
Introduction
Continuous positive airway pressure (CPAP) therapy had been previously shown to reduce the need for invasive mechanical ventilation (IMV) in cardiogenic pulmonary oedema, but evidence of its efficacy in viral-induced respiratory failure is limited and is a subject of debate.1,2 An early intubation strategy without trial of non-invasive ventilation (NIV) had been previously suggested, while others have argued for timely, but not premature, intubation.3 We retrospectively evaluated the efficacy of CPAP in patients with COVID-19 at a single centre.
Methods
We reviewed notes of consecutive patients between 21 March and 23 April 2020. Inclusion criteria were laboratory-confirmed diagnosis of SARS-CoV-2 and CPAP therapy. Exclusion criteria were <16 years old, pregnancy, acute-on-chronic hypercapnic respiratory failure and acute respiratory failure from an alternative diagnosis to SARS-CoV-2. Patient characteristics, laboratory results, rates of intubation and mortality were recorded.
Unpaired parametric and non-parametric data were compared with an unpaired two-sample t test or Mann–Whitney test, respectively. Fisher's exact test was used for categorical variables. All statistical tests were two-tailed. Analyses were performed with GraphPad Prism 8.4.2 (GraphPad Software, San Diego, USA).
Results and discussion
Sixty patients received CPAP during the study period; 52 met study criteria. Mean age was 61.4 (±14.1) years, 17 (33%) were females, 14 (27%) non-White Caucasians, median body mass index (BMI) 27.7 kg/m2 (interquartile range (IQR) 23.8–32.2 kg/m2) and frailty scale 2 (1–3). Before CPAP, 46 (89%) patients required FiO2 ≥0.60 to maintain target oxygenation and the remaining patients were commenced on CPAP due to respiratory rates >35 breaths/min despite FiO2 ≥0.35.
Thirty-eight patients received CPAP as a trial to avoid IMV; 21 (55%) eventually required IMV after 38 (21–67) hours, while 17 (45%) avoided IMV after 108 (71–209) hours. Patients requiring a non-rebreather oxygen mask pre-CPAP were unlikely to avoid intubation; seven of nine (78%) failed trial of CPAP. Patients who avoided intubation (PCPAP) had a significantly higher pre-CPAP PaO2/FiO2 and lower lactate dehydrogenase (LDH) than those who required IMV (PIMV) (Table 1, Fig 1). PaO2/FiO2 on PEEP (positive end-expiratory pressure) ≥5 cm H2O in PCPAP was higher than PIMV: median PaO2/FiO2 120.0 (104.0–228.8) vs 85.0 (80.2–92.0) mmHg, p=0.024.
SARS-CoV-2 patients receiving CPAP as a trial to avoid invasive mechanical ventilation. Comparing clinical and laboratory characteristics between patients who avoided IMV (PCPAP) and patients who required IMV (PIMV)
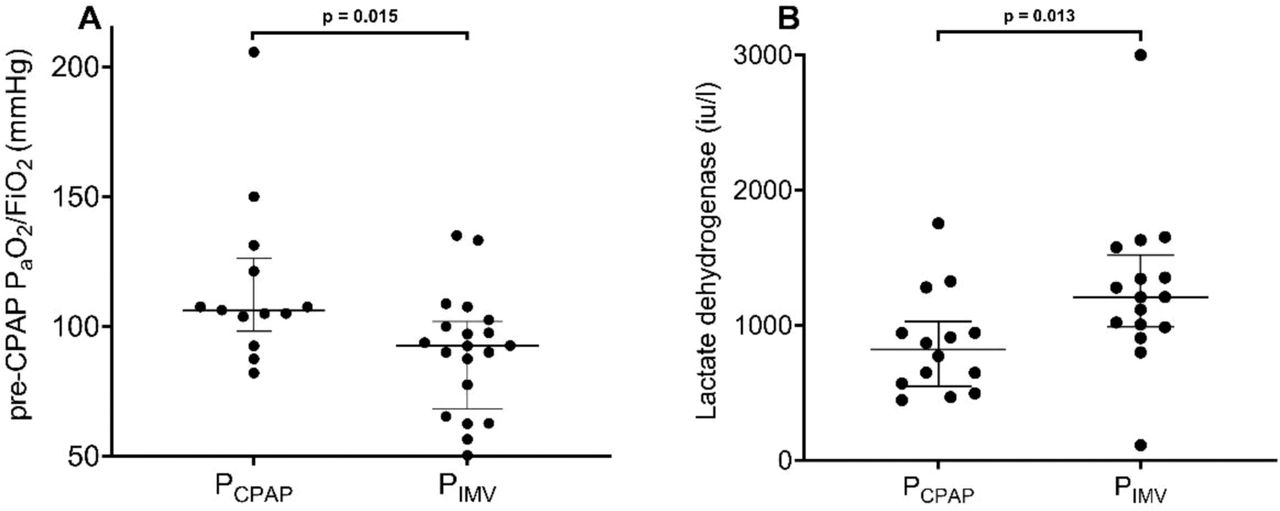
Pre-CPAP PaO2/FiO2 and LDH levels in patients who avoided IMV (PCPAP) and those who required IMV (PIMV). Differences between the two groups were compared using a Mann–Whitney U test. CPAP = continuous positive airway pressure; IMV = invasive mechanical ventilation; LDH = lactate dehydrogenase; pre-CPAP PaO2/FiO2 = ratio of partial pressure of arterial oxygen to a fraction of inspired oxygen preceding CPAP commencement.
Four of 14 (29%) patients who received CPAP as the ceiling of treatment were successfully weaned off CPAP after 152 (128–206) hours. Overall, in-hospital mortality was 21/52 (40%); 11/38 (29%) in the trial to avoid IMV group, and 10/14 (71%) in the ceiling of treatment group. Complications were uncommon; one (2%) patient developed a pneumothorax.
Early intubation strategy was previously fiercely advocated due to concerns of exceedingly high NIV failure rate in MERS, infection transmission risks and poorer outcomes with delayed intubation.4–6 In a non-SARS-CoV-2 population, the LUNG-SAFE study showed higher ICU mortality with NIV use in patients with PaO2/FiO2 <150 mmHg compared with early intubation.6 Data in SARS-CoV-2 are not available. Whether intubating patients after CPAP failure contributed to any excess mortality could not be inferred from this study and ought to be investigated further.
Conclusion
Ward-based CPAP was feasible and may reduce the need for intubation in patients with severe SARS-CoV-2 by 45%. Patients with high LDH and pre-CPAP PaO2 <100 were unlikely to avoid intubation with trial of CPAP. Larger studies should confirm the efficacy of CPAP therapy and investigate predictors of successful CPAP therapy in SARS-CoV-2 patients.
Conflicts of interest
None declared.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.