
Key points
In patients with atypical presentations or simultaneous acute multi-territory coronary infarcts, consider the possibility of coronary embolism. The use of intracoronary imagingguided interventions (eg intravascular ultrasound or optical coherence tomography) may be useful in these situations.
Timing of surgical intervention in native valve infective endocarditis is delicately balanced between the need to achieve a sterile surgical field and the risk of haemodynamic deterioration and/or septic embolism.
A close multidisciplinary collaboration approach (which may include interventional cardiologists, cardiac imaging specialists, infectious disease specialists, neurosurgeons and cardiothoracic surgeons) is essential to achieve timely and appropriate clinical management in cases of complicated infective endocarditis.
Introduction
Infective endocarditis (IE) can present with a myriad of clinical syndromes, which make initial clinical diagnosis elusive.1–3 We describe a rare case of native mitral valve IE presenting with multi-territorial myocardial infarction and subsequently complicated by peripheral emboli and cardiogenic shock. We discuss the clinical implications, importance of detailed initial clinical assessment and timely diagnostic imaging in the care of patients with suspected IE.
Case presentation
A 60-year-old woman with no known cardiovascular risk factors presented to the emergency department (ED) with severe substernal chest pain and dyspnoea of 8 hours' duration. She had visited her primary care physician 3 weeks earlier for lethargy, non-vertiginous dizziness and unintentional weight loss. She reported no clinical symptoms of bleeding. Preliminary investigation then showed anaemia with haemoglobin of 8.6 g/dL.
Initial clinical examination in the ED revealed a diaphoretic patient in moderate distress, with blood pressure of 122/77 mmHg and sinus tachycardia of 112 beats per minute. The patient was afebrile and with oxygen saturation of 98% on room air. Cardiovascular examination revealed conjunctival pallor, a soft pan-systolic murmur loudest at the left sternal edge, a displaced apex beat and minimal crackles on bilateral lung bases. There were no pedal oedema or peripheral stigmata of infective endocarditis. Digital rectal examination disclosed no signs of gastrointestinal bleeding. Abdominal and neurological examination were unremarkable. An electrocardiography (ECG) performed on arrival showed sinus tachycardia with marked anterolateral ST-elevation in the precordial leads V2–6, and lateral leads I and aVL (Fig 1). In view of the clinical presentation and ECG findings, the patient was referred for emergency percutaneous coronary intervention.
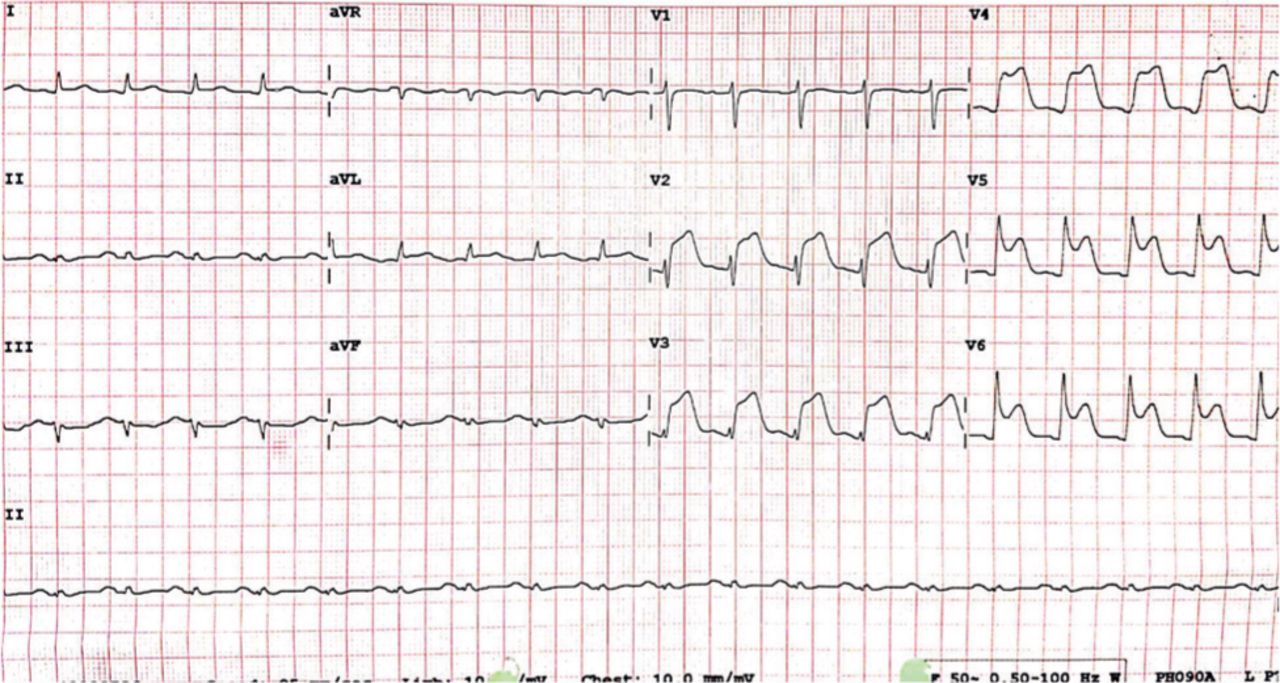
Electrocardiography showing anterior ST-segment elevation myocardial infarction.
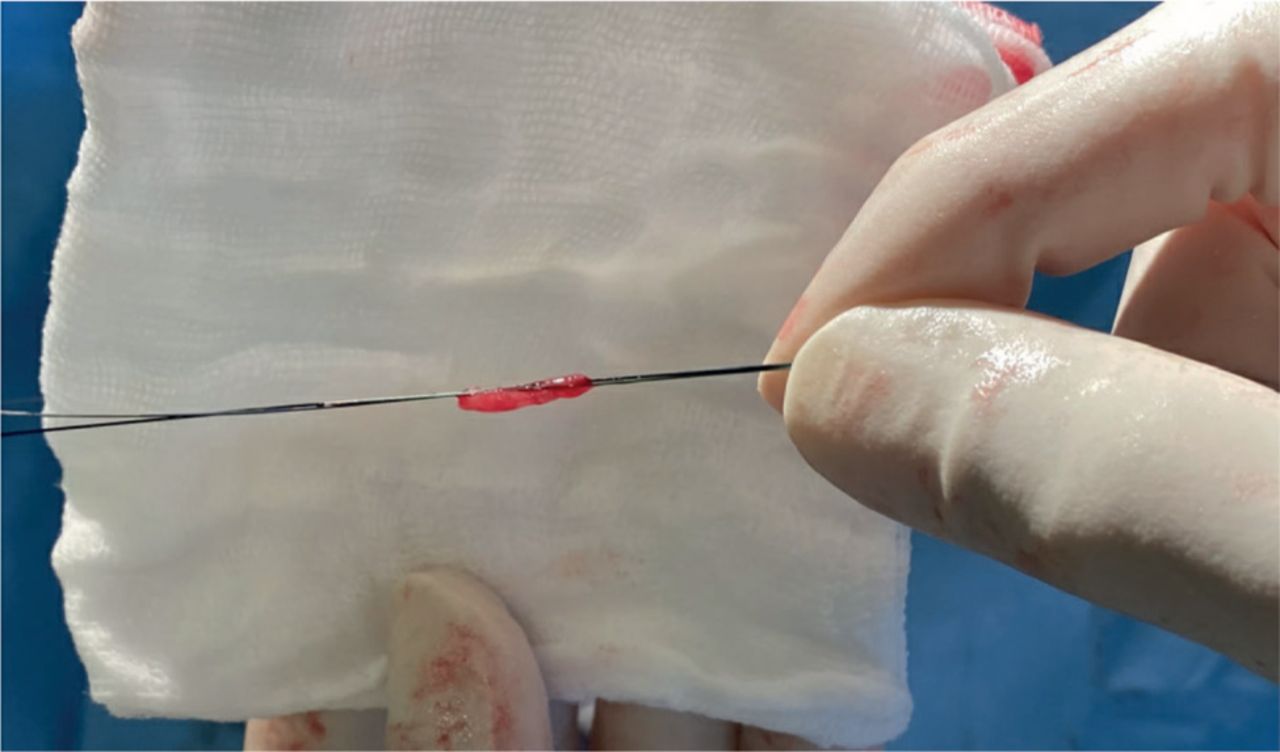
An emergency coronary angiography revealed complete occlusion of the mid-left anterior descending (LAD) and right posterolateral (RPL) arteries, with no other coronary lesions (Fig 2). Interrogation of the LAD revealed high thrombus burden, for which, multiple runs of aspiration thrombectomy were performed. Notably, mixture of red and white thrombi were recovered from the aspiration thrombectomy (Fig 3). Post-aspiration thrombectomy, thrombolysis in myocardial infarction (TIMI) 3 coronary flow was restored and intravascular ultrasound (IVUS) demonstrated no significant underlying coronary atheroma. The patient remained hypotensive post-procedure and an intra-aortic balloon pump was inserted.
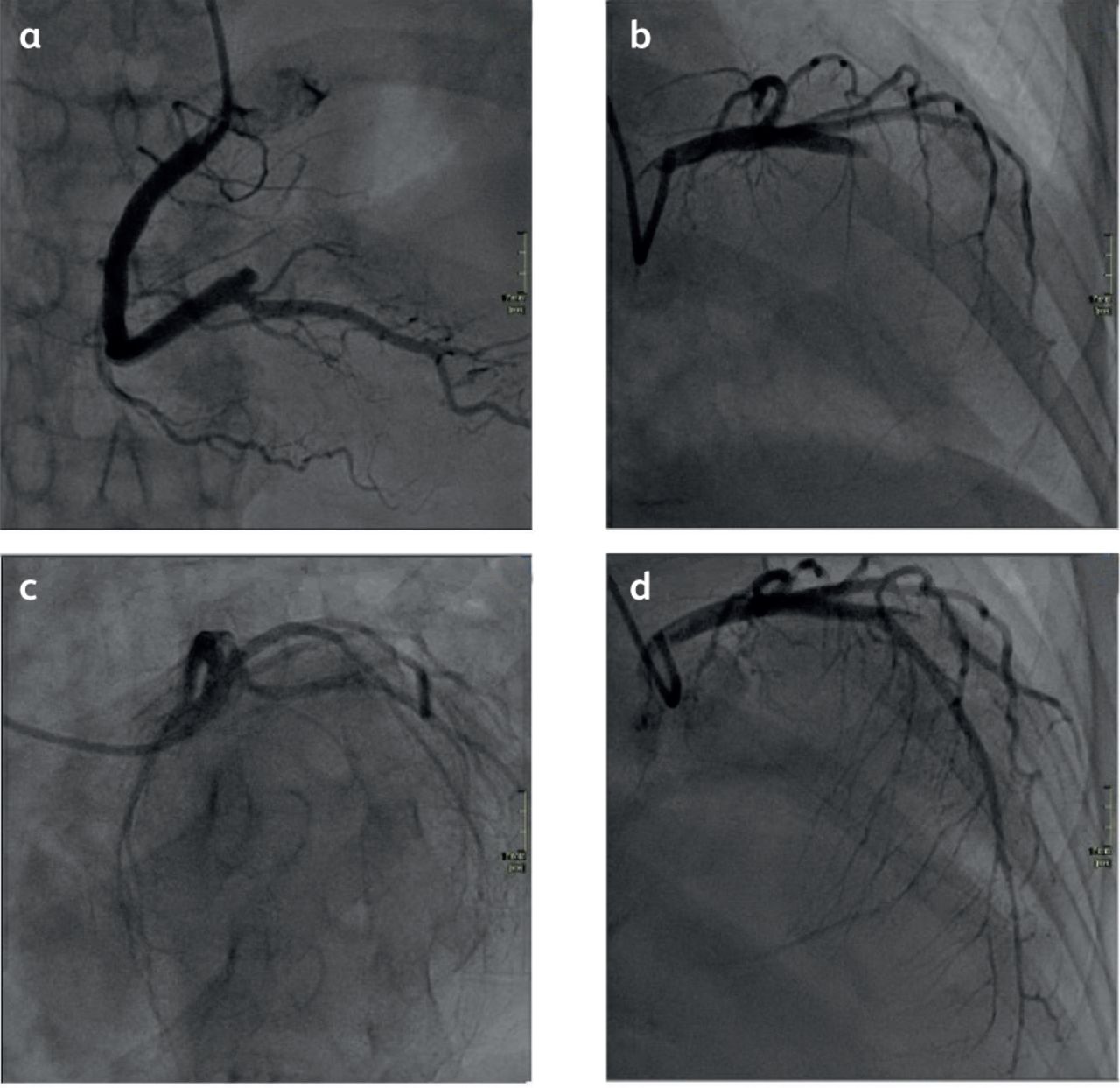
Coronary angiography showing left anterior descending artery and right coronary artery occlusions. a) Right coronary artery. b) Left coronary artery before percutaneous coronary intervention. c and d) Left coronary artery after percutaneous coronary intervention.

Thrombi recovered from aspiration thrombectomy during coronary angiography.
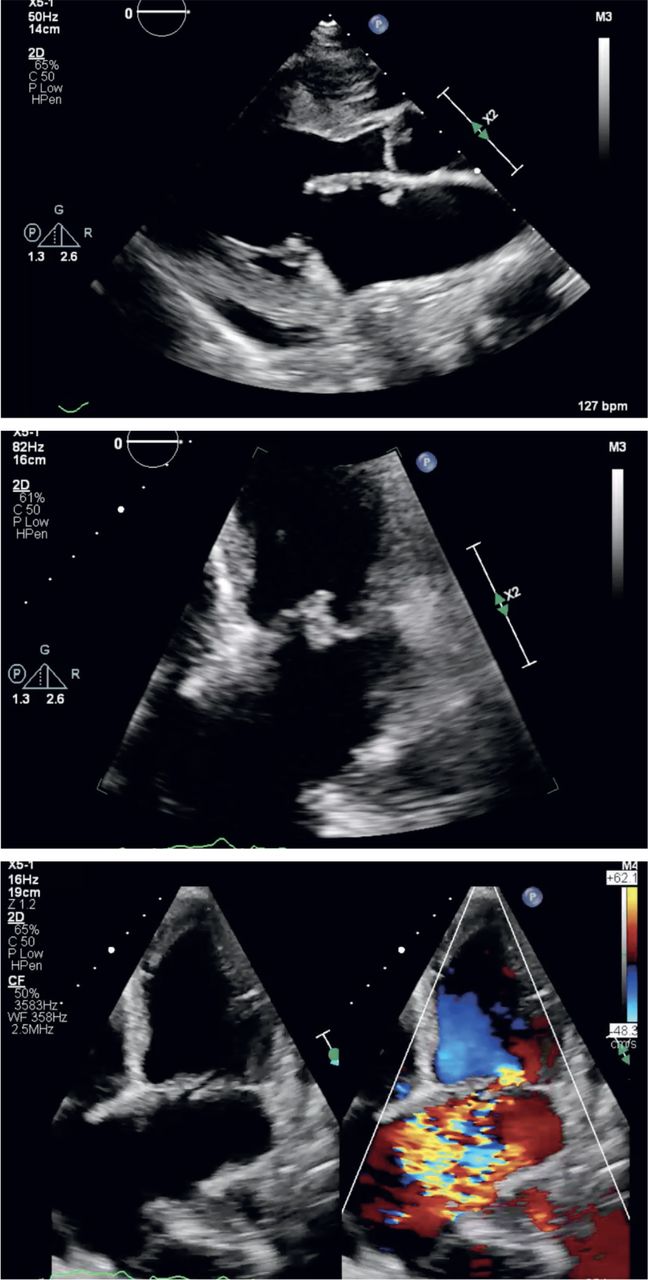
An echocardiography (Fig 4) performed afterwards showed mildly impaired left ventricle systolic function and severe, anteriorly directed mitral regurgitation due to flail posterior leaflet at P2 scallop (Carpentier classification). There were multiple masses compatible with mobile vegetation noted on the atrial surface of the anterior mitral leaflet and roof of the left atrium. After obtaining blood cultures, empirical intravenous antibiotic therapy for infective endocarditis was initiated. A joint decision for a delayed surgical approach was made together with the infectious disease and cardiothoracic surgery teams in view of a small subarachnoid haemorrhage noted on computed tomography of the brain. She also developed septic emboli to her digits, which were managed conservatively.

Echocardiography. a) Parasternal long axis view of mitral valve showing vegetations on mitral valve leaflets and left atrial wall. b) Apical fourchamber view of mitral valve with vegetations. c) Apical four-chamber view of mitral valve with severe mitral regurgitation.
On day 10 of admission, the patient deteriorated rapidly with new onset intermittent Mobitz type II atrioventricular block requiring temporary pacing (Fig 5). She underwent emergency mitral valve replacement surgery with implantation of a bioprosthetic mitral valve replacement (Fig 6). The surgery was successful; however, post-operative recovery was complicated by atrial fibrillation, acute kidney injury requiring temporary renal replacement therapy, and hospital-aquired pneumonia. She was admitted for a total of 3 weeks and was subsequently discharged and followed up at the outpatient cardiology and cardiothoracic surgery clinic.

Telemetry showing new onset 2.1 atrioventricular block.
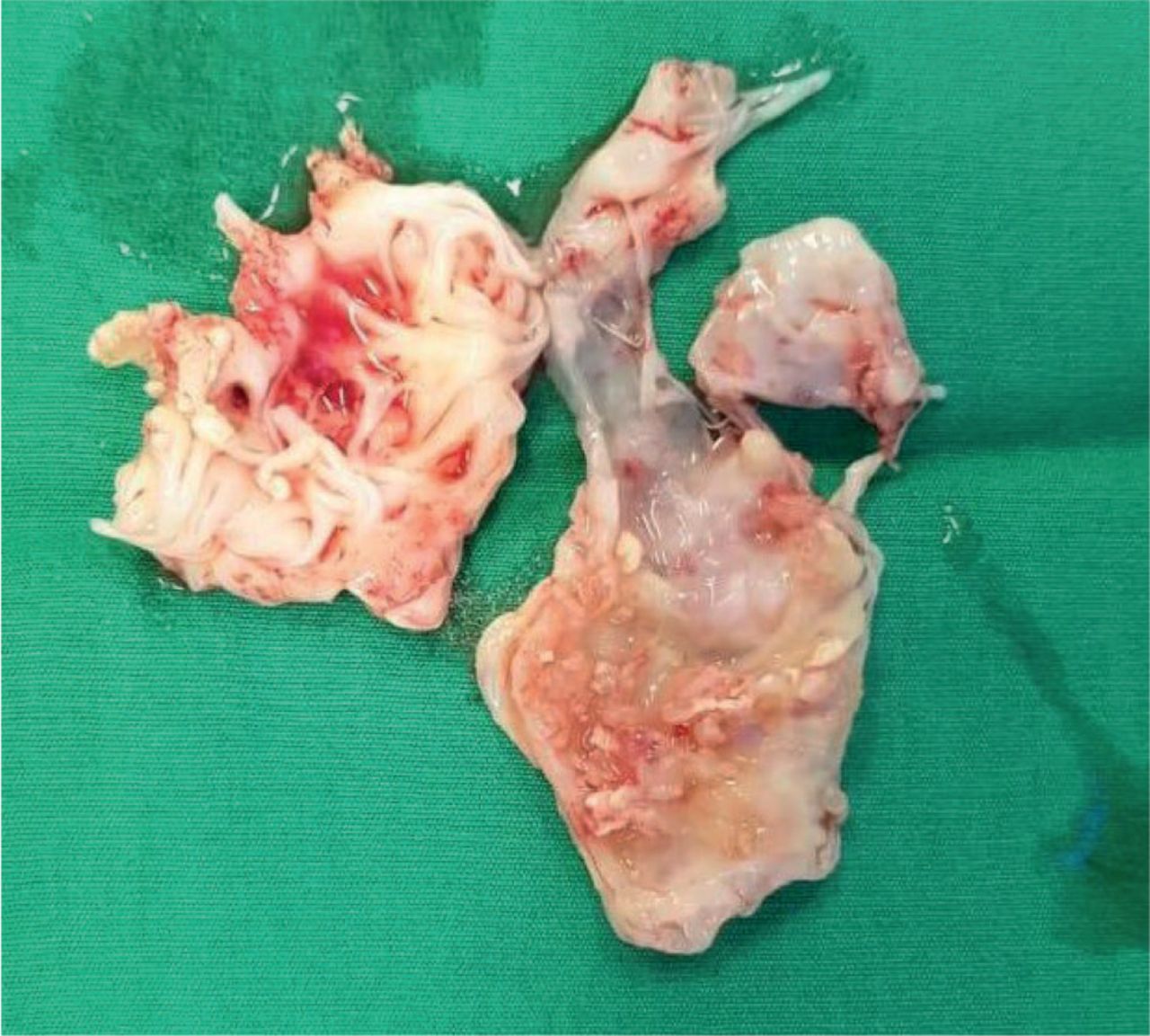
Intraoperative findings of excised mitral valve.
Discussion
Coronary embolism has been reported in 4%–13% of patients presenting with acute ST-segment elevation, of which, 8% is due to infective endocarditis.4 Treatment is often challenging, requires prompt coronary intervention and appropriate intravenous antimicrobial therapy. Surgical intervention would need to be considered early, especially in acutely unwell patients or those who deteriorate despite being on appropriate medical therapy. However, surgery carries a 15%–20% risk of mortality. The key to considering coronary embolism is the presentation of a simultaneous multi-territorial acute infarct. Differential diagnoses of embolic causes should be considered, and early echocardiography should be obtained to evaluate for intracardiac thrombus, infective endocarditis and intracardiac masses (like myxomas and fibroelastomas).
Mitral valve IE is associated with a higher risk of embolic events, especially when the anterior mitral leaflet is involved.2 The most common coronary involved in coronary embolism is the LAD artery, which has a less acute course when compared with the right coronary (RCA) and the left circumflex (LCX) arteries.2,5,6
During acute management of embolic ST-segment elevation myocardial infarction due to infective endocarditis, aspiration thrombectomy is preferred over the use of thrombolytic agents as there is an increased risk of intracerebral haemorrhage due to mycotic aneurysms and embolic strokes.7,8 The mental status of a patient should be monitored closely and early cerebral imaging should be performed to evaluate for intracranial complications. Intracranial complications include ruptured intracranial mycotic aneurysms, embolic strokes and intracranial haemorrhage.9 As soon as the diagnosis of IE is established, anticoagulation should be stopped to reduce the risk of catastrophic intracranial haemorrhage.10
In our case, the presence of multi-territory ST-segment elevation on ECG prompted immediate management with coronary angiography as per acute coronary syndrome. A bedside echocardiography prior to angiography would have been useful to evaluate the murmur noted on clinical examination, resulting in earlier recognition of IE, prompt initiation of antibiotic therapy and avoidance of anticoagulation that may have averted the intracranial haemorrhage.
Summary
Coronary embolism and IE should be considered in patients presenting with multi-territory ST-segment elevation myocardial infarction. A targeted echocardiography can be considered prior to transfer to primary percutaneous intervention to guide therapy in patients who have clinically relevant murmurs or atypical presentations.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.