
Abstract
Accelerated coronary artery disease seen following radiation exposure is termed ‘radiation-induced coronary artery disease’ (RICAD) and results from both the direct and indirect effects of radiation exposure. Long-term data are available from survivors of nuclear explosions and accidents, nuclear workers as well as from radiotherapy patients. The last group is, by far, the biggest cause of RICAD presentation.
The incidence of RICAD continues to increase as cancer survival rates improve and it is now the second most common cause of morbidity and mortality in patients treated with radiotherapy for breast cancer, Hodgkin's lymphoma and other mediastinal malignancies. RICAD will frequently present atypically or even asymptomatically with a latency period of at least 10 years after radiotherapy treatment. An awareness of RICAD, as a long-term complication of radiotherapy, is therefore essential for the cardiologist, oncologist and general medical physician alike.
Prior cardiac risk factors, a higher radiation dose and a younger age at exposure seem to increase a patient's risk ratio of developing RICAD. Significant radiation exposure, therefore, requires a low threshold for screening for early diagnosis and timely intervention.
Introduction
The incidence of cancer is continually increasing worldwide. In 2018, there were 18.1 million new cancer cases, and this figure is predicted to rise to 29.5 million by 2040.1 With 50% of oncology patients requiring radiotherapy at some point in their treatment course, the cohort of post-radiotherapy patients is steadily increasing.2 Improving outcomes following treatment has created a paradigm shift in the aims of treatment away from the short-term view of ‘curing’ cancer and towards a goal of long-term survival.
Historically, the risks of significant radiation exposure have been apparent both through nuclear warfare (such as from the atomic bombs dropped on Hiroshima and Nagasaki in 1945 that killed between 150,000 and 200,000 people, collectively) as well as the Chernobyl accident in Ukraine in 1986 where 60,910 emergency workers were exposed to significant radiation doses.3,4 Survivors of the Chernobyl accident were found to have an excess relative risk of coronary artery disease (CAD) at 0.42 per Gy of radiation (95% confidence interval (CI) 0.05–0.78).4 The outcomes of survivors of nuclear attacks and accidents provided initial evidence that, even in a comparatively young and otherwise healthy population, the risk of CAD was dramatically increased following significant radiation exposure.
Fortunately, few clinicians may ever see or treat a patient exposed to radiation from a nuclear event. However, patients treated for malignancies of the mediastinum, thorax and upper abdomen have been demonstrated to be at an increased risk of cardiovascular disease with a relative risk of greater than 2.4 times that of the general population.5 This represents the leading cause of non-malignant tumour-related death, which increases over time for almost all cancer survivors and is an important risk factor to note for the oncologist when offering and consenting patients for radiotherapy treatment.3 It is also important for the general medical physician interacting with the patient at multiple stages in their cancer journey and for many years after their successful treatment.
Manifestations of radiation-induced cardiac toxicity include pathology of the pericardial, myocardial, autonomic, valvular and conduction systems as well as the distinct entity of accelerated CAD that has been termed radiation-induced coronary artery disease (RICAD). RICAD generally occurs with a latency period of 15 years post-radiation exposure by which time many patients will already have completed their oncology follow-up and would be increasingly likely to present to a general medical physician or general practitioner (GP).6 This represents a significant challenge to these services as RICAD can often present silently and requires a high index of clinical suspicion. Therefore, it is no surprise that RICAD is the second most common cause of morbidity and mortality in patients treated with radiotherapy for breast cancer, Hodgkin's lymphoma and other prevalent mediastinal malignancies.7 Another challenge is that this cohort of patients has both a possible higher risk of in-stent restenosis as well as a higher risk of adverse surgical outcomes. Challenges to coronary artery bypass grafting (CABG) surgery include an increased risk of mediastinal fibrosis, which can be extensive, as well as damage to the mammary arteries rendering them unsuitable for harvesting. A reduced rate of success of pericardiocentesis for cardiac tamponade has also been observed.8
Although guideline statements relating to RICAD are relatively limited from both the American Heart Association and European Society of Cardiology (ESC), there is an increasing appreciation of the value of long-term follow-up in this patient group.9,10 The latest ESC guidelines emphasise the critical importance of effective strategies for both prediction and prevention of cardiovascular toxicities for cancer patients.11
The purpose of this review is to improve the understanding and awareness of RICAD that is increasingly relevant to the oncologist, the cardiologist and, ultimately, the general medical physician alike.
Radiotherapy
The risk of RICAD is dependent on the area to which radiotherapy is directed. Following mediastinal radiotherapy treatment for Hodgkin's disease (which involves one of the largest doses of radiotherapy close to the heart), cardiovascular causes are the third most common cause of death and account for 12%–16% of mortality with a four-to-seven-fold increased risk of CAD compared with the general population and a cumulative CAD incidence of up to 50% at 40 years after treatment. Furthermore, the risk of myocardial infarction (MI) is increased two-to-seven-fold compared with the general population, with a cumulative incidence of 10% at 30 years in those receiving radiotherapy doses of 10–40 Gy.12
Darby et al demonstrated the relationship between radiation dose and the risk of CAD in a group of patients receiving radiotherapy for breast cancer (which is one of the most common indications for radiotherapy in the chest).13 Mean doses of radiation to the heart from radiotherapy for breast cancer was typically 1 or 2 Gy for disease of the right breast and 10 Gy for disease of the left breast. The average dose to the whole heart was 4.9 Gy (range 0.03–27.72) with major coronary events increased linearly by 7.4% per Gy.13 Furthermore, the rates of death from CAD were found to be six times higher in those treated with radiotherapy at an age of less than 50 years and doubled for those treated with radiotherapy after the age of 70 years.13 An increased risk in those irradiated when young is likely due to the late effect of radiation, and an increased time to manifest and longer to live with the inflammation. It was noted that patients treated with radiotherapy with one or more cardiac risk factors had an increased absolute risk of death from CAD of 0.7% and an absolute risk increase of an MI of 1.7% compared with those without cardiac risk factors.13
As well as patient cohorts receiving mediastinal radiotherapy for Hodgkin's lymphoma and breast cancer, there is also emerging evidence associated with oesophageal and lung cancer (which are other chest radiotherapy targets). Frandsen et al analysed cardiovascular mortality after radiotherapy for oesophageal cancer noted patients with mid-oesophageal lesions were at highest risk and overall concluded that for all patients receiving radiotherapy, death from heart disease occurred at 1.46 times the rate of those not receiving radiotherapy.15 Ming et al also noted that the incidence of cardiac complications in patients receiving radiotherapy for lung cancer was elevated at 33% and noted that a high prevalence of smoking was also a significant pre-existing risk factor, however, it should be noted that their data set included 2D radiotherapy where the doses to the heart were much higher as compared with the modern radiotherapy techniques.16 Nevertheless, smoking is a significant modifier for CAD risk and needs to be addressed by clinicians in these patients.
Pathophysiology and inflammatory pathways associated with RICAD
Pathophysiological mechanisms of RICAD include dysfunction of the endothelium, reduction in capillary density, acceleration of atherosclerosis, and fibrotic changes involving both the coronary macrovasculature and microvasculature. In the acute phase, the rapid formation of a large proportion of reactive oxygen species (ROS) as a result of radiation exposure is a key mechanism causing vascular damage.17 An imbalance in the cell antioxidant system with excessive ROS overwhelms the cell antioxidant defense system leading to oxidative damage to cell structures including DNA, lipids and proteins.17 Nuclear factor kappa B, an inducible transcription factor, is usually bound to an inhibitor protein, however, exposure to radiation liberates nuclear factor kappa B to bind to numerous target genes. Binding of nuclear factor kappa B induces transcription of pro-inflammatory enzymes such as COX-2 and 5-LPO, which are key sources of on-going ROS generation. Therefore, a positive feedback loop is formed between excessive ROS and their activation of nuclear factor kappa B to switch the cell into a continual state of excessive ROS production further promoting cardiovascular damage.17
Excessive ROS also leads to an acute inflammatory response with release of monocyte chemotactic factor, tumor necrosis factor, and interleukins (IL) 1, 6 and 8, resulting in the recruitment of neutrophils to the damaged areas. This response is similar to the atherosclerotic process and is a key component in the development of RICAD.18 Furthermore, radiation exposure increases endothelial permeability with subsequent intimal infiltration of lipids. Activation of lysosomal enzymes within the intima and media lead to the formation of cholesterol plaques that are vulnerable to thrombosis.17
In the chronic phase, coronary artery fibrosis occurs secondary to the release of pro-fibrotic cytokines (IL-4 and IL-13), platelet-derived growth factor, transforming growth factor beta (TGF-beta), basic fibroblast growth factor and insulin-like growth factor.19 Of note is the role of TGF-beta, which is directly activated by ROS to promote up regulation of collagen synthesis, provoke myofibroblast activation and ultimately trigger extracellular matrix production that leads to fibrosis. TGF-beta also increases the synthesis of protease inhibitors to prevent degradation of the matrix and to further amplify the fibrotic process.17 Sub-endothelial and microvascular fibrosis are of clinical relevance due to the resultant microvascular angina that provides a distinct diagnostic challenge.18
Preventing the development of RICAD
Advances in radiotherapy treatment techniques can be used to reduce cardiac dose. Computed tomography (CT) simulation and 3D conformal radiotherapy (3DCRT) planning can reduce dose through outlining the heart as an organ at risk, and therefore limit the dose to accepted tolerance thresholds for toxicity. Furthermore, intensity-modulated radiotherapy (IMRT) and volumetric modulated arc therapy (VMAT) techniques can provide even more conformal treatment plans through the use of one or multiple beam arcs, reducing dose to the heart.20 However, IMRT treatment results in a wide irradiated low-dose ‘bath’ and potentially increased cardiac dose, when this could be avoided with the use of 3DCRT. Furthermore, the deep-inspiratory breath hold (DIBH) technique for treating left-sided breast cancer is now used routinely in the UK to displace the breast/chest wall away from the heart during treatment and thus decrease cardiac dose.21
Consideration should also be given to treatment modality; eg photon, electron or proton therapy and their respective depth dose deposition profiles. In particular, proton therapy has several benefits regarding the reduction in radiation delivered to the healthy surrounding tissues. Although most commonly used for tumours proximal to the spinal cord, proton beam therapy is being explored for treatment of early breast cancer to limit the irradiated volume and reduce dose at depth, ie the cardiac dose.22 This hopefully may reduce the prevalence of RICAD over time.
There are no current guidelines regarding specific parameters for blood pressure, diabetic control, and use of statins and anti-hypertensives in the population of post-radiotherapy patients. It is also important to note the cardiovascular risk calculators such as QRISK2 (as recommended by the National Institute for Health and Care Excellence) and SCORE2 (as recommended by ESC) also do not take into consideration the patient's history of cancer treatment and, therefore, may underestimate their cardiovascular risk.23,24 A limited number of studies have generated risk scores specifically for oncology patients, however, none have currently been prospectively validated.25,26 Overall assessment of cardiovascular risk in post-radiotherapy patients requires an individualised approach and a suggested algorithm for risk assessment is proposed in Fig 1.
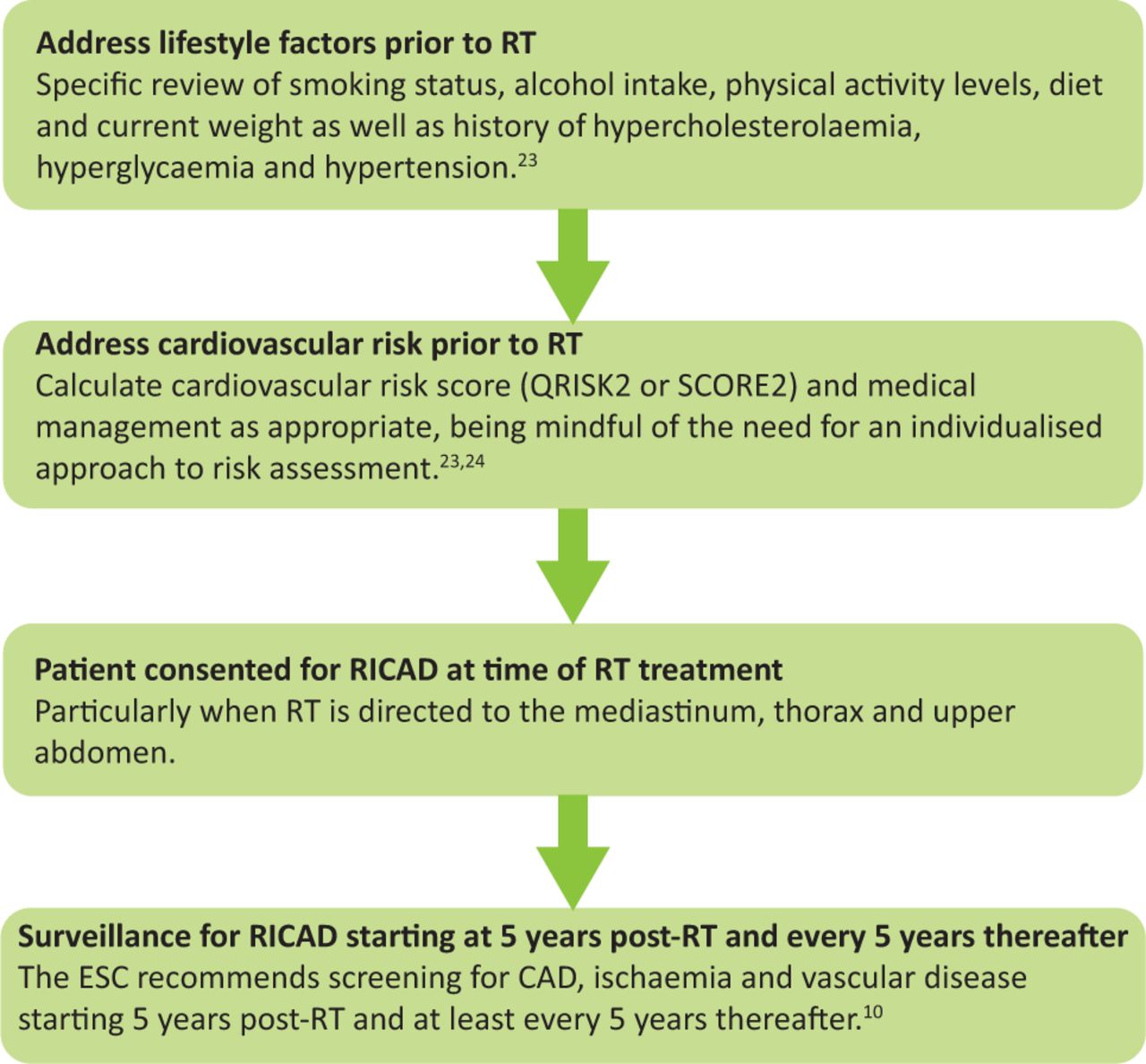
Suggested process for assessment and prevention of radiation-induced coronary artery disease. CAD = coronary artery disease; ESC = European Society of Cardiology; RICAD = radiation-induced coronary artery disease; RT = radiotherapy.
It is important to appreciate that post-radiotherapy patients represent a comorbid population. Studies of cancer survivors beyond 5 years post-diagnosis have demonstrated a 1.7-to-18.5-fold increased incidence of cardiovascular disease risk factors including hypertension, diabetes mellitus and dyslipidaemia when compared with age-matched counterparts without a history of cancer.27
Whether concurrent treatment at the time of radiotherapy exposure, with anti-inflammatory medications (specifically statins, colchicine, clopidogrel and aspirin) could act as prophylaxis against the development of RICAD is an area that warrants future research.28 Early evidence also shows a potential role for primary prevention of RICAD with use of angiotensin-converting enzyme (ACE) inhibitors and antioxidants but prospective human studies remain lacking.29 Overall, in absence of this specific trial data, the primary prevention of CAD should continue as per general guidance with reference to the patient's overall risk of CAD.
Diagnosis of RICAD
The presentation of RICAD includes the development of angina, MI and, potentially, ischaemic heart failure.10 However, RICAD patients will more frequently present with either atypical or even ‘silent’ symptoms compared with their non-irradiated counterparts.30 This is likely because of multiple factors including autonomic dysfunction following radiation exposure.31 Groarke et al demonstrated that autonomic dysfunction resulted in elevated resting heart rate and abnormal heart rate recovery in patients requiring thoracic radiotherapy for Hodgkin's lymphoma.32 An abnormal recovery heart rate was associated with significantly increased all-cause mortality (age-adjusted hazard ratio 4.60; 95% CI 1.62–13.02).32
The ESC recommends evaluation for CAD, ischaemia and vascular disease in patients with a history of mediastinal radiation, even if asymptomatic, starting 5 years post-treatment and then at least every 5 years thereafter.10 A suggested algorithm for surveillance of patients following radiotherapy is proposed in Fig 2. In addition, it is important to note that radiation-induced aortic valve disease, although a distinct entity from RICAD, is another example of a late complication of mediastinal radiotherapy and its detection should also prompt further assessment for RICAD.10
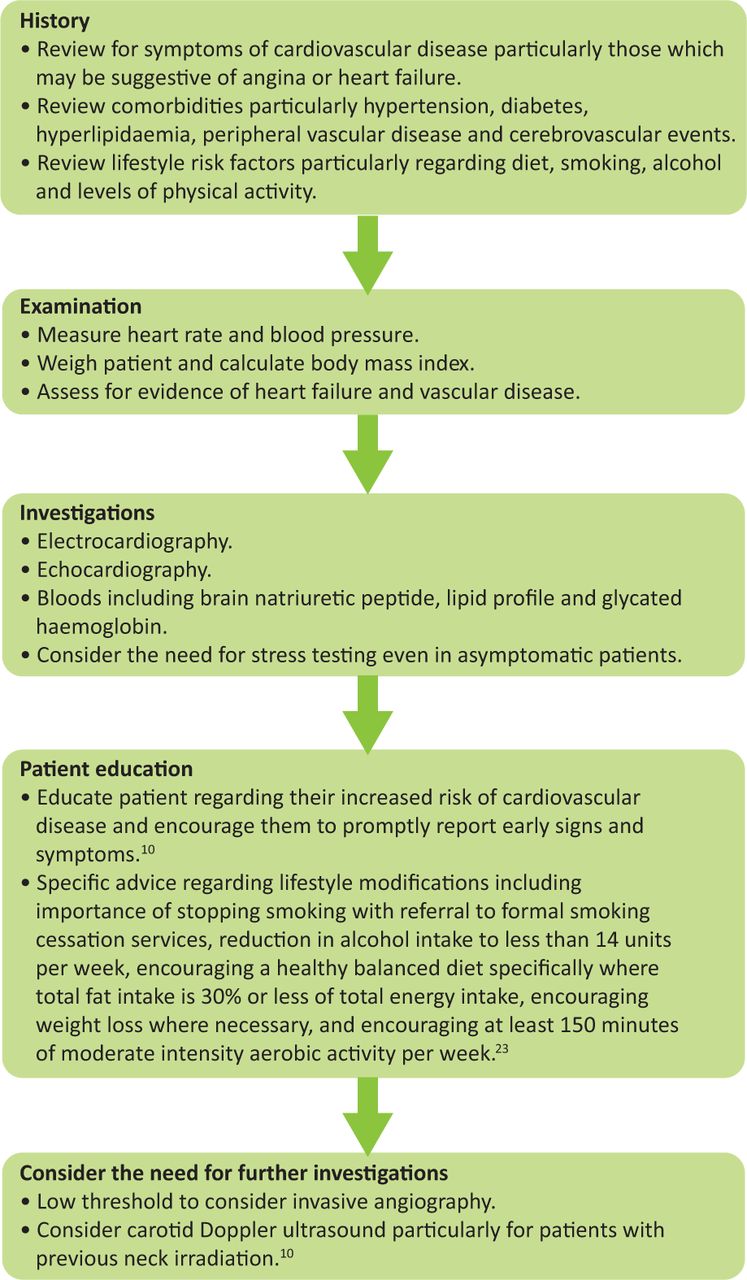
Suggested process for surveillance of patients following radiotherapy at 5 years post-treatment and every 5 years thereafter.
There are several validated diagnostic approaches to screening and assessing for RICAD. Desirable characteristics of a screening modality include minimal radiation exposure with maximal clinical information and reproducibility so that myocardial perfusion imaging using technetium-99m tetrofosmin, stress echocardiography, and cardiovascular magnetic resonance with stress perfusion and CT coronary angiography with or without coronary artery calcium scoring are all possible techniques to screen for RICAD.33 The choice of a specific imaging modality will largely depend on clinical expertise and availability. However, it should be noted that some abnormalities observed at perfusion imaging do not correspond to coronary artery territories, suggesting that they may be due to microvascular dysfunction.33 Furthermore, the introduction of fractional flow reserve in CT coronary angiography may reduce the amount of unnecessary invasive coronary angiographies due to a reduction in false positive perfusion stress tests caused by microvascular ischaemia.34
Depending on the non-invasive imaging, some patients may proceed to invasive coronary angiography. Clinicians should have a lower threshold to performing invasive coronary angiography in this group due to the known risk of accelerated atherosclerosis.35 Intravascular ultrasound can be particularly useful in assessing RICAD and appearances can range from heavy calcification to significant neointimal hyperplasia or negative re-modelling that has been described following radiation exposure.36
Management of RICAD
The management of RICAD is similar to the treatment of CAD in non-irradiated patients and the optimal management requires a multifaceted approach. Aggressive secondary prevention including controlling medical and lifestyle factors such as smoking, obesity, hypercholesterolaemia, hyperglycaemia and hypertension is mandatory as these factors act synergistically with radiation exposure to increase the lifetime risk for major coronary events from 2% to 7%.37
Medical management of known CAD is key for control of symptoms, halting progression of atherosclerosis, reducing the risk of cardiovascular events and improving mortality. All patients with CAD should be initiated on low-dose aspirin (75 mg once daily) in the absence of any contraindications, and high-dose statins (such as atorvastatin 80 mg once nightly) should be offered to all patients irrespective of formal lipid profile results and with an aim to decrease low-density lipoprotein cholesterol (LDL-C) by at least 50% of the patient's baseline and an ultimate LDL-C goal of <1.4 mmol/L.11,24 ACE inhibitors targeting a blood pressure <140/90 mmHg are recommended for co-existing left ventricular dysfunction with ejection fraction <40%, diabetes or chronic kidney disease. Beta blockers and calcium channel blockers remain the first-line therapy for controlling the symptoms of stable angina. In general, for diabetic patients, glycated haemoglobin targets should be <53 mmol/mol, however, more stringent goals may be chosen for selected patients.24 The key targets for medical management are summarised in Table 1.
European Society of Cardiology recommendations for medical management of coronary artery disease and relevant treatment targets
There is some debate about whether percutaneous coronary intervention (PCI) outcomes in patients with RICAD are the same as those in the general population. While Fender et al demonstrated that there was no difference between the two groups post-PCI, Veeragandham et al suggest that there is a higher rate of restenosis in stented vessels in the irradiated cohort.8,34 Further studies are required to better understand the long-term outcomes of PCI in this cohort.
Desai et al demonstrated that, in patients undergoing CABG surgery, mortality was significantly higher in patients with RICAD compared with the general population.37 Furthermore, patients with RICAD had a higher rate of restenosis of bypassed vessels compared with the general population.8 In radiotherapy studies, surgical intervention and CABG experienced difficulties due to mediastinal fibrosis, with a high incidence of complications.8
It should be noted that, because radiation may cause multiple types of heart disease in one patient, CABG has the potential of being performed during the same operation including interventions for complications of radiotherapy (such as pericardiectomy or valve surgery) and may therefore reduce the need for reoperation. However, if a patient only requires coronary revascularisation, it may be reasonable to consider PCI as a first-line therapy, but this should be an individualised decision based on the specific sites of the patient's disease. Borges et al suggest that surgical intervention should be considered as a last resort as outcomes in patients undergoing redo cardiac surgery are significantly worse in patients with previous radiation exposure compared with the general population.38
Ultimately long-term research to directly compare PCI with CABG outcomes is required to identify the optimal modality of revascularisation in this complex patient cohort.
Conclusion
There is a strong association between radiation exposure and the development of CAD. Prompt diagnosis of CAD can be challenging in this cohort due to its silent or atypical presentation and, therefore, the difficulty in diagnosis. Screening programmes can help bridge this gap and aim to reduce the morbidity and mortality surrounding RICAD. Such programmes may also provide more information on progression of coronary plaques post-radiation therapy and, furthermore, will improve understanding of the long-term durability of the differing modes of revascularisation. Overall, RICAD is a complex phenomenon that the oncologist, cardiologist and general medical physician should be aware of and be vigilant for.
Key points
Radiation-induced coronary artery disease (RICAD) typically presents after a latency period of 15 years following radiotherapy treatment. Patients may present with atypical or even ‘silent’ symptoms of coronary artery disease.
Patients who are at a high risk of RICAD include those receiving radiotherapy directed at the thorax, mediastinum or upper abdomen; those receiving higher doses of radiotherapy; those of a younger age at time of exposure to radiotherapy; and those with pre-existing cardiovascular risk factors. RICAD is the second most common cause of morbidity and mortality in patients treated with radiotherapy for breast cancer, Hodgkin's lymphoma and other mediastinal malignancies.
Aggressive control of cardiovascular risk factors is warranted following a confirmed diagnosis of RICAD. As many patients are asymptomatic, proactive surveillance of individuals who have received radiotherapy to the mediastinum is recommended.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}