
ABSTRACT
One in three deaths of people who are homeless are preventable. The morbidity and mortality of people who are homeless is shocking. With people who are homeless having a higher rate of emergency department attendance and hospital admission compared with the general population, we have a unique opportunity to change their health and their life.
This led to the design and implementation of the Homeless Assessment Tool (HAT) at Gloucestershire Hospitals NHS Foundation Trust. The HAT is an opportunistic prompt to assist doctors in providing the best care for patients who are homeless upon (or during) hospital admission.
Teaching sessions on the health of people who are homeless and the HAT were given to doctors and nurses. Feedback commended the HAT's comprehensiveness, ease of use, and utility in assessing and managing a patient who is homeless.
As such, the HAT is accepted as a standard by the Faculty for Homeless and Inclusion Health, further demonstrating its merits in assessing patients who are homeless.
Introduction
In the UK, there is an ongoing homelessness crisis.
Homelessness refers to rough sleeping, statutory homelessness (households who have approached their local authority when at risk of homelessness) and hidden homelessness (those who do not approach their local authority or are not entitled to help).
At the beginning of 2021, the Ministry of Housing, Communities & Local Government reported that almost 270,000 households were homeless or at risk of becoming homeless.1 This is a staggering 1 in 200 people and does not included the hidden homeless, which Crisis estimates could be an additional 380,000.2,3 A significant number of our population, therefore, live without shelter or the security of it.
With lack of safe shelter comes lack of health. This is seen with the average life expectancy of men being 45 years old and a bleaker expectancy of 43 years old for women.4 In effect, being homeless is a death sentence. This can be understood by the tri-morbidity of homelessness: physical ill health, mental ill health and substance abuse.
As a result, people who are homeless have complex multi-system pathology, with many physical health ailments being much more prevalent than in those that are housed. Forty-one per cent of homeless people have a long-term physical health problem, compared with just 28% in the general population.5 Common conditions (such as asthma, chronic obstructive pulmonary disease, cardiovascular disease, stroke and epilepsy) are more frequent in people who are homeless, in addition to communicable diseases (such as HIV, hepatis B, hepatitis C and tuberculosis (TB)).5,6 There is also a lack of screening and testing, with 65% having not had a sexual health check in the past 12 months and most having not been tested for HIV, hepatitis C or TB.7 Furthermore, a majority have not had their hepatitis A or B vaccinations.7
Beyond physical health, mental health problems in people who are homeless are over twice as high compared with the general population, with 86% of people who are homeless reporting a mental health condition yet only 44% having a formal diagnosis.5,7 People who are homeless are also nine times more likely to take their own lives than the general population, making it the second most common cause of death.8,9
The third part of the tri-morbidity is problematic alcohol or drug use, which is reported in 27% of the population of people who are homeless generally, increasing to over 40% in those specifically that sleep rough.10,11
The aforementioned is a brief summary of only some of the myriad of health needs that our homeless population has. It is, therefore, no surprise that they are 60 times more likely to attend the emergency department (ED) and four times more likely to have an inpatient admission than the general population, with more than 500 rough sleepers being admitted each month.12–14 Admissions for people who are homeless, on average, are longer and cost at least £64 million more than for the same number of the general population per year.13
From this understanding of the vast discrepancy in morbidity and mortality, and that one in three homeless deaths can be preventable with timely medical care, the Homeless Assessment Tool (HAT) was created.15 With people who are homeless far more likely to attend the ED and require hospital admission, we have a unique opportunity to make every contact count and change the health and life of a person who is homeless in under 10 minutes.
Aims
The aims of the HAT were to:
develop and implement a comprehensive assessment tool to streamline and optimise the care of patients who are homeless
deliver teaching on the HAT and assessing patients who are homeless to doctors and nurses in Gloucestershire Hospitals NHS Foundation Trust
demonstrate the benefit of the HAT in improving the care of people who are homeless.
Methods
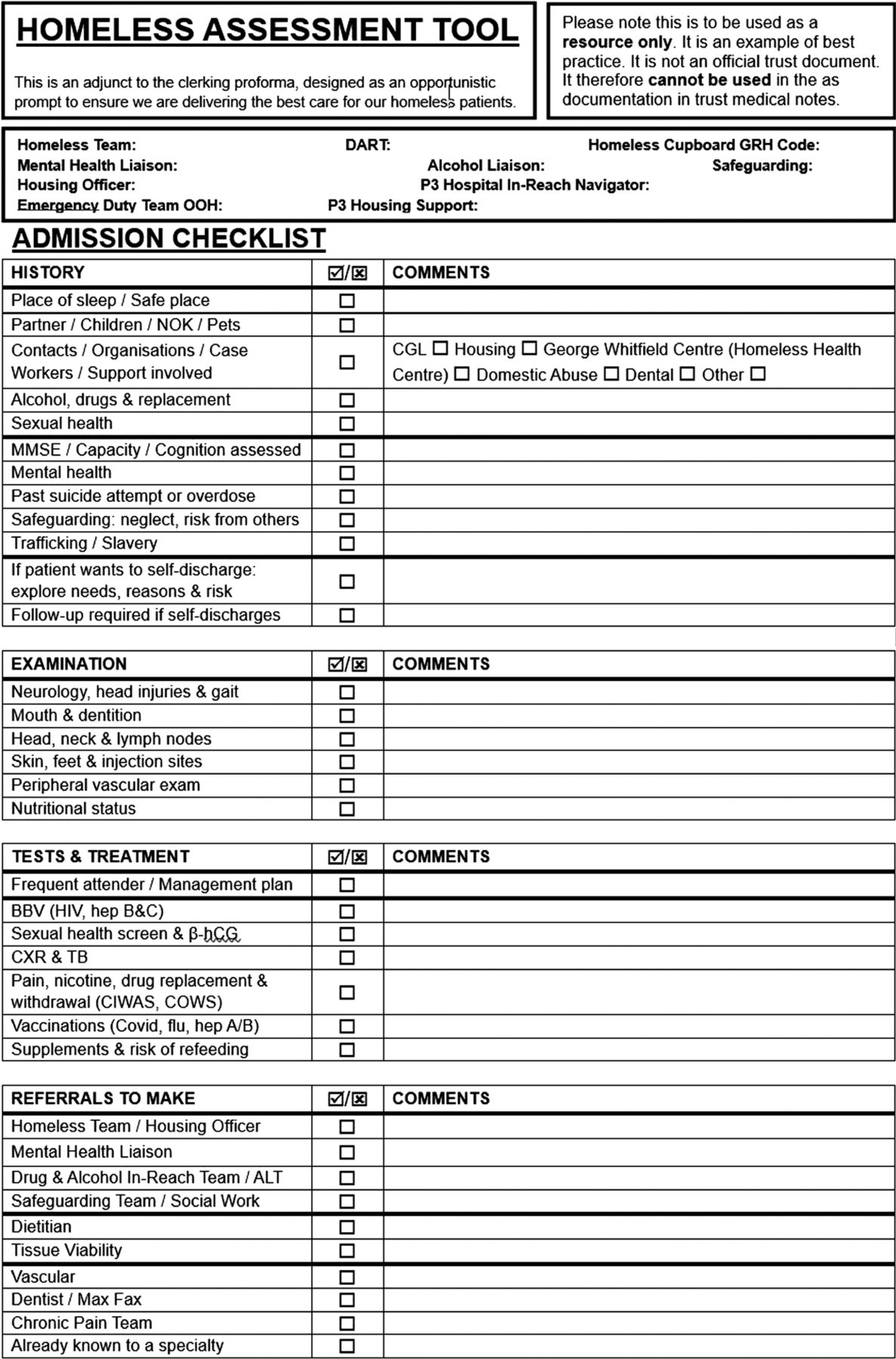
The HAT (Fig 1) is an adjunct to the clerking pro forma, designed as an opportunistic prompt to assist doctors in their clerking of people who are homeless to ensure that we are delivering the best care for our patients who are homeless upon (or during) hospital admission.

The Homeless Assessment Tool developed and used at Gloucestershire Hospitals NHS Foundation Trust.
The HAT is purposely designed to a single side of A4 and is divided into sections pertaining to admission (history, examination, tests and treatments) and relevant referrals to make, followed by tick-box answers and text boxes for elaboration. This aims to identify needs, assessment and action intervention in a systematic way.
The HAT has prompts to ask about alcohol and drugs, with suggestions for replacement and withdrawal, as approximately one-third of our patients who are homeless have problematic use with substances.10,11 Our homeless population has a significant burden of mental ill health, so assessment of mini-mental state exam, capacity and cognition are important as well as detailing previous mental health diagnoses and past overdose attempts or attempts to kill oneself.5,7,8 There are prompts around safeguarding also. As highlighted earlier, a majority have not had blood-borne virus or sexual health checks in the previous 12 months or had their hepatitis A or B vaccinations, so this is covered in the assessment.7 Pointers towards physical examination are included in the HAT to help elucidate vascular disease, head injury, poor dentition, infection, malignancy and nutritional status. The HAT also contains suggestions for referrals to make and provides local hospital and community contact information of the relevant teams regularly associated with the health of homeless people.
At Gloucestershire Hospitals NHS Foundation Trust, we delivered teaching sessions to doctors and nurses about the health of people who are homeless and the HAT, and subsequently rolled it out across the trust. Thereafter, we gathered feedback from the doctors and nurses about the HAT and its utility in clinical practice through a questionnaire.
Results
The feedback from our teaching sessions and the utility of the HAT in clinical practice were overwhelmingly positive.
From the responses received from across the team, 88% stated it was very comprehensive and very easy to follow, being quick and easy to use in practice. Moreover, 94% reported it helped in assessment and management of patients who are homeless, with 100% saying they would use it in their practice of assessing patients who are homeless.
Feedback iterated that the HAT would change their practice in a positive way, commending its holistic and comprehensive content. It was voiced that the HAT should be compulsory practice for healthcare of patients who are homeless and would improve care delivered and address needs that are not immediately obvious. It was emphasised that the HAT should be available on the trust intranet and implemented into our computer system to be used electronically, that lack of access would limit its utility.
Discussion
The feedback we received demonstrates that this is an important piece of work that increases individual knowledge around global assessment of a patient who is homeless, which is currently missing from medical practice.
The HAT has been adopted into the national guidance by the Faculty for Homeless and Inclusion Health, further demonstrating its merits to be used as the standard for assessing patients who are homeless.
We recommend that the HAT is rolled out to trusts across the country to utilise this simple and effective method in delivering comprehensive and holistic care to their homeless population, and adapt it to their local needs and requirements.
Conclusion
The HAT is a comprehensive means of assessing the needs of patients who are homeless at point of entry into hospital.
Feedback has demonstrated the HAT's ease of use and that it can positively impact the care given to patients who are homeless.
Access to this resource is the limiting factor in making this the compulsory standard for assessing patients who are homeless.
Acknowledgements
Thanks to the staff of Gloucestershire Hospitals NHS Foundation Trust for their feedback and implementation of the Homeless Assessment Tool with their ongoing care for all our patients.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}