
ABSTRACT
Medical emergencies causing unplanned hospital admission place considerable demands on acute healthcare services. Some patients can be assessed and treated through ambulatory pathways without inpatient admission, via same day emergency care (SDEC), potentially benefiting patients and reducing demands on inpatient services. There is currently considerable variation within acute medicine in aspects of SDEC delivery ranging from overall service design to patient selection methods. Scoring systems identifying patients likely to be successfully managed through SDEC services have been suggested, but evidence of utility in diverse populations is lacking. Specific scoring systems exist for some common medical problems, including cardiac chest pain and pulmonary embolism, but further research is needed to demonstrate how these are most effectively incorporated into SDEC services. This review defines SDEC and describes the variation in services nationally. It reviews the evidence for their clinical impact, tools to screen patients for SDEC and current gaps in our knowledge regarding service deployment.
Introduction
With over 500,000 unplanned admissions monthly in the UK, emergency hospital admissions place significant demands on healthcare services.1 Medical emergencies are the most frequent cause, requiring assessment through acute medicine services,2 predominantly through referral from emergency medicine (EM) departments, with a proportion referred directly by community primary care services.3 Despite an increase in overall case-mix complexity and acuity, the proportion of patients admitted to NHS hospitals following presentation at an emergency department has remained stable,4 although this leads to an overall increase in the number of admissions.
Up to 80% of hospital beds contain unplanned admissions; during times of increased pressure, such as winter or waves of the recent COVID-19 pandemic, increased unplanned admissions directly impact the delivery of elective services.5 Although many patients in acute medical services require further investigation and treatment, acuity varies and up to 30% of admissions are discharged within 24 hours of arrival to hospital.3,6,7 The fact that a proportion can be discharged home within hours of arrival8 suggests alternative treatment pathways could potentially avoid admission for a subset of these patients, while still providing necessary reassurance, investigation or treatment.
Same day emergency care: definition and national variation
Same day emergency care (SDEC) is the delivery of urgent care in a hospital setting without overnight inpatient admission.9 SDEC aims to benefit both patients and healthcare service providers, reducing demand on inpatient services and avoiding the risks associated with inpatient admission.8
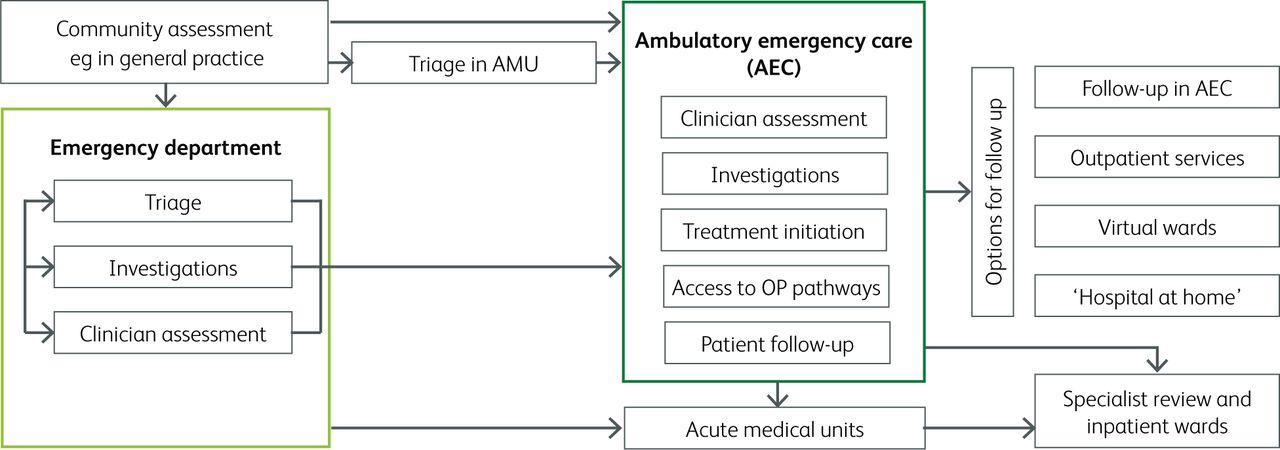
Acute and general medicine teams deliver SDEC in ambulatory emergency care (AEC) units,10 usually identifying suitable patients based on an expectation of discharge, with mapped assessment and treatment pathways that do not include an overnight stay. Patients should receive assessment to ensure they are suitable for discharge before leaving hospital, and should be given appropriate safety-netting advice.11 Not all SDEC assessments and treatments need to be delivered within the same day, and patients can return on subsequent days, including for specialist outpatient services. Pathways to assess and exclude diagnoses in new admissions may be delivered alongside services providing specific procedures or treatment for selected conditions,12,13 for example ambulatory management of cellulitis requiring intravenous antibiotics.10 Within these general parameters, there is considerable variation in pathway design and delivery (Fig 1).14,15
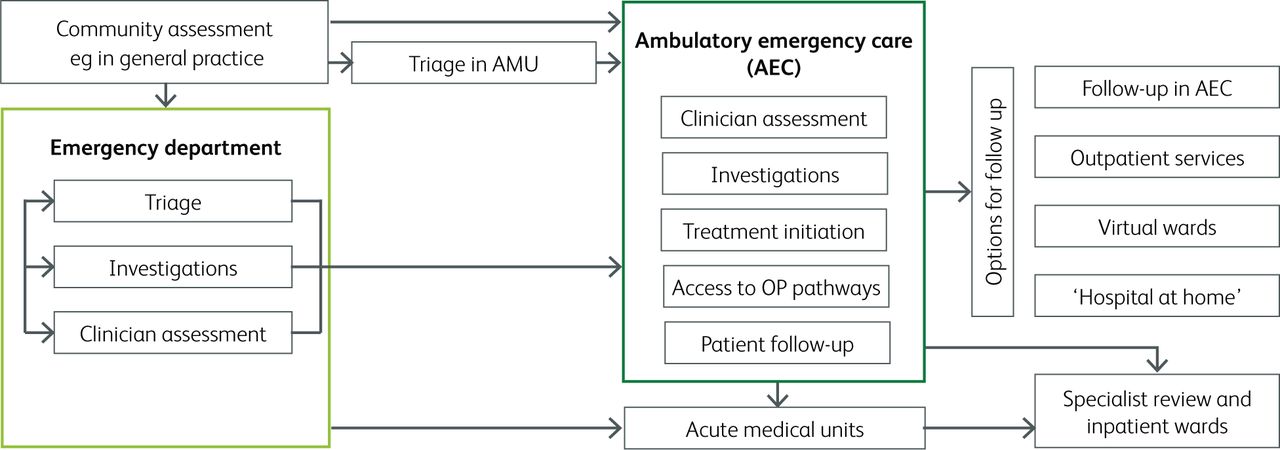
Ambulatory emergency care (AEC) pathways. Possible routes in the acute care admission pathway where patients can access AEC services, and the potential services delivered through AEC. OP = outpatient.
In a recent survey of UK acute hospitals, 99% of responders reported that they deliver ambulatory emergency care.3 On average, 20% of patients admitted to acute medicine are seen through AEC; however, the proportion varies, with some centres seeing up to 75% of admissions through this route.14 This variation likely has multiple underlying causes. The local patient population may affect the number deemed suitable for SDEC, with some patient cohorts, such as the very elderly or pregnant patients, automatically excluded in some centres.16 Not all centres have additional services that facilitate AEC, such as outpatient parenteral antibiotic therapy (OPAT) or rapid access to specialist clinics.17
Despite variation in the provision and model of SDEC services, there are agreed performance indicators for comparison of services. These include measurement of a National Early Warning Score (NEWS) within 30 minutes of arrival, clinician assessment within 1 hour and use of validated condition-specific risk stratification tools.11 While it is recommended to monitor the proportion of admissions treated within SDEC,11 further evidence is needed regarding how many patients are likely to be suitable for, or benefit from, SDEC.
Evidence for SDEC-driven improvements in care
Delivering SDEC is a priority within the NHS and the current NHS Long Term Plan recommends that 30% of patients attending acute services should be treated via SDEC.18 However, despite this policy drive, evidence of positive impact on patient care is currently limited.
There is evidence of the safety of ambulatory pathways for certain, specific conditions, such as pulmonary embolism, when using appropriate, disease-specific scoring systems,19 but robust evidence of benefit is lacking for most conditions seen through SDEC. For many medical conditions where it is suggested that a high proportion of patients may be suitable for SDEC (Table 1),12 evidence is limited on how to safely identify the patients that can be managed in this way, and how services could be most effectively structured to ensure benefit to patients and the wider healthcare system. Indeed, much of the evidence guiding SDEC relies on case studies of service development.20–22 No studies have compared different SDEC service models, or SDEC to usual care (hospital admission), the number of patients that may benefit from SDEC services remains unknown, and there are no health economics studies evaluating the cost effectiveness of SDEC. Despite this lack of evidence, SDEC pathway development for several conditions has been widely encouraged.12,20 For acute healthcare providers, there remains uncertainty as to which model to deploy, how to identify suitable patients, and what add-on services might be needed.
Medical conditions suggested as suitable for same day emergency care
Screening for SDEC suitability
To effectively deliver SDEC, appropriate patients must be identified, with those likely requiring admission directed to acute medical units, and those most likely to be discharged home directed to SDEC.23 Two established scoring systems are available to identify SDEC patients from unselected medical admissions, ie medical admissions that have not been selected out as belonging to a specific medical specialty:20 the Ambulatory Care Score (Amb Score) and the Glasgow Admission Prediction Score (GAPS).
The Ambulatory Care Score
The Amb Score identifies patients likely to be discharged from hospital on the day of admission, and thus suitable for SDEC pathways.24 It can be used at multiple points in patient pathways, including primary care settings, is not disease-specific, and is recommended by the Royal College of Physicians.10
The Amb score was derived through a small single-centre cohort, with 282 primary care referrals for derivation, and 343 patients for validation. Outcomes were dichotomised as early discharge (within 12 hours) and admission (≥48 hours); those admitted for 12–48 hours were excluded. Factors influencing likelihood of early discharge were used to generate a score predicting early discharge (described in Table 2). An Amb score ≥5 had 96% sensitivity (95%CI 90–98%) and 62% specificity (95%CI 55–68%) in identifying those likely to be discharged with 12 hours of assessment, and therefore suitable for SDEC.
The Amb Score
A single-centre study of 200 acute medicine referrals in Taunton showed the Amb score had lower sensitivity in predicting early discharge than the original study,25 with a score ≥5 having 88% sensitivity and 69% specificity. This may reflect local population differences, suggesting score performance varies with local demographics. Demographics or comorbidities of subjects were not reported, making it difficult to assess how these cohorts represent the population at large.
Glasgow Admission Prediction Score (GAPS)
The GAPS, derived from a multi-centre retrospective cross-sectional study of unscheduled EM attendances, estimates probability of inpatient admission at initial hospital triage.26 Variables were combined into a six-variable scoring system predicting admission (Table 3). The GAPS also considers age and baseline physiology, as well as triage category at presentation, and, like the Amb score, is not disease-specific. The authors recognised the impact of local population demographics, and did not recommend specific cut-off scores for use in other hospitals, instead advising venues to conduct local validation to determine individualised thresholds. In North Glasgow, a GAPS >15 to predict admission had 78.0% sensitivity (95%CI 77.8–78.2%), and 81.7% specificity (95%CI 81.6–81.9%).
Glasgow Admission Prediction Score26
A single-centre study suggested EM triage nurses had higher accuracy in predicting admission when confident about the outcome (ie they estimated probability of admission to be ≥95% or ≥5%) but the GAPS performed significantly better when the probability of admission was ranked between 6%–94% (the majority of cases in the clinical caseload studied). The best performance was obtained by overruling the GAPS in cases of high clinical certainty, suggesting clinicians consider factors when predicting admission that are not captured within the GAPS.27
Studies directly comparing the performance of the Amb and GAPS systems are limited. One comparison study suggests that the GAPS may predict inpatient admission for patients presenting to EM triage more accurately. This prospective cohort study of attendances at two large teaching hospitals in Glasgow and Sheffield found the GAPS to be a better predictor of discharge from hospital within both 12 and 48 hours,28 with cut-offs maximising sensitivity and specificity of GAPS <18 and Amb score >5. However, one of the centres was where the GAPS was originally derived, potentially impacting performance.
Limitations of scoring systems
There are a number of limitations to consider before embedding these systems within acute services.
Both systems were derived in single geographical areas and may be affected by local population demographics, impacting generalisability to the wider UK population. The Amb Score was derived and validated in rural Wales,24 while only 18.5% of the UK population live in a rural setting. A higher proportion of the Welsh population identify as White British than most other UK regions.29 The GAPS was derived in Glasgow,26 which has poorer health outcomes and lower life expectancy than other major UK urban areas.30 While Glasgow's ethnic diversity has increased over recent years, non-White ethnic groups comprise less than 15% of the population,31 considerably lower than many other UK cities.32 Ethnicity is associated with the prevalence and age of onset of certain comorbidities, including cardiovascular disease, renal disease and diabetes, which may increase the need for inpatient admission.33
Using the Amb Score, women have an increased likelihood of discharge within 12 hours. This may be population-specific; the derived population is known for its historical coal mining industry, potentially increasing morbidity in men disproportionately.34 In the GAPS,26 women were significantly more likely to be admitted than men (not included in the final score due to small effect size (OR 1.2)). Using the Amb score, male patients over 80 years old, with no other negative features, would be deemed unsuitable for SDEC.
Implementation of the GAPS is further complicated by the need to validate binary cut-off levels within a specific population.26 This requires the skills and resource to undertake a robust analysis at each centre to determine appropriate cut-offs with acceptable sensitivity and specificity to predict admission.
There are also practical considerations when implementing the Amb score. Despite aiming to identify patients before full clinical assessment, a judgement predicting intravenous treatment is required, which may be difficult before reaching a diagnosis. Prediction without clinician involvement, for example incorporating machine learning, has not yet been investigated. Whether intravenous therapy does necessitate admission varies between services, and many hospitals have well-established OPAT services, with pilot studies suggesting other intravenous treatments, including diuretics, could be delivered effectively in alternative settings, reducing hospitalisation.35,36
Evaluation of score performance throughout the year is needed. The Amb Score was derived and validated from attendances in summer months.24 Acute services face additional pressures during winter,14 with seasonal variation in common presentations including respiratory diseases,37 and an increased average length of hospital admission,38 which likely impacts the need for admission for the unselected patient cohort overall.
Both the GAPS and Amb Score incorporate early warning scores (EWS). Previous research suggests a raised NEWS measured pre-hospital predicts inpatient admission and poor outcomes following admission.39,40 However, the single EWS measurement incorporated into the GAPS and Amb score may not fully reflect a patient's trajectory, with the change in EWS potentially more informative in directing clinical care, and a normal EWS does not equate to a low risk of morbidity or mortality in all patients. Since 2018, the more nuanced NEWS2 score, including new onset confusion and adjusted oxygen saturation ranges in patients with hypercapnic respiratory failure, has been mandated nationally in acute hospitals.41,42 The impact of incorporating the NEWS2 score in the GAPS and Amb score has not been evaluated.
Stratification after initial diagnostic tests
The GAPS and Amb scores are designed for unselected medical cohorts, early in patient pathways before a diagnosis is suspected. However, deploying scoring systems later in admission pathways may still prevent prolonged admission. Two clinical examples include patients requiring exclusion of acute coronary syndromes (ACS)43 or pulmonary embolism (PE). These conditions often present with shortness of breath and chest pain, the most common presenting symptoms in acute medical services.24 For these conditions, diagnosis-specific scoring systems are likely more appropriate in the first instance, alongside blood biomarkers.
Suspected cardiac chest pain
Chest pain accounts for 5–10% of emergency hospital admissions,44,45 with approximately 41 people per 1,000 population attending annually due to non-specific chest pain.46 Although some patients have serious underlying causes, half of those presenting to the emergency department have non-cardiac, non-specific or musculoskeletal pain.47 Many of these causes could be managed within SDEC where they require further assessment. Currently, evaluation with 12-lead electrocardiogram and high-sensitivity troponin I or T measurement on arrival, with further testing guided by a validated risk stratification tool, is recommended for suspected cardiac chest pain.48 Risk stratification tools assessing clinical features include the Emergency Department Assessment of Chest Pain Score (EDACS)49; History, Electrocardiogram, Age, Risk factors and Troponin (HEART) score50 and Thrombolysis in Myocardial Infarction (TIMI) score.51 Comparison of these tools showed the EDACS could rule out acute MI in 48.3% of patients with suspected cardiac chest pain, with a sensitivity of 96.1%, suggesting 3.9% of those with acute MI would be falsely reassured.52
Some high-sensitivity troponin assays can rule out MI in chest pain starting >1 hour ago with a single measurement.47 A low (but possibly abnormal) level on first measurement requires repeat testing after one hour, with acute MI ruled out if there is no increase.47 Meta-analysis found this strategy had sensitivity >98%, a negative predictive value (NPV) of >99%, and specificity of >90%; however, the positive predictive value (PPV) varied between 50%–75%, suggesting a high number had acute MI identified as a possible diagnosis, but later excluded on further investigation.53 This testing approach ruled out acute MI in 55% of patients with suspected cardiac chest pain and could be incorporated into SDEC pathways.
Pulmonary embolism
Investigation and management through ambulatory pathways is recommended for a subset of patients with diagnosed or suspected PE. Early discharge with follow-up through ambulatory or outpatient services is recommended for low-risk patients with confirmed PE, defined by risk stratification tools including the Pulmonary Embolism Severity Index (PESI) or simplified PESI (sPESI).54
These tools combine independent predictors of 30-day mortality in PE, incorporating age, gender, comorbidity and clinical features including tachycardia and hypotension, to identify patients at low risk of mortality. Using the PESI, 30-day mortality is ≥1.6% in 'very low risk' patients and 3.6% if 'low risk,55 with these two categories comprising approximately half of patients with PE.56 The sPESI dichotomises risk as low or high with approximately a third of cases classified as low risk, with 1% 30-day mortality.57
This relies on prompt access to appropriate imaging to confirm the diagnosis within timescales allowing delivery of SDEC.58 However, these same tools can facilitate ambulatory investigation of suspected PE, with patients identified as low risk receiving anti-coagulation treatment before discharge home, subsequently returning for confirmatory imaging through AEC services.54
Similar approaches may identify patients at low risk of adverse outcome for ambulatory investigation of specific symptoms, including jaundice59 or upper gastrointestinal bleeding (using the Glasgow-Blatchford Bleeding Score),60 or where a diagnosis has been reached, for example the CURB-65 score in community acquired pneumonia.61
Point of care testing in SDEC
Where diagnostic testing is required, point of care (POC) testing may facilitate rapid availability of results, shortening assessment pathways by reducing test turnaround time. Use of POC d-dimer testing to exclude deep vein thrombosis and PE is well established, with POC test accuracy comparable to laboratory testing.62,63 High-sensitivity POC troponin tests have been developed, but diagnostic performance requires further evaluation.44 Some POC investigations replace standard diagnostic tests and comparable performance must be demonstrated, while some provide additional assessment, such as point-of-care ultrasound (POCUS). POCUS has increasing evidence of utility in a range of presentations,63–65 but requires appropriately trained staff, and current availability in acute and emergency medicine settings varies.7,66
SDEC and virtual wards
A middle ground may exist, where risk of deterioration does not necessitate hospital admission, but care requirements exceed standard community provision. Early assessment could identify patients for discharge with increased outpatient support, with follow-up via home visits, telephone consultation or remote monitoring.
Home monitoring following early discharge of patients with chronic obstructive pulmonary disease with low mortality risk67 may reduce healthcare costs, without increasing readmissions or death.68 Previous evidence suggests discharge with ‘virtual ward’ support may decrease readmissions in frail older adults;69 however, this is compared to discharge with usual care and whether this approach could facilitate discharge in patients who would otherwise have been admitted was not assessed. Current evidence is limited to single centre, often observational studies68–70 and evidence from large multicentre trials is lacking.
Some centres have rapidly developed and implemented ambulatory pathways for patients with COVID-19, avoiding inpatient admission for those at low risk of deterioration.71,72 Pathways often combine routinely measured clinical features with ‘rapid walk tests’ identifying falling oxygen saturations on walking.71,73 Some ambulatory pathways included virtual review, providing pulse oximeters for home oxygen saturation monitoring.74 Again, evidence is limited to observational studies without control groups, but readmission appears to occur in approximately 11% of patients.71
Although these pathways may reduce pressure on acute services, and have positive patient feedback,71 the impact of delivering and supporting an additional service must be considered. Delivering ambulatory pathways and virtual reviews requires trained healthcare professionals. Healthcare staffing is a finite pool, and those with the skills to deliver these services are likely already delivering SDEC in other areas. Redistributing time and resource to new services may reduce ability to deliver existing services and thorough health economic evaluation is needed to assess the wider impact and costs of new services, alongside assessment of clinical benefit.
Knowledge gaps and research priorities
Further research is needed to understand how SDEC can deliver the greatest benefit to both patients and the healthcare system.
First, greater understanding of the different models currently deployed across centres is needed, including the underlying reasons for the chosen service structure. A common model may not be possible across diverse healthcare settings, but agreed patient selection criteria and common performance indicators would facilitate comparison. Although key indicators for SDEC are recommended,11 outcomes assessing impact (including death, re-presentation, admission, and patient experience) are not reported or compared nationally. Comparing internationally, while there may be differences in health service structure, there are similarities in healthcare demand,75 and SDEC models used should be evaluated in comparison to alternative approaches utilised in other countries, for instance the increased primary care services offered in the Netherlands.76
Second, strategies to identify suitability for SDEC require wider validation. Further evidence should demonstrate how screening for SDEC can be most effectively incorporated into referral pathways, including where and when this screening occurs in admission pathway, and by whom, including the level of clinical experience or training in specific scoring systems required. Currently suggested risk scoring systems have been derived in local populations, and head-to-head comparison of performance in wider regions with diverse demographics is needed, alongside assessment of whether new acuity scores (such as NEWS2) improve performance, and whether these simple scores could be supplemented in more digitally mature settings, enabling more stratified or personalised risk scoring. Reassurance that these scores can be used safely, predictably identifying patients at low risk of death or adverse outcome, must be shown through multicentre, prospective validation, in healthcare services that are representative of all centres where the scores would be used. Additional factors not included in these scoring systems are known to be associated with mortality after discharge from the emergency department, including levels of comorbidity,77,78 dependence in activities of daily living,79 and specific symptoms such as dyspnoea,80 fatigue,81 and recurrent falls.78 How these factors should be incorporated into streaming processes for medical admissions that utilise scoring systems requires assessment. The impact of scoring systems on access to SDEC for patient cohorts with different risk profiles, including pregnant patients and older adults, also needs evaluation.
Third, research may point to an agreed list of minimal additional services or tools required to optimise SDEC, such as POC testing, POCUS or specific out-reach services such as OPAT. Virtual wards may offer potential pathways, combining remote medical review and structured safety-netting without requiring inpatient admission.
The proportion of medical patients that may benefit from a SDEC service is unknown, and must be assessed alongside these other factors. Understanding the impact of proposed service models on defined patient outcomes and health service delivery is important, including the expected benefit to patients, but also staffing and infrastructure implications. Health economic analysis of different models would inform cost-effective healthcare choices.
Conclusion
SDEC is a current priority in NHS acute care service provision, aiming to reduce hospital admission for selected patients and therefore inpatient service demands. However, there remain several unanswered questions.
To understand how systems can be effectively implemented, an evaluation of clinical benefit is needed. Whether greater benefit would be gained from standardisation across healthcare settings, or pathways adapted to local population demographics and healthcare needs, is unclear. The potential wider repercussions of any new system must be considered, with health economic evaluation of potential impacts on acute care services. This will build an evidence base to guide the delivery of safe and effective SDEC.
Key practice implications
Same day emergency care (SDEC) delivers assessment, investigation and treatment without overnight admission to an inpatient hospital bed.
Structure of SDEC services varies nationally within the UK, and there is no clear evidence regarding the optimum way to design these services.
Scoring systems have been suggested to identify patients from unselected medical admissions suitable for SDEC services, including the Glasgow Admission Prediction Score (GAPS) and the Amb Score.
When considering use of a scoring system to identify patients for SDEC, local population demographics must be considered as these can impact score performance, and local assessment of performance may be needed before implementation.
SDEC pathways can be especially effective for specific conditions, such as suspected cardiac chest pain with validated risk stratification tools and suspected PE if at low risk of mortality, determined by PESI or sPESI scoring system.
Additional services may facilitate the delivery of SDEC, such as virtual wards, but the impact of running an additional service on delivery of current services should be considered.
There remain multiple gaps in our knowledge about how best to structure SDEC services and identify appropriate patients, to gain maximum benefit for patients and for healthcare services.
- © Royal College of Physicians 2022. All rights reserved.
References








{kind=link}
Jump to section
- Article
- ABSTRACT
- Introduction
- Same day emergency care: definition and national variation
- Evidence for SDEC-driven improvements in care
- Screening for SDEC suitability
- Stratification after initial diagnostic tests
- SDEC and virtual wards
- Knowledge gaps and research priorities
- Conclusion
- Key practice implications
- References
- Figures & Data
- Info & Metrics