
ABSTRACT
Objective To determine the maximal response of the temperature and inflammatory response to SARS-CoV-2 infection and how these are modified by age.
Methods Participants were patients admitted to hospital with SARS-CoV-2 infection. For each participant, the maximal temperature and serum C-reactive protein (CRP) were identified and stratified by age. In a secondary analysis, these were compared in patients treated before and after dexamethasone.
Results Mean maximal temperature varied by age (p<0.001; ANOVA) with the highest mean maximal temperature of 37.3°C observed in patients aged 30–49 years and decreasing maximal mean temperatures in the older age groups, with the lowest measure of 36.8°C observed in individuals aged 90–99 years. The mean maximal serum CRP also varied across age groups (p<0.001; ANOVA) and increased with age across all age categories from 34.5 mg/dL (95% confidence interval (CI) 22.0–47.0) for individuals aged 20–29 years to 77.6 mg/dL (95% CI 72.0–83.2) in those aged 80–89 years. After dexamethasone became standard treatment for COVID-19 pneumonia, mean maximal CRP decreased by 17 mg/dL (95% CI −22 to −11).
Conclusion Age modifies both maximal temperature and systemic inflammatory response in patients with SARS-CoV-2 infection.
Introduction
One of the strongest prognostic factors for many diseases is age, and this is used by clinicians in selecting the most appropriate management for individual medical conditions. However, the processes by which age modifies the natural history of diseases is poorly understood. Awareness of the mechanisms by which age can modify the biological response to diseases (such as infection) may help in the interpretation of normal values and the development of new strategies of managing these conditions. Approval for this work was granted via an Nottingham University Hospitals NHS Trust (NUH) Clinical Effectiveness Team audit (reference 20-153C), the NUH Caldicott guardian, data protection impact assessment (reference 436) and, as a research study, ethics approval via the NHS Health Research Authority (HRA) Integrated Research Application System (IRAS) (reference: 282490). The HRA confirmed that individual patient consent was not required for this work.
One example of how age can modify response to infection was observed during the Spanish influenza epidemic from 1918 to 1920. This caused approximately 50 million deaths globally, with approximately half occurring in younger adults aged 20–40 years old.1 One hypothesis to explain this age differential in mortality is that younger adults experienced a more vigorous immune response to infection with this strain of virus, resulting in a more severe clinical scenario compared with older individuals.1 Very little data exist to substantiate this theory, although clinical observation in older individuals suggest that parameters (such as temperature) may not be elevated in the context of acute infection, leading to delays in diagnosis and treatment.2
The science of ageing is very broad, but one area that has developed over recent decades is the concept of immunosenescence, which encompasses the understanding of how the immune system changes throughout the life course.3 This is prompted by observations that, as individuals age, they become more susceptible to infectious disease and have diminished responses to vaccination, as well as a number of diseases that may have an immunological component, including cardiovascular disease, neurodegenerative disorders, the concept of frailty and cancer.4,5
The COVID-19 pandemic allows the impact of age on maximal physiological parameters and systemic biomarkers in response to a single-agent viral infection to be explored in detail. We have tested the hypothesis that the maximal temperature and systemic inflammatory response to SARS-CoV-2 infection vary with age using data from a cohort of patients admitted to a teaching hospital with SARS-CoV-2 infection in 2020. This spanned a timeframe that began when dexamethasone was not routinely used for these patients and continued into the period when the use of corticosteroids became standard therapy for managing COVID-19 pneumonia, we also examined how these parameters varied over these two distinct time periods as a secondary outcome.6
Method
The study population consisted of patients admitted between 01 February 2020 and 31 December 2020 with either clinically diagnosed or PCR confirmed SARS-CoV-2 infection.
Vital signs were recorded electronically using NerveCentre (http://nervecentresoftware.com), and C-reactive protein (CRP)and neutrophil measurements are automatically uploaded to the hospital data warehouse. Maximum values for each individual were calculated across their hospital admission stratified by 10-year age bands in the 60 days after the date first suspected of SARS-CoV-2 infection. The main hypotheses of interest were that maximal temperature and systemic inflammation (as measured by serum CRP) responses would be lower in higher age groups. We also utilised all available data to explore how age modified the maximal systolic and diastolic blood pressure, heart rate and blood neutrophil responses as secondary outcome measures.
The press release providing evidence for supporting the use of dexamethasone in hospitalised patients with SARS-CoV-2 infection was released 16 June 2020.7 We therefore plotted the differences in the average maximum measurements from before and after this date, and tested the significance of the differences date (16 June 2020) using linear regression adjusting for age.
Results
Temperature and CRP measurements were available from 3,484 individuals with a median age of 74 years (interquartile range (IQR) 57–84) and, of whom, 1,815 (52%) were male patients. There were 188,702 individual temperature measurements and 15,001 serum CRP measurements available for analysis.
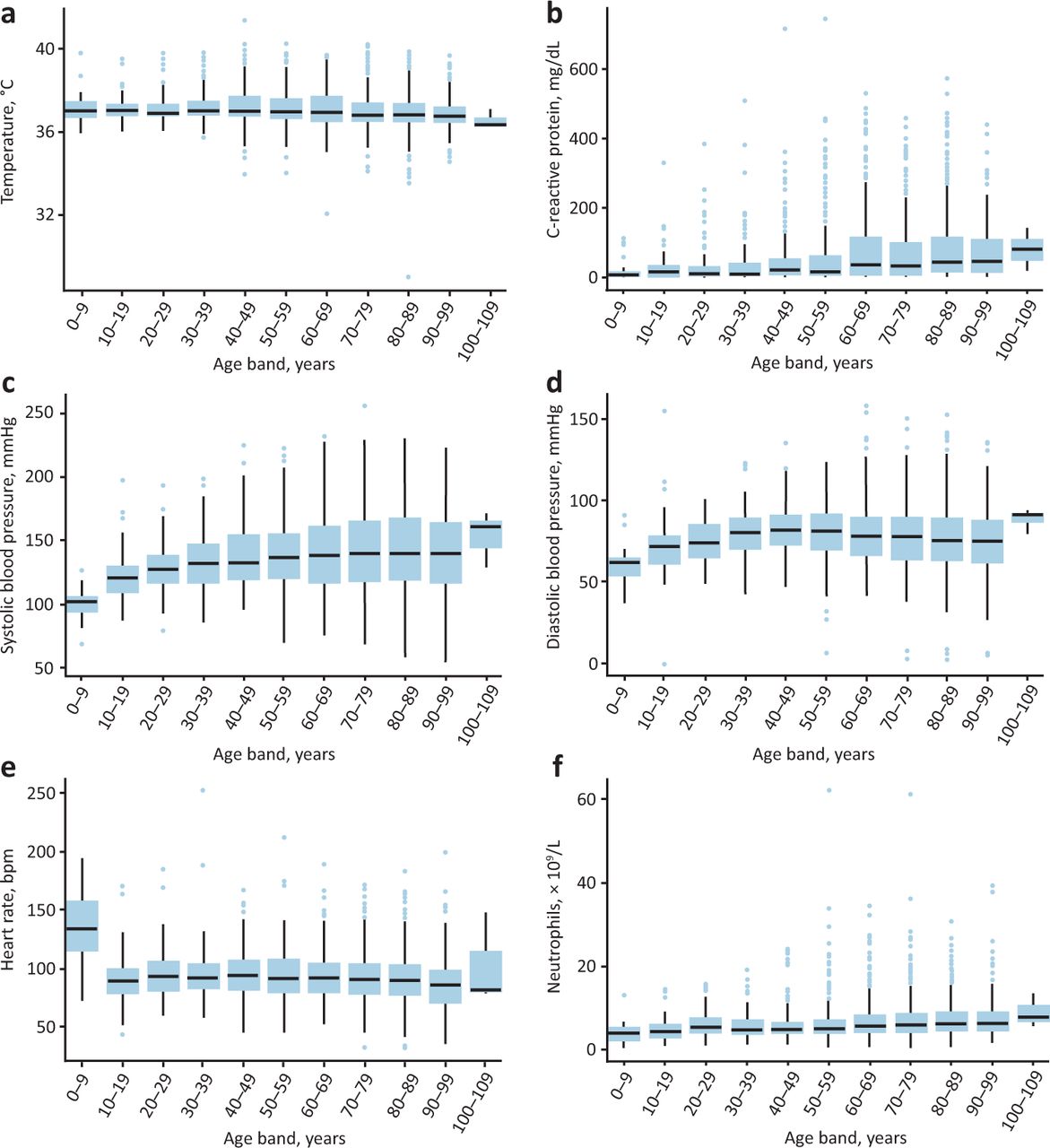
The mean maximum values of temperature, serum CRP, systolic and diastolic blood pressure, pulse, and blood neutrophils for each patient all varied by age (p<0.0001 for all measures; ANOVA) and are presented in Table 1. The distributions of the maximum measured values stratified by 10-year age bands are presented in Fig 1. Maximal mean temperature was highest in adults aged 30–39 years (37.4°C; 95% confidence interval (CI) 37.1–37.7) and 40 to 49 years (37.3°C; 95% CI 37.2–37.4) and decreased with increasing age to a lowest value for the age range 90–99 years (36.8°C; 95% CI 36.8–36.9).

Distributions of patients by 10-year age bands, in maximum per patient. a) Temperature. b) C-reactive protein. c) Systolic blood pressure. d) Diastolic blood pressure. e) Heart rate. f) Neutrophils.
Maximal clinical and systemic inflammatory responses stratified by age
Maximal serum CRP increased with age from 34.5 mg/dL (95% CI 22.0–47.0) for 20–29 years to 77.6 mg/dL (95% CI 72.0–83.2) for 80–89 years.
After dexamethasone became a standard treatment for COVID-19 pneumonitis, there was a decrease in the mean maximal CRP of 17 mg/dL (95% CI −22 to −11) compared with the pre-dexamethasone era and adjusting for age. There was no change in mean maximal temperature (−0.002°C; 95% CI −0.07 to 0.01) during the dexamethasone era compared with the pre-dexamethasone era (Table 2).
Maximal temperature and serum C-reactive protein responses stratified by age before and after dexamethasone was introduced into the management of SARS-CoV-2 infection
Discussion
This is the first study to explore the maximal physiological and systemic inflammatory response in a cohort of patients admitted to hospital with SARS-CoV-2 infection. The data demonstrate that age is a factor that modifies both maximal temperature and maximal systemic inflammatory response to SARS-CoV-2 infection, with the higher temperatures being observed in the age groups from 30 to 49 years, and the maximal systemic inflammatory response as measured by serum CRP and blood neutrophils increasing with age. The introduction of dexamethasone as a standard treatment for COVID-19 pneumonia was associated with a decrease in maximal serum C-reactive protein as would be expected from an anti-inflammatory medication.
The strengths of these data include that it represents every patient admitted to NUH with SARS-CoV-2 infection during the data collection dates, and hence there is no risk of bias due to differentials in recruitment. As all patients experienced infection by the same organism, this provides a homogeneous population in which the body's response can be stratified by age, both before and after the date of the introduction of dexamethasone to the standard treatment for SARS-CoV-2 infection.6 The data are from real-world healthcare data and are sourced from the routinely collected clinical observations that are generally measured every 6 hours on most patients, although can be done more or less frequently depending on the clinical scenario.
As observational analyses, there are some limitations that warrant consideration. Older patients with less severe SARS-CoV-2 infection but more comorbidities may have an increased risk of being admitted as a precaution or as a consequence of an absence of carers in their home environment. If older patients have lower risk of escalation, there may be a tendency to do fewer blood tests, which may limit the number of samples of blood neutrophil count and CRP taken, hence potentially biasing the results from the differentials in blood sampling frequencies across age groups. However, the increasing trend in mean maximum systolic and diastolic blood pressures with increasing age is as would be expected from our knowledge of risk factors for hypertension, and hence gives confidence in the validity of these data. Finally, we had no prescribing data on the use of dexamethasone in individual patients, and had to use the date of the press release from the RECOVERY trial to delineate the period when dexamethasone was introduced into the standard management of patients with COVID-19 pneumonia to generate a proxy measure of dexamethasone exposure.7 This may introduce some measurement error as some of these patients may have had mild disease and not been prescribed dexamethasone. However, the fact that we observed a change in the maximal serum CRP suggests that there was an impact of corticosteroids on these parameters, and any measurement error of this exposure could lead to an underestimate of the true size of effect as a consequence of regression dilutional bias.8
These data give an insight into the biological response to infection by a single pathogen and how it may be modified by both age and dexamethasone. The mean maximal temperature was seen in individuals aged 30–49 years old, decreasing for older age categories. The maximal serum CRP did not show such a plateau trend but continued to rise with age. This is consistent with age as a risk factor for severity and mortality from SARS-CoV-2 infection, and serum CRP is also an independent prognostic marker for mortality from SARS-CoV-2 infection.9,10 Thus the maximal temperature and maximal serum CRP response are responding to SARS-CoV-2 infection differently across the age categories.
The secondary analysis of maximal temperature and serum CRP responses over the two periods represent the times when dexamethasone was not a treatment for COVID-19 pneumonia and also the period after it was discovered to be efficacious in reducing mortality.6 This demonstrated that there was a decrease of maximal serum CRP of 17 mg/dL after dexamethasone treatment for COVID-19 pneumonia was established, which reflects the anti-inflammatory action of corticosteroid therapy, but no change in maximum temperature.
These data contribute to our understanding of how age modifies the clinical response to infection and complement scenarios that clinicians have regularly observed in daily practice throughout the COVID-19 pandemic. As such, they provide clinical data to inform the new science of immunosenesence, which represents the understanding of how the immune system changes with ageing, and is considered to be a consequence of the progressive decline in the innate and adaptive immune responses.3,4 Our data suggest that there is a less vigorous response in the facets of the immune system that increase temperature in older individuals, yet, despite this, the blood inflammatory response as measured by CRP and neutrophil levels is stronger than in younger patients. The CRP response is attenuated by dexamethasone, as expected for a systemic inflammatory response. To reconcile these observations, it is necessary to consider that the immune response to infection is multifaceted, and not a single entity, with separate pathways that can be expected to change with age differently. Future studies of these processes at the immunological cellular level are important, as they may open new opportunities to modify the immune response in the elderly improving defences to exogenous infection.
Conclusion
Both maximal temperature and serum CRP levels are modified by age in a cohort of patients with SARS-CoV-2 infection, thus demonstrating two ways by which age can modify the host response to infection. After the introduction of dexamethasone to the treatment options for COVID-19 pneumonia, maximal systemic inflammation measures decreased.
Summary box
What is known?
Ageing may modify the host response to infection in the clinical setting, but little standardised data exist.
What is the question?
Does the body's response to SARS-CoV-2 infection vary with age?
What was found?
Mean maximal temperature of patients admitted to hospital with SARS-CoV-2 infection decreased in older patients.
Mean maximal serum C-reactive protein (CRP) increased with age in patients admitted to hospital with SARS-CoV-2 infection.
When dexamethasone was introduced as a standard therapy for SARS-CoV-2 infection, mean maximal serum CRP decreased by 17 mg/dL compared with when dexamethasone was not used to treat SARS-CoV-2 infection.
What is the implication for practice now?
This report suggests that there are a wide range of host responses to infection that are modified by age. In particular, in older people, the absence of a rise in temperature does not exclude infection.
Funding
Joanne R Morling receives salary support from the Medical Research Council (grant number MR/P008348/1).
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}