
ABSTRACT
A 44-year-old woman presented to the emergency department with sudden chest tightness and breathlessness, and a chest X-ray revealed unilateral pulmonary oedema (UPO). Colour Doppler echocardiography showed that the leaflet prolapsed with severe regurgitation, and the regurgitant jet tended to blow rightward within the left atrium. With the assistance of mechanical ventilation and venoarterial extracorporeal membrane oxygenation, the patient underwent mitral valve replacement. UPO is easily misdiagnosed, which leads to delays in treatment. Therefore, accurate diagnosis and immediate treatment are crucial.
Introduction
The usual pattern of cardiogenic pulmonary oedema is a bilateral symmetrical opacity, also called ‘butterfly shadow’. In contrast, unilateral pulmonary oedema (UPO) is uncommon and easily misdiagnosed at the initial stages, turning into an independent risk factor for deaths. The most common cardiogenic cause of UPO is acute mitral regurgitation (MR) with a directed jet. Here, we report a case of UPO caused by acute MR.
Case presentation
A 44-year-old woman complained of sudden chest tightness and breathlessness with dizziness, and was not relieved after treatment by the local hospital. The symptoms occurred with no obvious cause and had been noted for 5 hours. Thus, she presented to the emergency department. Investigations revealed a significant systolic murmur at the fourth left sternal border. Echocardiography showed massive mitral valve regurgitation. On admission, orthopnoea was present, and vital signs were a heart rate of 118 bpm, blood pressure of 112/80 mmHg, respiratory rate of 31 breaths per minute and oxygen saturation of 78% at 8 L/minute of oxygen through a mask. Respiratory system auscultation revealed decreased breath sounds and coarse crackles in the entire right hemithorax. Cardiac auscultation revealed a holosystolic murmur at the fourth left sternal border. Laboratory testing revealed a white blood cell count of 8.12 × 109/L, C-reactive protein level of 10.4 mg/dL, brain natriuretic peptide level of 929 pg/mL and high-sensitivity troponin I level of 342.5 pg/mL. Electrocardiography showed sinus tachycardia.
Severe hypoxia was present when the patient was admitted to the department and she was intubated immediately for mechanical ventilation. However, hypoxia and tachycardia remained and haemodynamics collapsed within an hour after treatment with high-dose vasopressors. Therefore, the patient unfortunately lost the opportunity of emergency surgery. Despite having poorly filled blood vessels, venoarterial extracorporeal membrane oxygenation (VA-ECMO) was performed within 30 minutes. Chest X-ray revealed right-side significant alveolar–interstitial infiltrates without cardiomegaly (Fig 1). Colour Doppler echocardiography showed that the posterior leaflet prolapsed with severe regurgitation (Fig 2a), and the regurgitant jet tended to blow rightwards within the left atrium (Fig 2b). With VA-ECMO, the patient was treated with mechanical ventilation and medication: diuretics, vasopressors and antibiotics. On day 4, the patient's haemodynamics and respiratory conditions improved, and the chest X-ray showed that pulmonary oedema was relieved. Then, mitral valve replacement with a mechanical GKS-27M was carried out. The treatment with VA-ECMO continued due to myocardial stunning. On the day after the operation, VA-ECMO and the chest drains were successfully weaned.
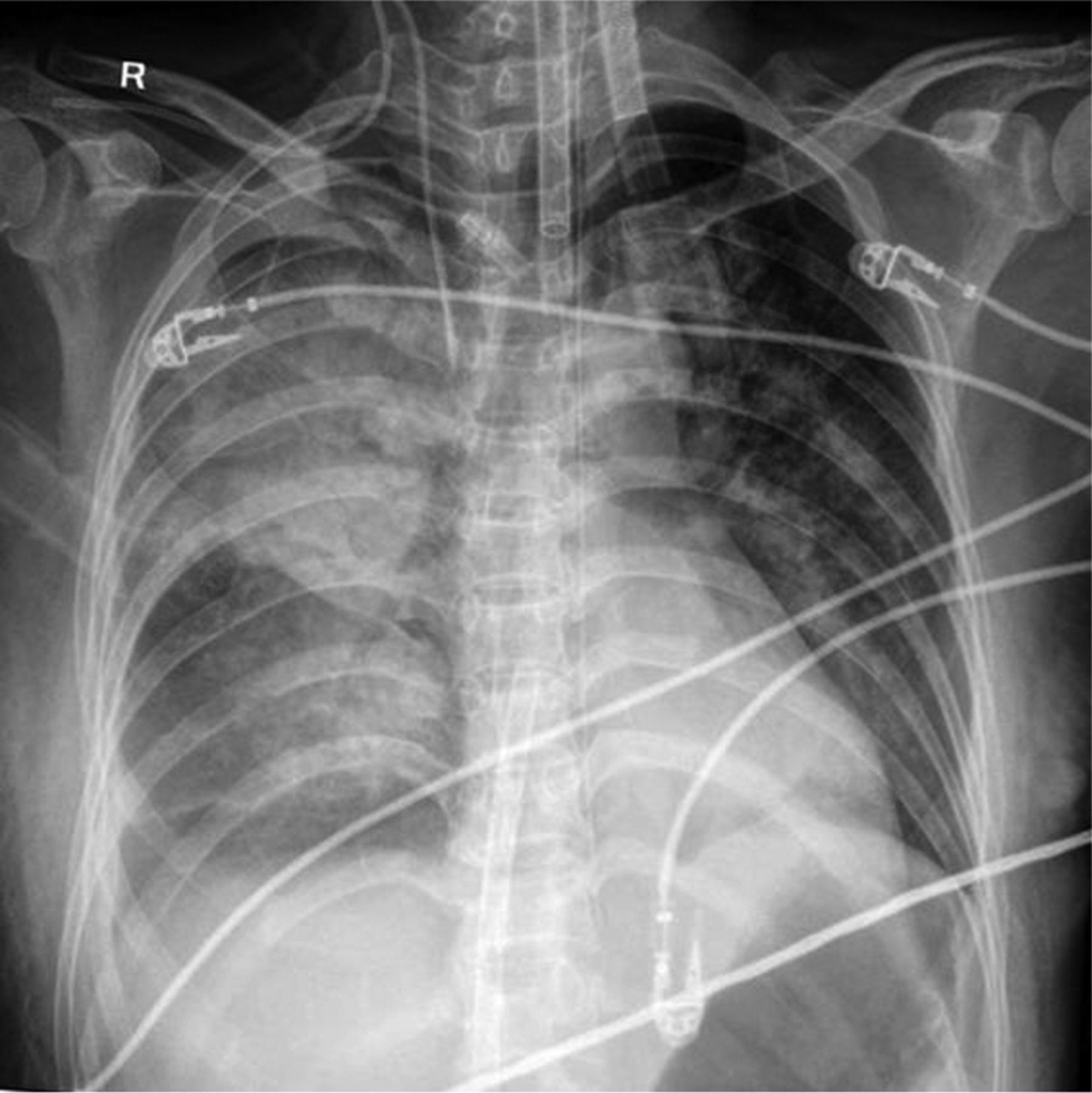
Chest X-ray showing significant right-side alveolar interstitial infiltration without cardiomegaly.

Colour Doppler echocardiography. a) The posterior leaflet is prolapsed with severe regurgitation. b) The regurgitant jet is clearly tending to the right in the left atrium. LA = left atrium; LV = left ventricle; RA = right atrium.
Outcome and follow-up
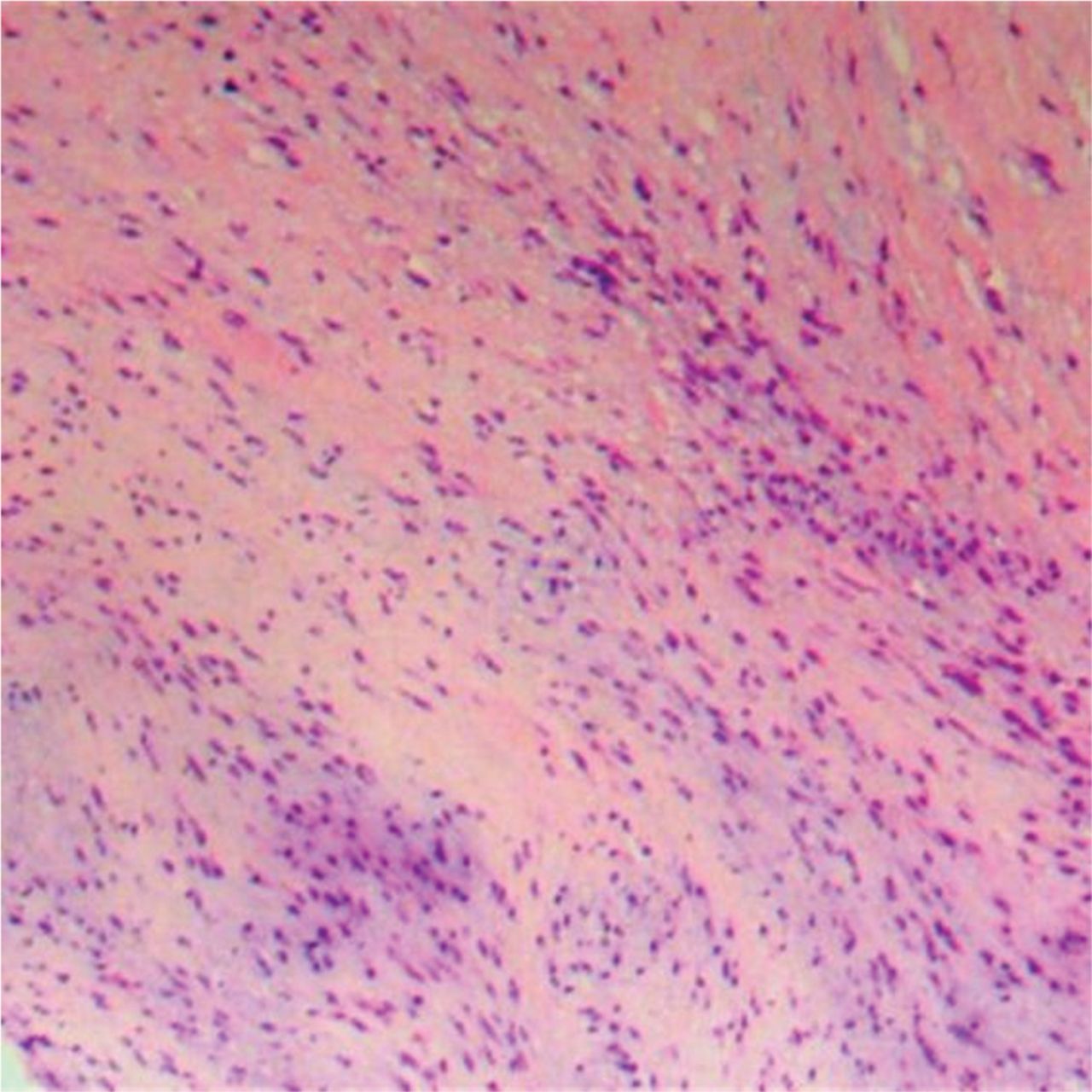
The patient started taking warfarin because of her mechanical valve and there were no complications in her outpatient follow-up. The pathological and histological findings showed that the chordae of the posterior mitral leaflet (P2) was ruptured with mucinous degeneration (Fig 3).
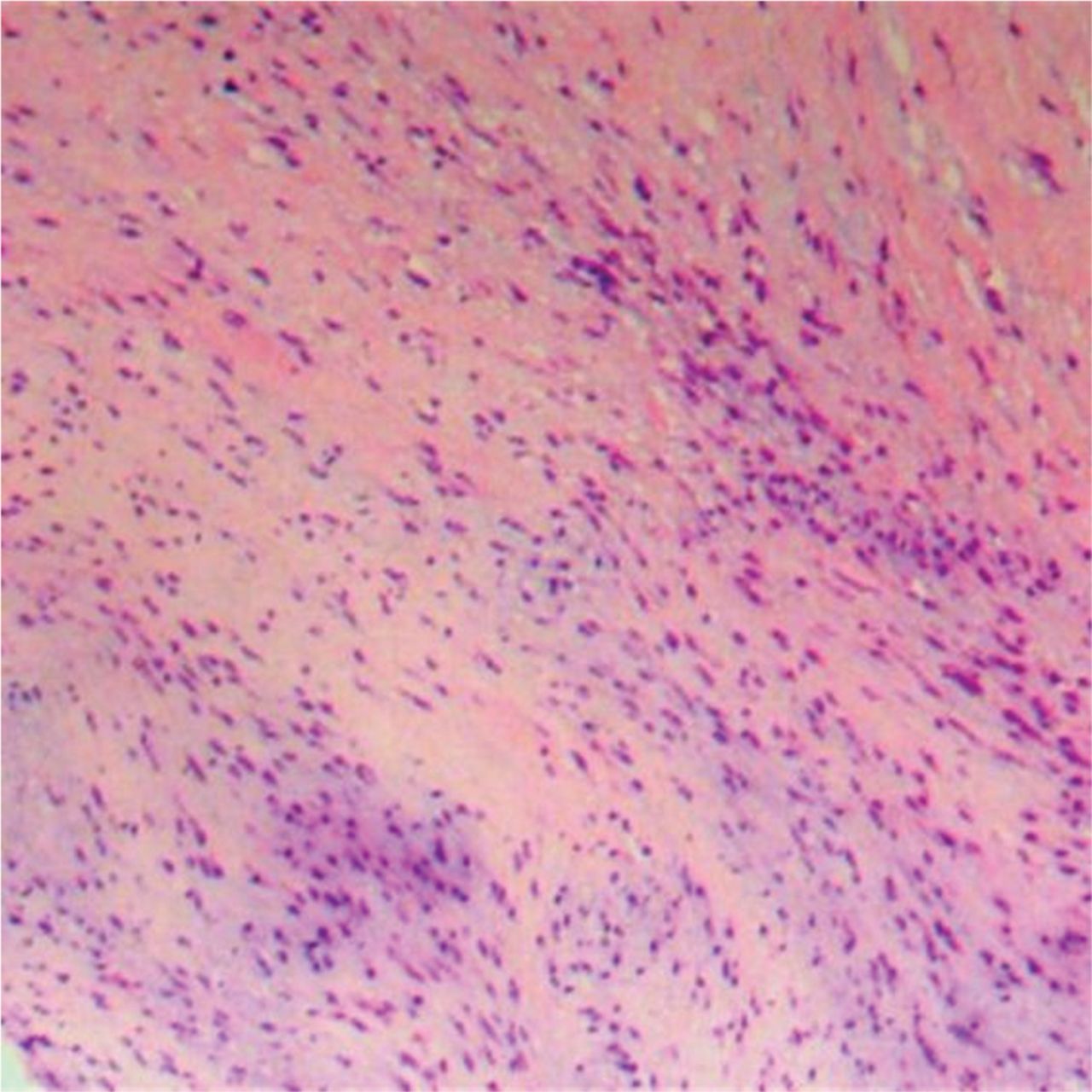
Haematoxylin and eosin staining histopathological slide (×100 magnification) showing that the chordae in the P2 area of the posterior mitral valve is ruptured and accompanied by mucinous degeneration.
Discussion
At present, the requirement of ECMO assistance tends to be more common in patients after heart valve surgery than in patients with rapid disease progression before the surgery.1,2 The patient's condition deteriorated rapidly after admission to hospital, and her respiratory and circulatory systems were difficult to maintain, which were mainly attributable to the fact that the chordae of the mitral valve were ruptured. The majority of such cases are congenital and occur in the posterior lobes. Excessive mucus accumulation in the fibrous layer of the valve eventually led to chordal rupture and MR. The volume load and pressure load of the left atrium (LA) and left ventricle (LV) increased sharply, leading to pulmonary congestion and pulmonary oedema. Meanwhile, the cardiac output decreased, and the blood perfusion of various organs was insufficient. As a result, the patient was treated with ECMO in a timely manner. Interestingly, the patient's imaging finding showed UPO. Echocardiography revealed reverse eccentric blood flow through the LA towards the opening of the right pulmonary vein, which resulted in increased local pulmonary vein pressure and, consequently, UPO. Although the non-physiological retrograde blood flow in the aorta would lead to significant haemodynamic changes, the increase in LV afterload could be controlled by adjusting the extracorporeal circulation flow and the number of vasopressors according to blood pressure and echocardiography.3,4 Therefore, we could create conditions for surgery by reducing pulmonary oedema.
It is reported that UPO accounts for approximately 2% of cardiogenic pulmonary oedema, 90% of which occurs on the right side.5 It is usually caused by a variety of factors, including severe MR, congestive heart failure, left atrial myxoma and thrombosis in the left atrium.6–8 A readily available echocardiography examination (which could reveal valve abnormalities, decreased left ventricular ejection fraction (LVEF), left atrial myxoma etc) is of paramount importance in determining the cause and differential diagnosis. In addition, Doppler echocardiography can show reverse eccentric blood flow of mitral regurgitation. UPO has no specific manifestations such as chest tightness, dry cough, shortness of breath, orthopaedic breathing, palpitations, cyanosis, and even respiratory and circulatory failure. Unilateral cardiogenic pulmonary oedema is often misdiagnosed as pneumonia, aspiration and alveolar haemorrhage due to the main shadow on one side of the lung, causing delays in diagnosis and treatment. Therefore, accurate diagnosis and timely treatment are crucial to reducing mortality.
Key points
UPO is rare and easily misdiagnosed, making the treatment initiation delayed. Therefore, accurate diagnosis and immediate treatment are crucial.
Echocardiography can help patients with UPO to determine the cause and differential diagnosis.
ECMO can provide support for acute heart failure caused by valvular diseases and create conditions for further treatment.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.