
ABSTRACT
Hyperosmolar hyperglycaemic state (HHS) is a life-threatening metabolic complication of type 2 diabetes (T2DM) that often presents with neurological symptoms. A 74-year-old man with known T2DM presented to the emergency department with collapse, left-sided weakness and slurred speech (National Institutes of Health Stroke Scale (NIHSS) 3) and a biochemical profile consistent with HHS. When he further deteriorated (NIHSS 20), he was managed for concurrent ischaemic stroke. All his symptoms fully resolved after 24 hours, which coincided with establishment of normoglycaemia. Subsequent magnetic resonance imaging (MRI) of the head revealed a tiny parietal lobe infarct. Two further cases of HHS mimicking ischaemic stroke have been reported with symptoms and imaging findings resolving with treatment of HHS. Our case demonstrates how HHS can also accentuate symptoms of a minor stroke, highlighting the importance of excluding ischaemic stroke in HHS patients with neurological dysfunction. We recommend consideration of early MRI and/or computed tomography angiography in this cohort, especially in those appropriate for intervention.
Introduction
Hyperosmolar hyperglycaemic state (HHS) is a metabolic emergency seen in patients with type 2 diabetes mellitus (T2DM). It is a life-threatening condition with mortality of up to 20%, most commonly affecting older patients or those with multiple comorbidities.1 Neurological dysfunction is often present and can be the only presenting symptom. Correction of hyperosmolality and hyperglycaemia will typically fully resolve presenting symptoms.2 This case demonstrates the risk of occult ischaemic stroke in patients with HHS and neurological symptoms.
Case presentation
A 74-year-old man presented to his local emergency department (ED) having been found collapsed with a left-sided weakness and slurred speech. His past medical history included T2DM, hypertension, obstructive sleep apnoea, asthma and previous bladder cancer.
On arrival at the ED, his Glasgow Coma Scale (GCS) was 14 and National Institutes of Health Stroke Scale (NIHSS) score of 3 (1 point for dysarthria and 2 points for left leg weakness). His systemic examination was normal aside from hypertension (220/104 mmHg). His arterial blood gas results showed pH 7.37, partial pressure of carbon dioxide (pCO2) 5.63 kPa, partial pressure of oxygen (pO2) 8.6 kPa, bicarbonate of 24 mmol/L, glucose 38 mmol/L and base excess of 0 mmol/L. His urinary ketones were 0.9 mmol/L and he had a normal computed tomography (CT) of the brain. Subsequent blood tests confirmed serum glucose 51 mmol/L and serum osmolality of 322 mOsm/kg. He was promptly treated for HHS and hypertension.
He further deteriorated with reduced GCS 10 (E3, V2, M4) during the consultant review 5 hours later. His NIHSS had increased to 20 with reduced consciousness, inability to answer questions or follow commands, left hemiparesis, hemianopia, sensory neglect and dysarthria. The patient also became febrile with clinical evidence of pneumonia. An urgent stroke team opinion was requested.
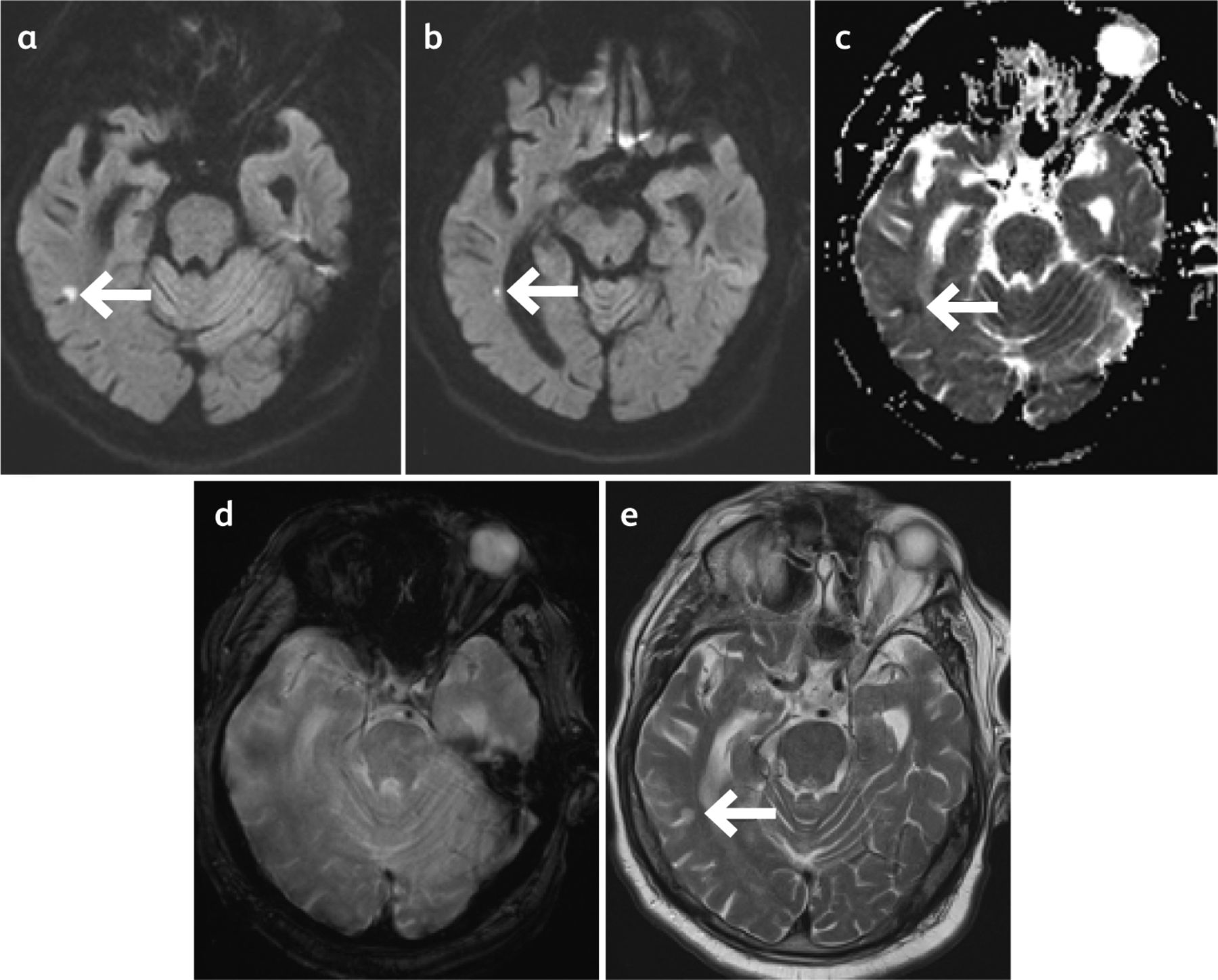
He was treated with aspirin empirically; he was not thrombolysed on admission and did not undergo CT cerebral angiography after stroke team review as it was felt that his initial presentation and subsequent deterioration was more likely to be related to HHS and pneumonia. He also received intravenous antibiotics and glyceryl trinitrate infusion following transfer to the stroke unit. His neurological deficits fully resolved after normoglycaemia was established after 24 hours of admission. However, the magnetic resonance imaging (MRI) of the head on day 4 of admission confirmed a tiny infarct at the right parieto-occipital region (Fig 1).
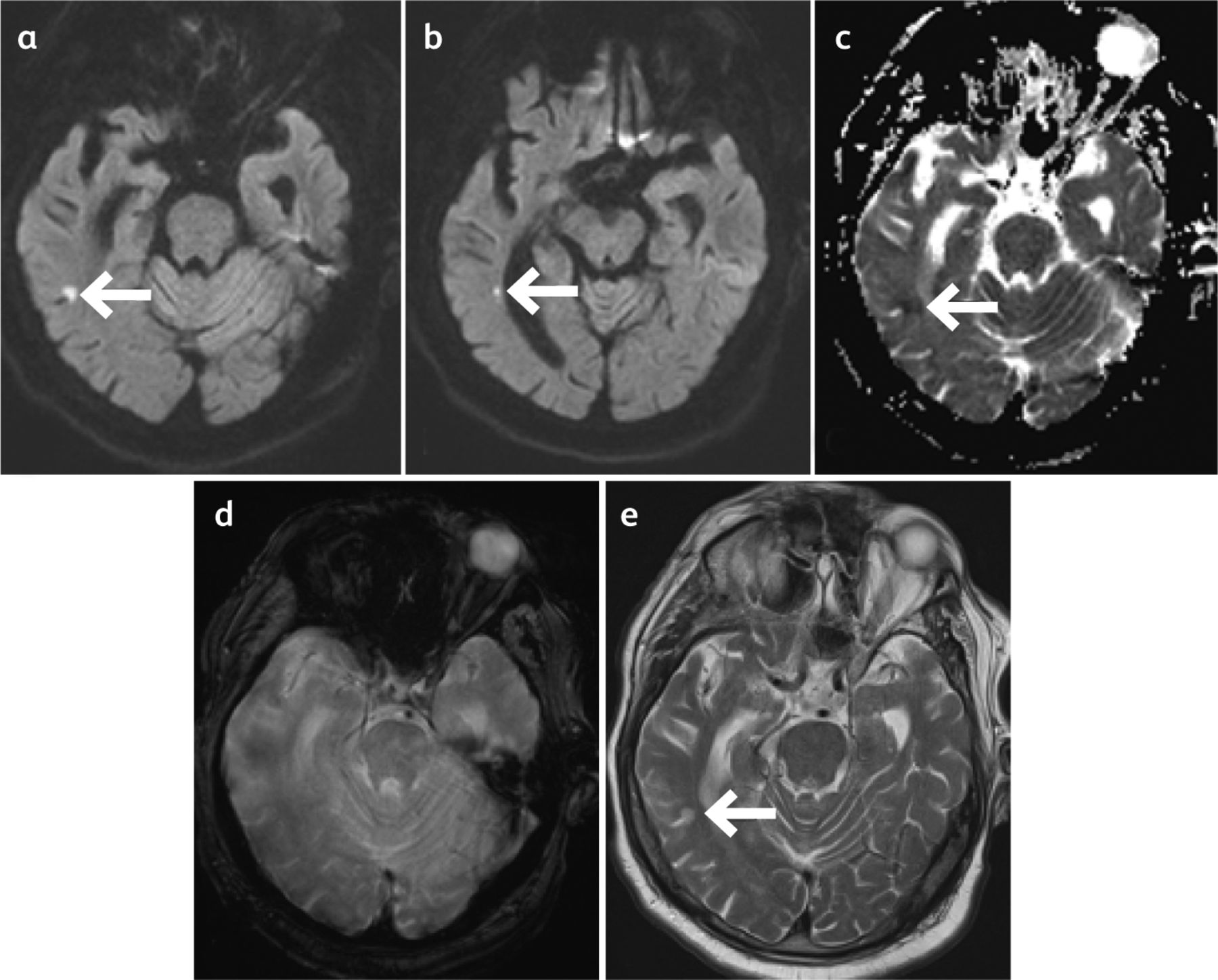
Magnetic resonance imaging of the head of a patient with ischaemic stroke and hyperosmolar hyperglycaemic state. a) Diffusion-weighted imaging. b) Diffusion-weighted imaging. c) Apparent diffusion coefficient. d) Gradient echo. e) T2-weighted imaging.
The patient was discharged following a week-long admission with an insulin regimen as per the specialist diabetic nurses and stroke clinic follow-up. He has been fully independent following discharge and with no recurrence of stroke symptoms at 6 months' follow-up with improved glycaemic control. Outpatient CT angiography did not show stenosis in the intracranial vessels, or arch of the aorta or carotid arteries. He also had a normal 7-day prolonged cardiac monitoring.
Discussion
HHS is an acute metabolic complication of type 2 diabetes, defined as marked hyperglycaemia resulting in serum osmolality >320 mOsm/kg without ketosis. Relative insulin deficiency and subsequent increase in counter-regulatory hormones leads to increased gluconeogenesis and glycogenolysis, and reduced uptake of glucose by peripheral tissues. Resulting severe hyperglycaemia leads to osmotic diuresis and profound dehydration.2 HHS symptoms may develop insidiously over several days, notably polydipsia, polyuria, lethargy and altered mental state.3,4 Common triggers are inadequate insulin therapy and illness such as infection, cerebrovascular disease and myocardial infarction.2 Timely correction of hyperosmolality, hyperglycaemia and electrolyte abnormality is key to survival.2 Without prompt treatment, HHS can lead to complications such as cerebral oedema, electrolyte derangement, myocardial infarction, stroke, seizures and central pontine myelinolysis.2
Despite neurological dysfunction being an established manifestation of HHS, there is limited research on the spectrum of neurological dysfunction. The most common presenting symptom is altered sensorium.5 Symptoms can range from lethargy to confusion and coma, with a demonstrated linear relationship between serum osmolality and obtundity.3 Others may present with focal neurology including hemianopia, hemiparesis, and focal or generalised seizures.3,4 A retrospective case series investigating the variation in neurological complications of HHS had shown that coma was the most common presentation, followed by seizures and hemichorea-hemiballismus.6
The two previous case reports of HHS mimicking stroke feature transient neurological dysfunction with transient abnormal MRI findings (Table 1).7,8 The first one described a 55-year-old man presenting with right homonymous hemianopia in the context of HHS.7 MRI of the brain revealed a subcortical lesion in left occipital lobe. However, both symptoms and MRI findings resolved on correction of HHS. Similarly, another report described an 67-year-old woman presenting with left middle cerebral artery syndrome.8 Investigations revealed severe hyperglycaemia. She was managed for HHS and received thrombolysis. MRI / magnetic resonance angiography / magnetic resonance perfusion at 6 hours showed a small abnormal area in the left posterior temporal lobe but no evidence of large vessel occlusion. Treatment of HHS led to resolution of all neurological symptoms within 24 hours of admission. Subsequent MRI at day 5 revealed no evidence of stroke or other condition consistent with her clinical presentation.It is theorised that either hyperosmolality and hyperviscosity result in hypoxic-ischaemic injury or ‘release’ of free radicals and the electroencephalography and the MRI findings are the result of reduced energy demand from inactive brain tissue.7,8 This, in turn, leads to reduced perfusion rather than tissue at risk of infarction. However, a mechanism by which HHS causes metabolic change in such tissue is not known.8
Summary table of reported cases of HHS mimicking stroke
Where neurological symptoms predominate, the diagnosis of HHS can be difficult to differentiate clinically from stroke.5 Importantly, our case highlights that the diagnoses are not mutually exclusive. Early studies around HSS and seizures often attributed patients with focal neurological deficits to Todd's paresis.8 However, at post-mortem, some of these patients had evidence of cerebral ischaemia.9 Those with HHS are at an increased risk of stroke due to the presence of diabetes and the acute prothrombotic state created by HHS.10,11 Therefore, lateralising or deteriorating neurology should not always be attributed to HHS but should prompt consideration of concurrent cerebral ischaemia, particularly if the deficits develop after initiating treatment for HHS. This will enable successful management of both pathologies, particularly for time sensitive interventions such as thrombolysis and thrombectomy. In cases similar to our patient, further urgent imaging (such as CT angiography or MRI of the brain) will help guide whether reperfusion therapy is required, since such intervention should not be taken lightly in view of the bleeding risk associated with hyperglycaemia.12
Furthermore, our case demonstrates the confounding relationship between HHS and stroke through the ability of HHS to accentuate stroke symptoms ie a minor stroke resulted in significant neurological deficit out of keeping with the size of infarct. Subsequent treatment of HHS then rapidly improved neurological function.
Conclusion
This case study of a 74-year-old patient presenting with HHS and lateralising neurology demonstrates the complex interplay between HHS and stroke. We propose that urgent MRI or CT angiography should be performed where possible in all patients with HHS and lateralising or deteriorating neurology. This will ensure appropriate management of both conditions and enable consideration for time-sensitive interventions such as thrombolysis and thrombectomy.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.