
ABSTRACT
A 60-year-old woman presented with sudden-onset epigastric pain, vomiting and small volume rectal bleeding. She had a history of mechanical mitral valve replacement, for which she was on warfarin. Computed tomography (CT) angiography of the abdomen showed gallstones, a fluid-filled stomach and faecal loading. She subsequently deteriorated with worsening abdominal pain and haemodynamic instability. Non-contrast CT showed small bowel ischaemia and infarction. She rapidly deteriorated and a decision was made that surgery was likely to be futile. She died soon afterwards. On review of the initial CT angiography, an occlusion within the superior mesenteric artery (SMA) was visualised. The post mortem showed small bowel infarction due to embolic occlusion of the SMA secondary to bacterial endocarditis of the prosthetic mitral valve. This case should prompt awareness among clinicians that acute mesenteric ischaemia secondary to septic embolisation should be considered in patients with risk factors for infective endocarditis presenting with acute abdominal pain.
Case presentation
A 60-year-old woman presented to the emergency department with sudden-onset severe epigastric pain, vomiting and small volume rectal bleeding. Her past medical history included hypertension and a mechanical mitral valve replacement, for which she was on warfarin. On examination, she had a systolic murmur, her abdomen was soft but tender in the epigastrium, and digital rectal examination revealed a small amount of dark red blood. Electrocardiography showed new-onset atrial fibrillation (AF). Initial blood tests revealed a white cell count (WCC) of 21.92 × 109/L, a neutrophil count of 18.43 × 109/L, an international normalised ratio (INR) of 4.5, a C-reactive protein (CRP) of 2 mg/L and a lactate of 4.1 mmol/L. She was treated as having presumed gastritis and was started on ciprofloxacin to cover for possible diverticulitis. Computed tomography (CT) angiography of the abdomen showed uncomplicated gallstones, a distended stomach with fluid extending into the distal oesophagus and faecal loading in the ascending and transverse colon.
On day 1 post-admission, she was reviewed by the general surgery and gastroenterology teams with a plan to perform an oesophagogastroduodenoscopy if she did not improve. Repeat INR was 8.1, likely secondary to interaction between warfarin and ciprofloxacin. There were no signs of active bleeding and she was given 2 mg of vitamin K.
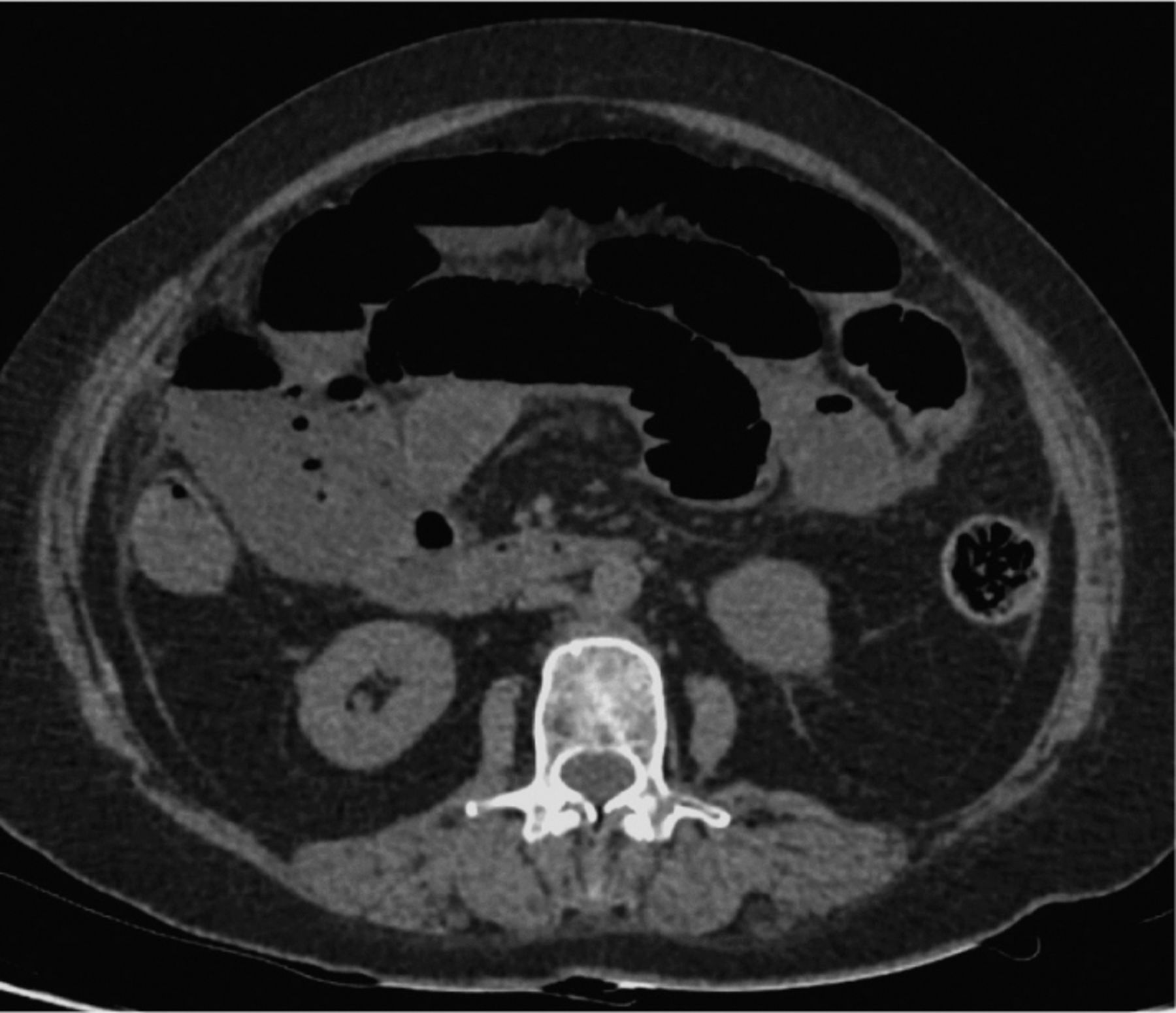
On day 2 post-admission, she complained of worsening abdominal pain and became tachycardic and hypotensive. Her abdomen was distended, firm and tender on palpation. Blood tests showed an INR of 20, CRP of 225 mg/L and a lactate of 6.4 mmol/L. She was resuscitated with intravenous fluids, her antibiotics were escalated and she was given further vitamin K and Beriplex (a prothrombin complex). Non-contrast CT of the abdomen showed findings consistent with superior mesenteric artery (SMA) occlusion with evidence of ischaemia in the small bowel loops with luminal dilatation, wall thickening, interloop fluid and possibly areas of infarction (Fig 1). She was reviewed by the general surgery team but she continued to deteriorate rapidly, and a decision was made against surgery as it was thought to be futile. She sadly died soon afterwards. The post mortem confirmed a small bowel infarction due to embolic occlusion of the SMA secondary to bacterial endocarditis of the prosthetic mitral valve.
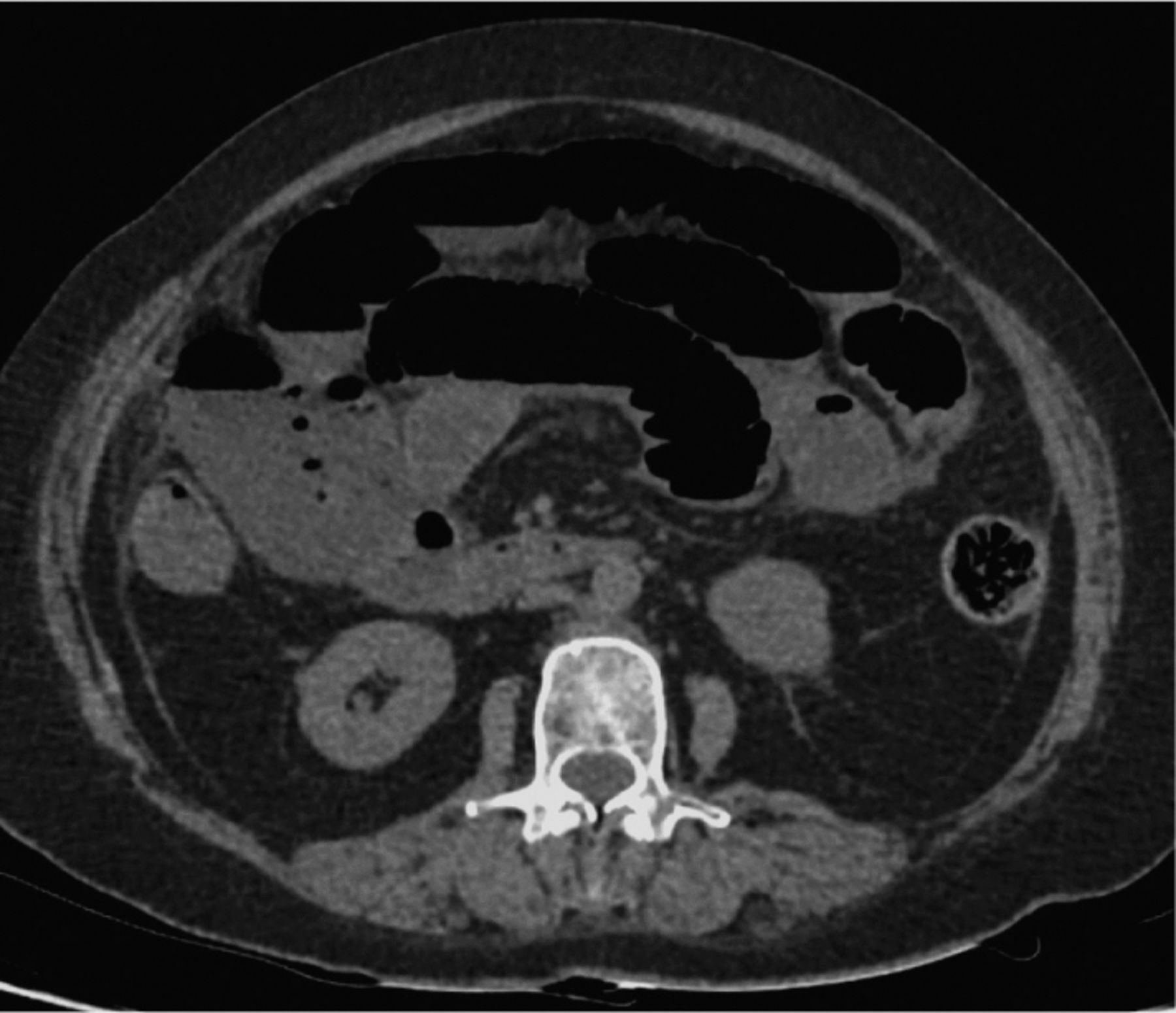
Axial non-contrast computed tomography demonstrating luminal dilatation, some wall thickening and interloop fluid suggesting small bowel ischaemia and possibly areas of infarction.
On subsequent review of the admission CT angiography, an occlusion within the SMA was in fact seen, but which was not initially reported (Fig 2).
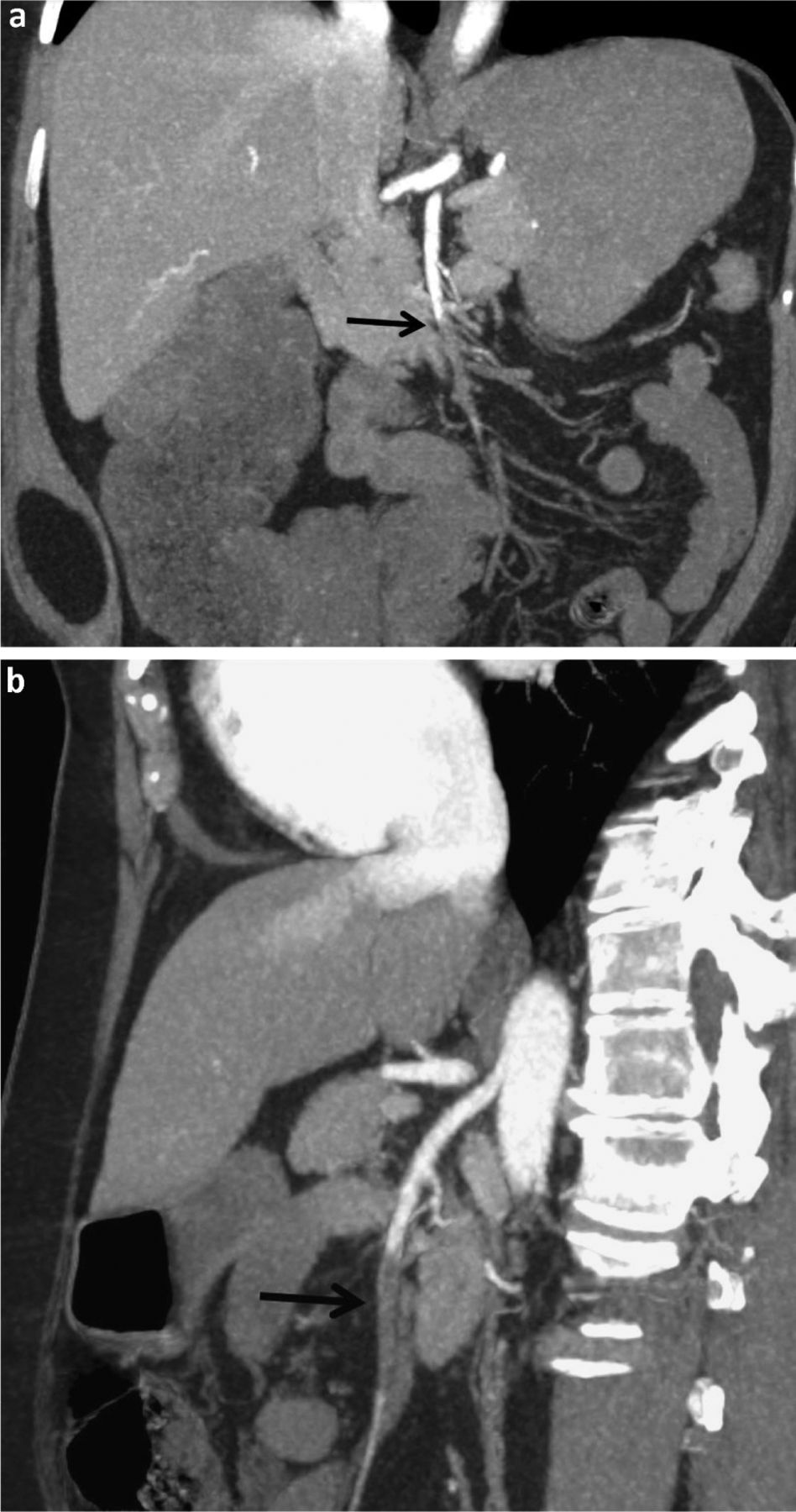
Multiplanar reformat maximum intensity projection computed tomography angiography of the superior mesenteric artery (SMA) following the administration of intravenous contrast in the arterial phase; there is abrupt non-enhancement of the distal SMA (arrows) representing, in this case, septic emboli.
Discussion
Septic embolism secondary to endocarditis occurs in approximately 40% of patients.1 Mesenteric artery embolus is an uncommon complication of infective endocarditis. The anatomic distribution in a study of 68 patients, of whom 35 experienced embolisation, was reported that the central nervous system was the most common (n = 21), followed by the spleen, kidney, liver and musculoskeletal system.2 The least common was the mesenteric artery (n = 1).
We performed a literature search and found only six case reports of mesenteric ischaemia secondary to infective endocarditis. Three identified mitral valve vegetation as the source of embolus causing SMA occlusion.
Eickhoff et al described a case where a 26-year-old woman presenting with fever, abdominal pain and diarrhoea had initially been diagnosed with ulcerative colitis after abdominal CT showed pancolitis.3 Blood cultures grew Staphylococcus epidermidis and clinicians had detected a cardiac murmur on presentation, but infective endocarditis was not suspected until new sudden-onset abdominal pain prompted a repeat CT with contrast that showed an SMA thrombus. Subsequent transthoracic echocardiography (TTE) revealed a mitral valve vegetation.
In another case report by Misawa et al, a 75-year-old woman with rheumatoid arthritis presented with persistent fevers, abdominal pain and diarrhoea.4 CT showed evidence of diffuse embolic phenomena with SMA occlusion, and bilateral renal and splenic infarcts. Following this, TTE confirmed a diagnosis of infective endocarditis of the mitral valve.
In a third case, the patient had already been recently diagnosed with infective endocarditis and started on antibiotics.5 After presenting with right-lower quadrant abdominal pain, SMA embolus and mesenteric ischaemia were confirmed on CT performed by clinicians suspecting appendicitis.
In our case, there were some features on presentation pointing towards mesenteric ischaemia, including the sudden-onset nature of the abdominal pain, raised lactate and new-onset AF. However, apart from hypertension, the patient did not have other typical metabolic risk factors for mesenteric ischaemia. Furthermore, mesenteric thrombosis seemed less likely as she was already anticoagulated. Despite this, she did undergo CT angiography of the abdomen to look for evidence of mesenteric ischaemia. Unfortunately, while this did show evidence of SMA occlusion, it was not reported. In the other cases, infective endocarditis was either already a confirmed diagnosis or suspected after CT reported clear SMA embolic disease. It is possible that, had evidence of embolic phenomena been reported on the CT, there would have been a higher clinical suspicion of infective endocarditis prompting further investigation with TTE.
While infective endocarditis is a cause for mesenteric ischaemia, it is a very rare cause of this, and would not necessarily have been considered as being implicated in her clinical presentation. The patient was asymptomatic from infective endocarditis and did not present with typical features of it; CRP at presentation was normal and the patient was apyrexial, which added to the diagnostic challenge. However, the patient did have a risk factor for infective endocarditis in that she had a history of prosthetic valve surgery.
Management of such a case is complex and requires a multidisciplinary approach involving medical, surgical and cardiothoracic teams. Prompt antibiotic administration remains the most important initial treatment. Early cardiac surgery is also a consideration in the prevention of embolic complications. Risk factors for embolisation include size and degree of mobility of the vegetation, prosthetic valve localisation, and Staphylococcus aureus aetiology.6–8 The European Society of Cardiology guidelines recommend urgent surgery for a vegetation >10 mm with previous embolisation or for isolated vegetation >15 mm.9 Unfortunately, in our case, the patient's clinical condition deteriorated rapidly before infective endocarditis was confirmed for this to be a consideration.
Conclusion
In summary, acute mesenteric ischaemia is a rare complication of infective endocarditis and can be challenging to diagnose. Clinical suspicion should be raised in patients presenting with acute abdominal pain or confirmed SMA occlusion, and identifiable risk factors for infective endocarditis.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.