
ABSTRACT
Visual loss describes temporary or permanent reduction in visual acuity and/or field. Its aetiology is diverse due to the contributions of the different neuro-ophthalmic structures (eye, optic nerve, and brain) to image formation and perception, but may be categorised into ocular causes (corneal, lenticular, vitreoretinal and macular) or optic neuropathies. Clinical evaluation of visual loss relies on thorough history and examination to guide further tests. In this article, we provide a practical overview of visual loss assessment for general physicians.
Key points
Assessment of visual function (acuity, colour vision and field) is the initial step to examining patients with vision loss.
Improvement in visual acuity with pinhole indicates undercorrected refractive error.
Ocular pathologies (corneal, lenticular, vitreoretinal and macular) and prechiasmal optic neuropathies typically cause monocular vision loss.
Urgent ophthalmology discussion is recommended for any patient with reduced vision and recent eye surgeries.
Amaurosis fugax represents ischaemia-related transient monocular vision loss, and must be recognised as it may herald an impending stroke.
Introduction
Visual loss is a serious clinical problem, commonly presenting first to non-ophthalmic healthcare professionals. It typically describes a reduction in visual acuity (sharpness/clarity) or field. This may be acute- or gradual-onset, monocular or binocular and transient or permanent, and may affect central and/or peripheral vision. The work-up for vision loss begins by characterising the nature of visual disturbance, eliciting any associated ocular, neurologic or systemic symptoms, and is followed by clinical examination to guide further tests and investigations. This article provides a brief overview of a practical approach to evaluating visual loss.
Background
The importance of vision to health and quality of life cannot be overstated. Of the different human senses, vision is frequently the most valued.1,2 In fact, participants within a UK-based study would trade off 10 years of life without sight for 4.6 years in perfect health.1 In another US-based nationwide poll, sight loss was deemed worse than life-changing diagnoses such as Alzheimer's disease, cancer and AIDS/HIV.2 Beyond its influence on quality of life, vision loss has indirect repercussions, including productivity losses and costs of informal care.3
Worldwide, the leading causes of blindness in adults over 50 years old are cataract, glaucoma, uncorrected refractive error, age-related macular degeneration (AMD) and diabetic retinopathy.4 These remain the top five causes in the UK, with an estimated 2 million people being blind or partially sighted.3 Among working-age adults in England and Wales, diabetic retinopathy/maculopathy was previously the leading cause of vision loss, but this has been overtaken by inherited retinal disorders.5
Requirements for clear vision
For a clear image, light must pass through clear media (tear film, cornea, aqueous, lens and vitreous) and be refracted by the cornea and lens onto the retina. Photoreceptors (rods and cones) then sense and transmit light as nerve impulses along the optic nerve.
Fibres from nasal hemiretinae (temporal visual field (VF)) decussate at the optic chiasm and join the contralateral optic tracts, whereas fibres from temporal hemiretinae (nasal VF) join ipsilateral optic tracts. As such, optic tracts carry fibres from contralateral visual fields.
Optic tracts synapse at ipsilateral lateral geniculate ganglia within the thalamus before continuing as optic radiations. Parts of the inferior optic radiations (contralateral superior quadrant VF) loop around the temporal horn of lateral ventricle (Meyer loop), whereas superior optic radiations pass through parietal lobes to arrive at primary visual cortices along calcarine fissures within the occipital lobes.
Due to the contributions of the different neuro-ophthalmic structures (eye, optic nerve and brain) to image formation and perception, the aetiology of vision loss is diverse but can be divided into ocular causes (eg corneal, lenticular, vitreoretinal and macular) and optic neuropathies (Table 1).
Differential diagnoses for vision loss
Key points in history taking
Monocular versus binocular visual loss
Monocular visual loss is typically caused by ocular pathologies or prechiasmal optic neuropathy unless the underlying disease affects both eyes; for instance, systemic conditions (eg diabetic macular oedema, malignant hypertension and nutritional optic atrophy) and inherited diseases (eg retinitis pigmentosa).
Binocular visual disturbance should raise a suspicion of chiasmal, retrochiasmal or other intracranial pathologies causing raised intracranial pressure (ICP) and papilloedema. Due to the retinotopic organisation within the visual pathway, the nature of VF loss may localise the lesion. In particular, bitemporal hemianopia is classically caused by chiasmal lesions, whereas homonymous field loss (congruent VF loss in both eyes) indicates retrochiasmal lesions; for example, temporal lobe lesions compressing Meyer loop may cause contralateral superior homonymous quadrantanopia (‘pie in the sky’ VF defect).
Central versus peripheral vision loss
Poor central vision sparing the peripheries indicates macular involvement. Macular diseases (eg AMD and central serous chorioretinopathy) may manifest as distortions (straight lines appearing wavy or warped) or paracentral scotoma (dark spots at central vision). The Amsler grid can be used to characterise this further.
Constricted peripheral vision is usually caused by optic neuropathy; the magnitude of field loss may be subtle and only detected during screening (eg chronic glaucoma), or large and cause difficulties with navigation (eg frequently bumping into things due to bitemporal hemianopia). Although uncommon, retinal causes of tunnel vision, such as retinitis pigmentosa or extensive bilateral panretinal photocoagulation, should also be considered.
Speed of onset
Speed and duration of onset may reflect the underlying pathophysiological processes. Vascular occlusions of retinal, optic discs or cerebral vessels usually cause rapid-onset vision loss. Inflammatory processes such as optic neuritis or scleritis generally cause subacute visual reduction over days. Degenerative processes (such as cataract) typically cause gradual-onset visual impairment, but the disturbance may not be realised in the early stages. In addition, serious insidious pathologies (eg compressive optic neuropathy from an intracranial mass) could cause slowly progressive visual loss.
Transient visual disturbance
Transient monocular visual loss (TMVL) is a worrying symptom, especially in older individuals with cardiovascular risk factors, as it could be ischaemic in origin (amaurosis fugax), heralding an impending stroke. Classically, TMVL in amaurosis develops in a downward curtain-like manner and lasts 2-30 minutes with an upward resolution. However, other patterns have been described.6
Amaurosis fugax typically results from temporary ischaemia caused by embolism originating from the carotid circulation, but may occur in chronic vascular insufficiency secondary to severely stenotic internal carotid artery (ocular ischaemic syndrome). In the latter, amaurosis may be induced by light, exertion or change in posture.7 Other causes of TMVL are giant cell arteritis, impending central retinal vein occlusion and retinal migraine. An important differential for TMVL is migraine-associated visual aura. This presents as episodic zig-zag lines or scotoma, lasts 5-60 minutes and typically, but not always, precedes the headache; its slow and gradual development is a key feature, differentiating it from ischaemia-related causes eg transient ischaemic attack.8
For transient binocular disturbance, the precipitating and relieving factors are clues to the underlying causes. Transient visual obscurations in papilloedema are brief binocular visual blurriness or darkening lasting for a few seconds and precipitated by bending forward or lying down (or any actions that increase ICP). Transient blurry vision on standing up may be related to postural hypotension. Frequent episodic blurry vision that clears with blinking may be due to ocular surface diseases that disrupts the air-tear film interphase.
Ocular pathology or optic neuropathy?
A useful framework to narrow the differentials is to determine if vision loss is secondary to ocular or optic nerve pathologies. A thorough history may identify those with ocular pathologies (Table 2); for instance, vision loss preceded by floaters and photopsia (brief sudden and flash-like) could be related to posterior vitreous detachment causing retinal detachment (Fig 1). Blurry vision in someone with severely painful red eye could be due to corneal ulcers, acute angle-closure glaucoma, scleritis or other ocular problems. However, most retinal causes of vision loss are painless and do not cause other symptoms; the diagnosis is based on the clinical appearance.
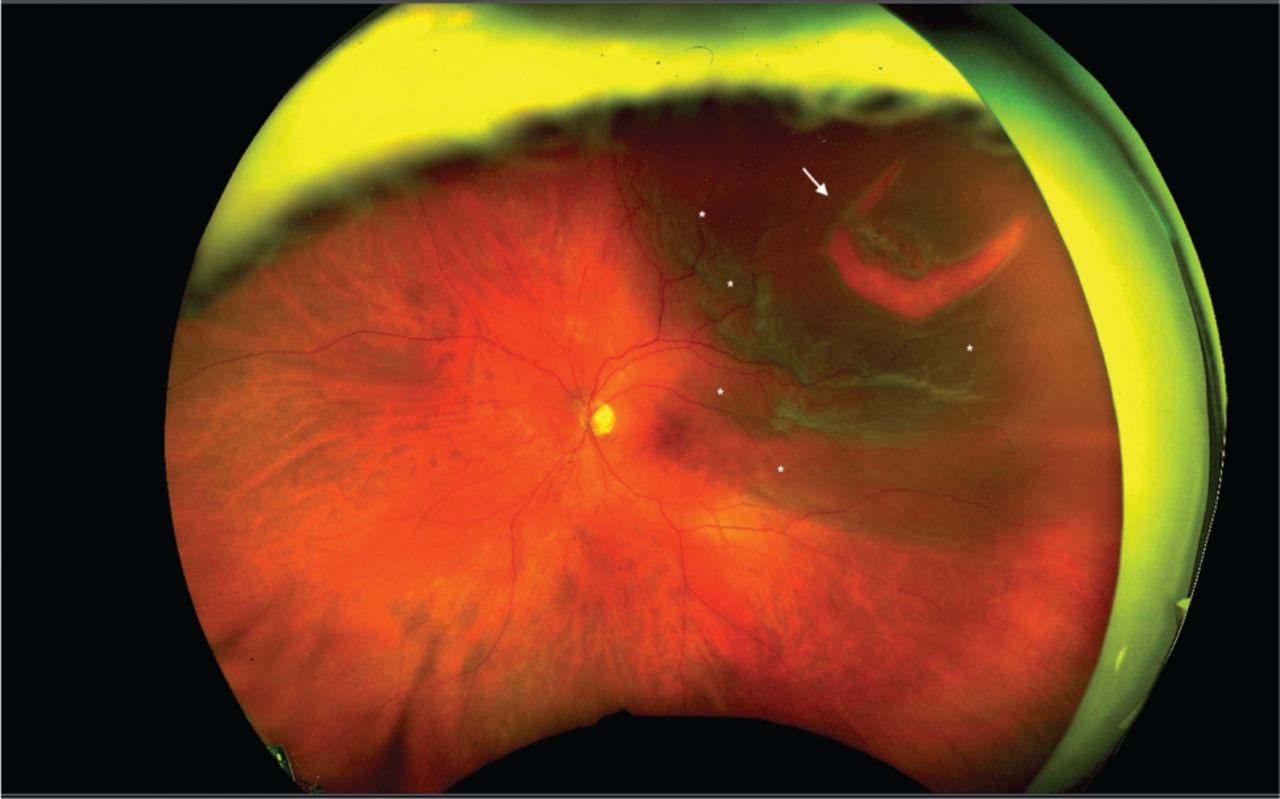
Macula-off rhegmatogenous retinal detachment in a 65-yearold man presenting with monocular visual reduction preceded by floaters and photopsia. Horseshoe-shaped tear (white arrow) is noted in superotemporal quadrant, with surrounding subretinal fluid (asterisks).
Salient points in the history taking when assessing vision loss
The identification of optic neuropathy is also largely clinical: dyschromatopsia, relative afferent pupillary defect (RAPD) and characteristic VF defect. The underlying cause may be obvious, eg orbital cellulitis, thyroid-associated ophthalmopathy or trauma (suspected retrobulbar haemorrhage). If not, the optic disc appearance (swelling or pallor) will focus subsequent work-up (Table 1). Of note, giant cell arteritis, non-arteritic anterior ischaemic optic neuropathy and optic neuritis (eg multiple sclerosis) are frequent causes of optic disc swelling.
Assessment of visual function
Prior to examining the eye, visual function deficits should be established. Visual function includes distance and near acuity, colour vision and visual field. Measuring distance visual acuity (VA) using standardised charts (eg Snellen and logMAR) is the key initial step to quantifying visual deterioration. Each eye needs to be tested separately, unaided, with glasses and with pinhole occluder. VA improvement with pinhole suggests a degree of undercorrected refractive error. In infants and toddlers, the inability to fix and follow a target, or aversion to occlusion of one eye more than the other, may be indicative of poor vision.
Near vision can be crudely evaluated using small prints, but this is rarely useful in non-ophthalmic settings. Using a red object and comparing each eye in turn may assess for red desaturation (colour appearing pink or ‘washed out’). If available, colour vision can be quantified using Ishihara charts. The presence and location of VF deficits can be determined by the confrontation method. Formal perimetry testing may be subsequently required for monitoring progression and to assess driving eligibility.
Essential eye examinations
Eye examination starts by inspecting the eyelids (for cellulitis, lid retraction or ptosis), globe position (for proptosis or enophthalmos) and eye movements (for restricted or painful extraocular movements). The conjunctiva and sclera are then examined for any generalised, sectoral or circumcorneal injection. Ten per cent phenylephrine will blanch episcleritis but not scleritis.
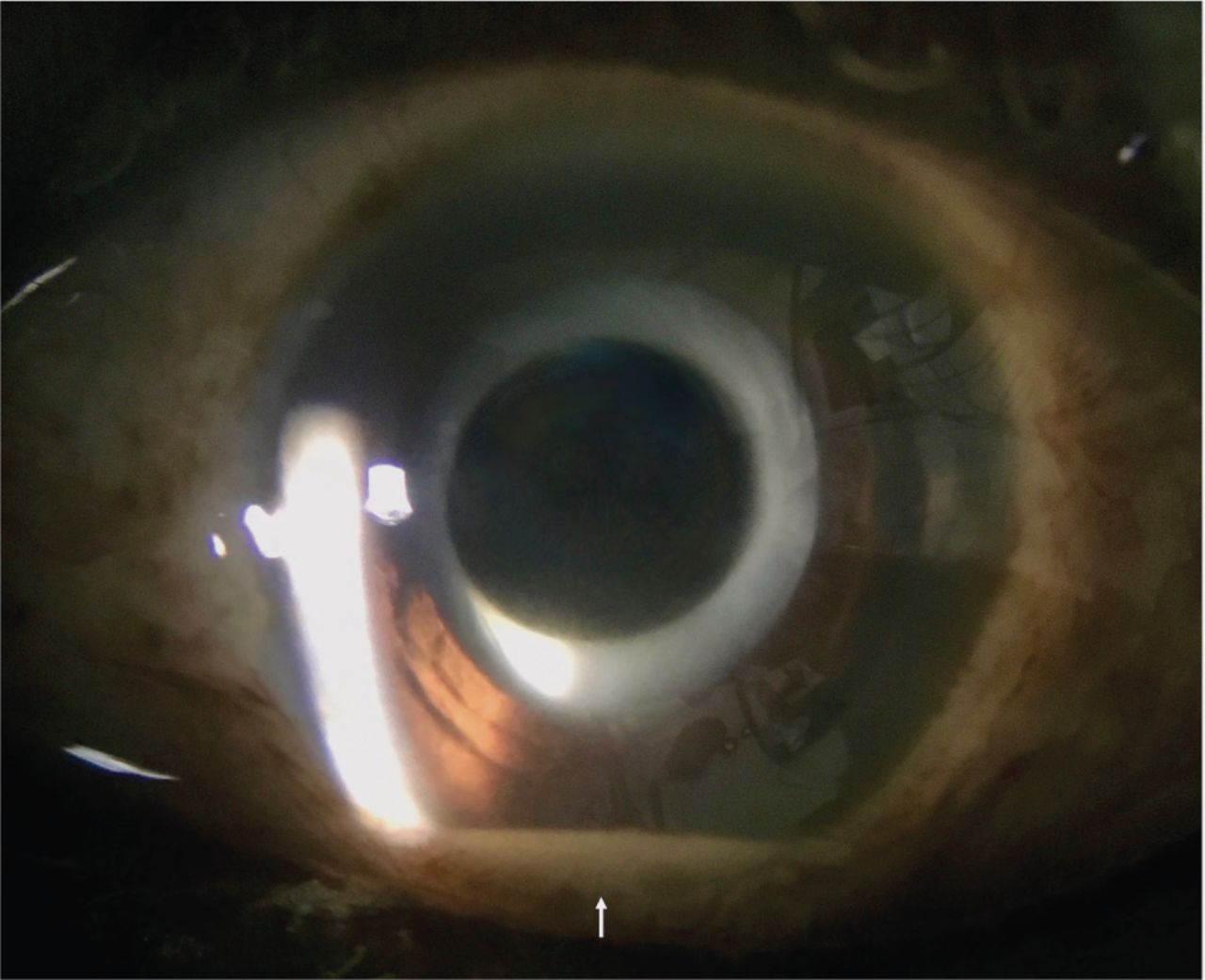
The cornea is best visualised using a slit lamp. However, any focal opacities, foreign bodies or generalised haziness impairing VA are usually readily noticeable. Fluorescein staining can further highlight any epithelial defect under blue cobalt light, available on most handheld ophthalmoscopes. Macroscopic build-up of red cells (hyphaema) or white cells (hypopyon) is also easily noticeable without a slit lamp (Fig 2).
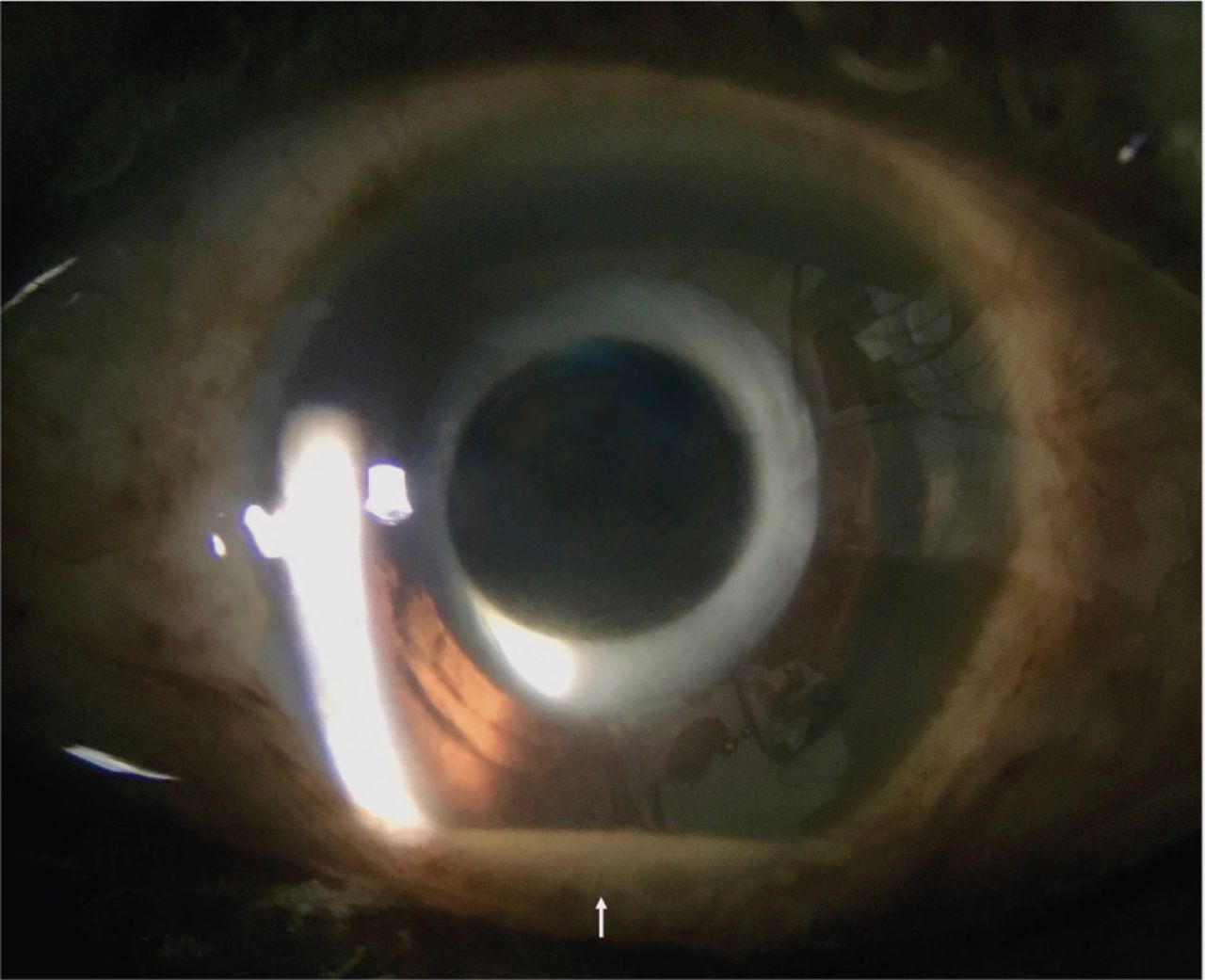
Hypopyon (white arrow) in the anterior chamber in a patient with recent intravitreal injection.
Next, pupils should be assessed for size asymmetry and response to light. Red reflex should be examined for leucokoria (eg retinoblastoma) in children and media opacity (eg dense cataract or vitreous haemorrhage) in adults.
Finally, the retina and optic discs can be examined using an ophthalmoscope; the view can be improved with pharmacological dilation, eg using cyclopentolate. The optic disc should be examined for its cup-to-disc ratio, colour and contour.
Referring to ophthalmology
Although the majority of eye presentations to the emergency department can be managed without ophthalmic input, vision loss warrants discussion with ophthalmology especially for those with recent eye surgeries.9 Further examination and tests (such as optical coherence tomography, ultrasound and electrodiagnostics) may be required.10,11 Neuroimaging is necessary in certain cases eg suspected compressive or demyelinating optic neuropathy and bilateral optic disc oedema. In the absence of organic disease, functional visual disturbance should be considered.12
Conclusion
In summary, vision loss can be caused by ocular or optic nerve pathologies. Its initial evaluation can be done well without any sophisticated equipment. While non-ophthalmologists may not always reach a firm diagnosis, a thorough initial assessment is key to determining the urgency of referral.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.