There were also variable numbers of radiological and clinical features of pulmonary fibrosis up to 60% but overall case numbers were small.2,3 We aimed to establish the proportion of CXR resolution following discharge in patients with COVID-19 pneumonitis and use this information to guide CXR timing in follow up.
Materials and methods
British Thoracic Society (BTS) guidelines for COVID-19 follow up formed the basis of local guidelines. BTS advised follow up for COVID-19 pneumonitis patients with CXR changes based on stratification into two groups; severe and moderate. The severe group included patients managed in ICU or HDU, who had protracted continued positive pressure ventilation, bi-level non-invasive ventilation or high fractions of inspired oxygen, or with new home oxygen.4 BTS advised follow-up at 4–6 weeks for severe cases with a face-to-face review within 12 weeks, while for moderate cases a virtual follow-up within 12 weeks was advised. Both groups were advised to have a CXR within 12 weeks.4 Local approach followed this, with the exception of bringing forward CXR for severe patients to 6 weeks. We analysed all follow-up appointments in order to establish CXR resolution and the presence of ongoing symptoms. We also reviewed the local Picture Archiving and Communication System to establish actual timing between abnormal to follow-up CXR.
Results and discussion
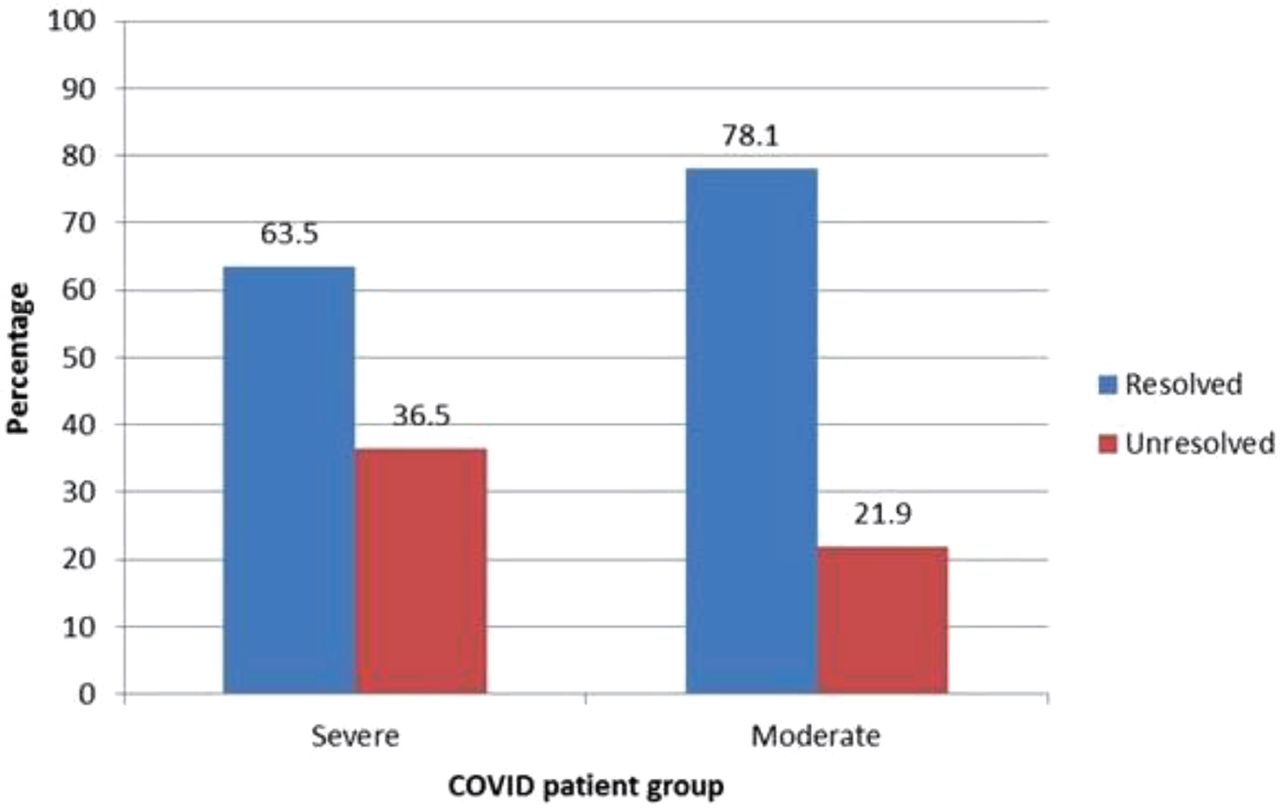
We had 63 patients with severe COVID-19 and 41 patients with moderate COVID-19. We found that in the severe group 63.5% had resolved CXR compared with 78.1% in the moderate group (Fig 1). While the severe group were followed up at 6 weeks and the moderate group at 12 weeks, we found that due to the prolonged admissions of the severe group, the CXR timing was similar; 62 days on median for the severe, and 66 for the moderate, making them comparable in terms of timing.

Resolved and unresolved chest X-ray on follow-up in severe and moderate cases of COVID-19.
We also found that in the severe group, those with resolved CXR were 65.9% asymptomatic and 24.4% symptomatic, those with unresolved CXR were 4.5% asymptomatic and 72.7% symptomatic. In the moderate group, those with resolved CXR were 75.0% asymptomatic and 25.0% symptomatic, and those with unresolved CXR were 33.3% asymptomatic and 66.7% symptomatic.
Conclusion
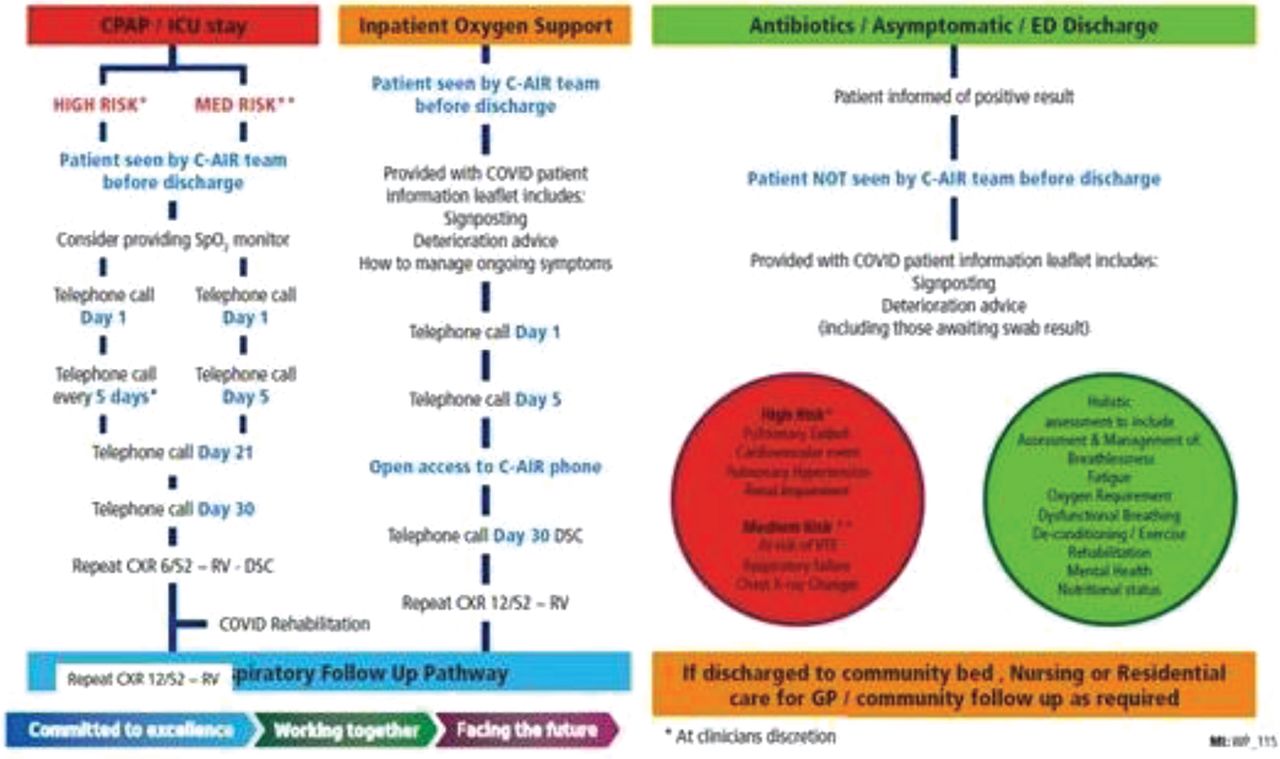
We concluded that follow-up CXR at 10 weeks should be recommended for both moderate and severe COVID-19 cases as resolution was over 70%. We hope this will reduce the number of unnecessary CXR while allowing poor resolution to be identified in a timely manner. We now offer both severe and moderate groups 10-week follow-up with a CXR, and COVID-19 Adult Integrated Respiratory (C-AIR) team follow up immediately following discharge (Fig 2).

Supportive discharge pathway for patients admitted as COVID-19 positive.
Conflicts of interest
None declared.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.