
Introduction
The criteria for possible SARS-CoV-2 infection focuses on evidence of pneumonia, acute respiratory distress syndrome, anosmia/change in sense of taste, fever ≥37.8°C, new persistent cough and breathlessness, as outlined by Public Health England. Triage of patients in the hospital setting typically relies on these symptoms. As elderly people with infections often present atypically there is a need to increase understanding of how COVID-19 affects this population.
Materials and methods
This retrospective observational study looks at the presenting complaints and observations during triage of elderly patients aged 70 and over who were admitted to a district general hospital in south-east England between 15 March and 31 May 2020 and tested positive for SARS-CoV-2 on admission. Clinical characteristics and observations were obtained from their initial hospital electronic record. History of presenting complaint documented by emergency department (ED) triage were analysed and symptoms were assigned to one or more of these 15 specific categories: shortness of breath, cough, fever, hypoxia, confusion, reduced consciousness, generally unwell, reduced oral intake, reduced mobility, fall, nausea and vomiting, abdominal pain, diarrhoea, myalgia and gastrointestinal bleed.
Results and discussion
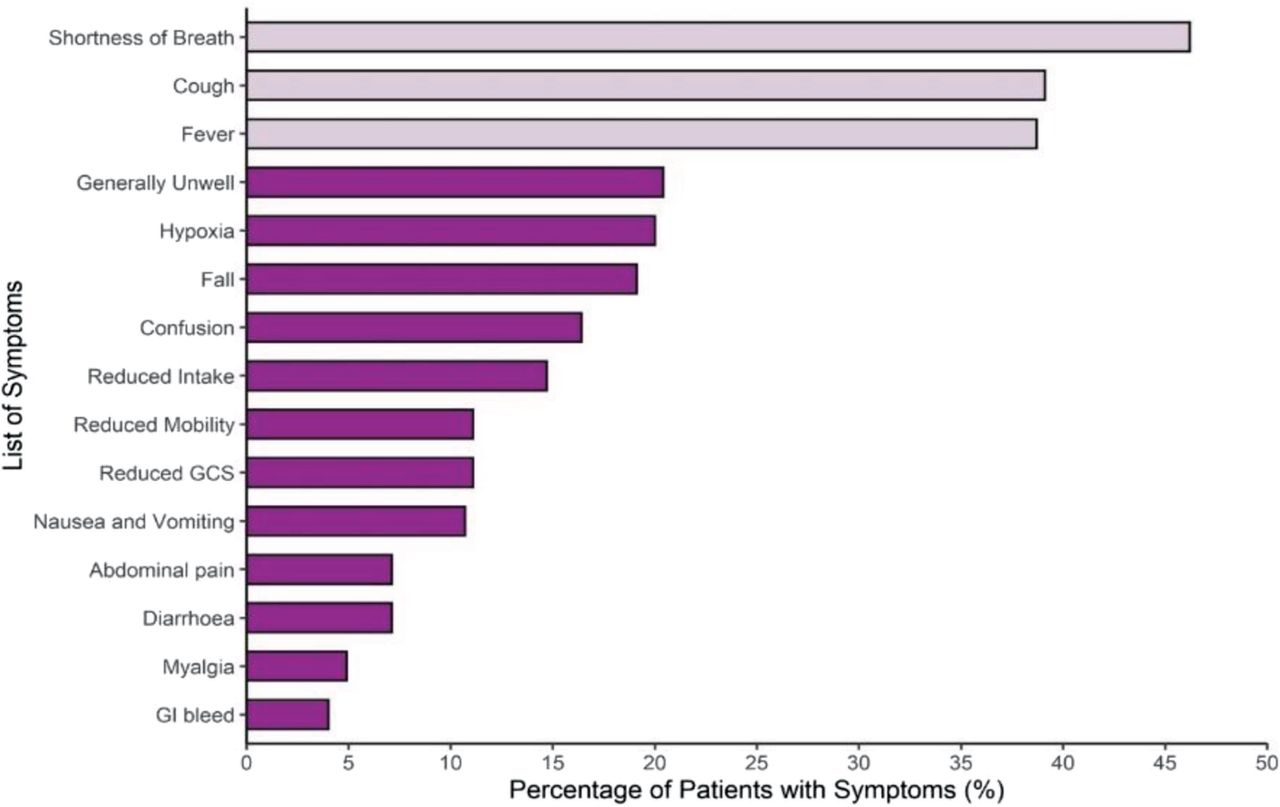
A total of 225 patients were included of whom 53.3% (n=120) were male and 46.7% (n=105) were female. The median age was 83 years (range 70–97). Only 11.5% (n=26) presented with the trio of cough, fever and breathlessness; 30.2% (n=68) did not present with any of these symptoms (p<0.001). The most frequent atypical complaints were ‘generally unwell’ (20%; n=46), falls (19%; n=43) and confusion (16%; n=37; Fig 1).
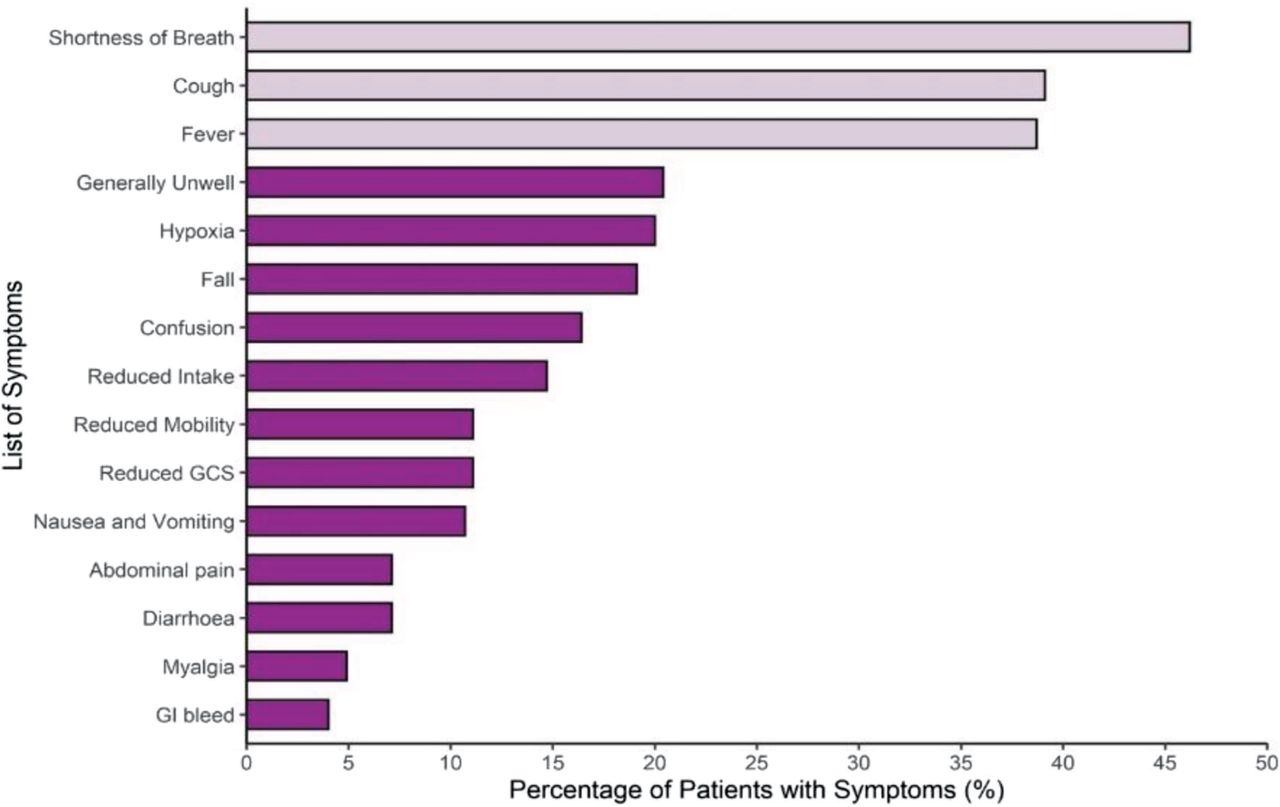
Distribution of presenting symptom(s) of patients with COVID-19.
In our cohort of elderly patients only 32.4% (n=73) recorded a temperature ≥37.6°C on admission, while 20.4% (n=46) were hypothermic with a temperature <36.4°C (p=0.0003); the remaining 36.0% (n=81) recorded a normal temperature of 36.5°C–37.5°C (p>0.05; Fig 2).
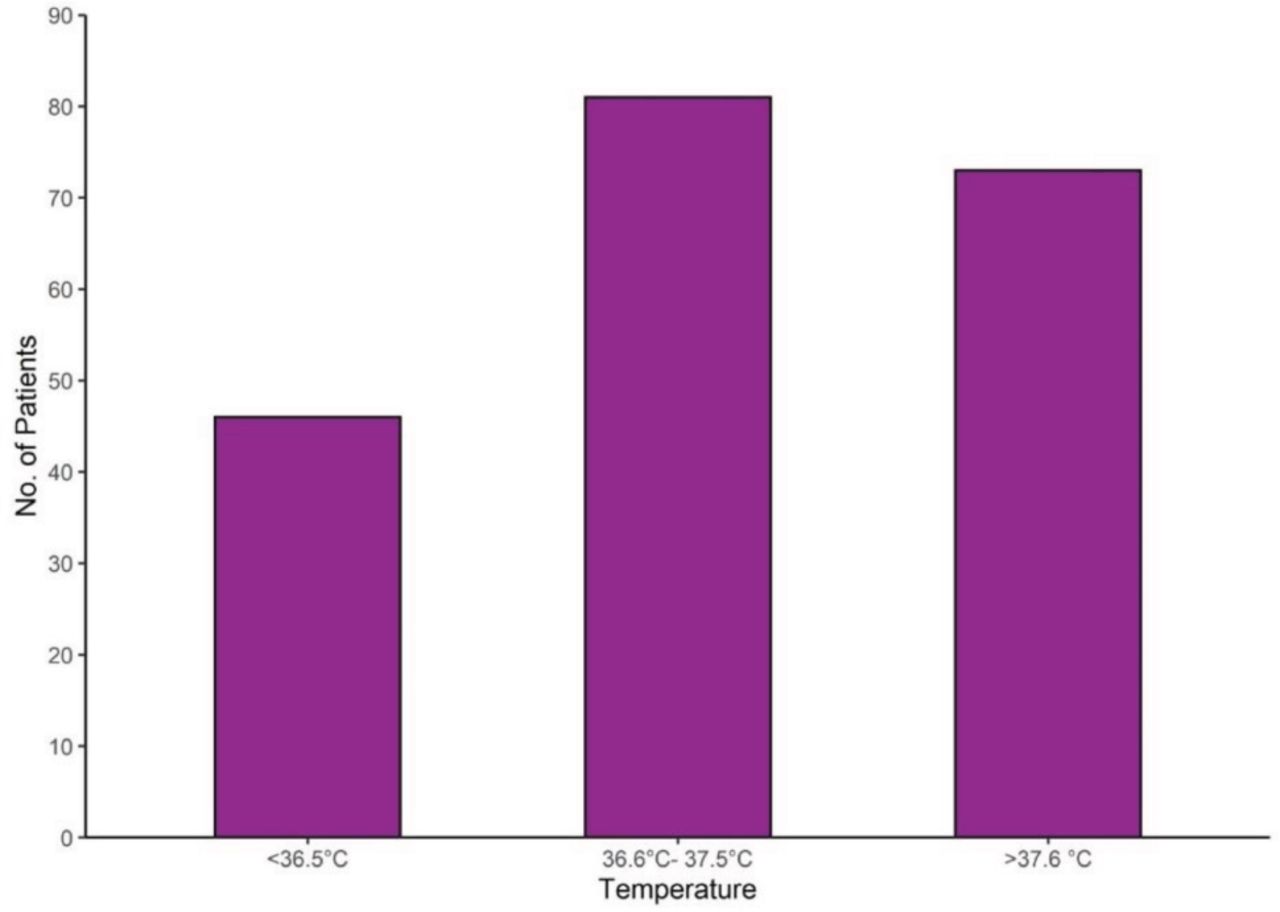
Distribution of temperature recorded on presentation to hospital.
Loss of sense of smell/taste was not recognised as a main symptom until 18 May 2020 and was not asked about frequently even following this date. Taking into account the high prevalence of cognitive impairment or delirium in this age group, many patients would not have been able to reliably report their symptoms and collateral histories may not have been accounted for in triage. Our retrospective study used hospital electronic records to ascertain the initial patient observations and did not account for whether patients may have received paracetamol prior to arrival in ED, potentially resulting in normal/low body temperatures.
Conclusion
A significant proportion of geriatric patients with COVID-19 presented with atypical symptoms and observations. The relatively high number of falls precipitating hospital attendance in this cohort, including resultant hip fracture, highlights the need for thorough history-taking to assess for possible cause of the fall, as well as accurate rapid diagnostic testing for SARS-CoV-2 to allow effective infection control in the hospital setting.1 The presence of delirium has already been identified as a frequent trigger for hospital admission in the presence of COVID-19 infection, and our study add further emphasise to this.2
Conflicts of interest
None declared.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.