
ABSTRACT
Older adults may experience a number of physiological changes that influence how acute pain is perceived, diagnosed and managed by healthcare professionals. Understanding these differences enables the identification, assessment and treatment of acute pain in older adults. Combining careful selection of pain medications with appropriate titration and monitoring allows the analgesic needs of this group to be met.
Key points
Both quantitative and qualitative methods of assessing pain are helpful in determining the choice of analgesia in the older adults.
Multiple factors determine the choice of analgesia prescribed for older adults including physiological changes, psychological issues, existing medications and cognitive function.
Under- or overtreatment of pain can have significant consequences, such as delirium and falls, so this must be considered when prescribing for older adults with acute pain.
Older adults should be given the lowest analgesic dose for the shortest possible time to adequately manage their pain: starting low and titrated cautiously.
Formally reassess the pain in older people to help guide the effectiveness of both the initial and ongoing treatments.
Introduction
Pain is the subjective experience of noxious stimuli and, in its acute form, is defined as pain lasting up to 3 months.1 Older adults may experience several physiological changes that influence how acute pain is experienced, as well as how it is diagnosed and managed by healthcare professionals. Acute pain is highly prevalent for all patients seen in both primary and secondary care, with estimates suggesting that more than 50% of hospital inpatients experience significant pain during their hospitalisation and that the prevalence of pain has been found to increase with age, particularly for those with a history of musculoskeletal problems and depression.2 This article aims to outline the age-related changes in physiology relating to pain that may alter the way pain is perceived for older adults, and outline the adjustments required when assessing and treating this pain.
Changes in ageing regarding nociception and perception of pain
There are a number of physiological changes that take place in the older adult that can affect their experience of pain. Nerve fibres, particularly the myelinated A-delta nerve fibres that produce the sensation of sharp localised pain decrease with age.1 Neurons in older adults do not regenerate and are replaced by proliferating non-neuronal glial cells reducing the response to pain. Further changes, including the loss of proprioception and altered peripheral nerve conductivity, increase the risk of injury leading to a higher likelihood of developing pain.1,3
Older adults are also more likely to experience multi-morbidity leading to an accumulation of potentially painful diseases as the prevalence of certain conditions linked to pain increases with age. These include conditions such as Parkinson's disease, post-stroke pain, degenerative spinal disease, arthritis and diabetic neuropathy.3 Older adults are also more likely to develop cognitive impairment, including dementia, which may result in an altered sensation of pain.4
Impact of pain in older adults
The impact of pain on an individual is wide ranging and is especially so in the older adult. Pain can result in functional impairment, sleep disturbance, reduced socialisation, depression, reduced mobility, and impaired or slowed rehabilitation. Studies have shown a 70%–80% reduction in the ability of older adults to perform activities of daily living for those with pain compared with those without pain, as well as decreased gait speed, weaker grip strength and decreased self-reported physical ability.5 Older adults, especially those with frailty, may have reduced functional reserves meaning that pain-related impairments may have a more profound impact on mobility, cognition and independence.
Assessing pain in older adults
Pain is a subjective phenomenon and cannot be directly measured. As a result, self-reporting pain measurement tools are used to quantify pain, including simple verbal rating scales, visual analogue scales and pictorial pain scales as well as more complex assessment tools such as the McGill Pain Questionnaire or the Brief Pain Inventory.6,7
It is important that pain is proactively explored with patients as they, and their carers, may underestimate pain by attributing it to the ‘normal’ ageing process, leading to under-reporting and, therefore, under-treatment. Patients and carers may also be concerned about the side effects or polypharmacy associated with analgesia and hence avoid reporting pain to healthcare professionals.3,8 It should also be recognised that the majority of older adults who experience pain will experience pain at multiple sites, and this must be considered when assessing pain. In one study, a fifth of older adults over 65 years old reported pain at four or more sites.5
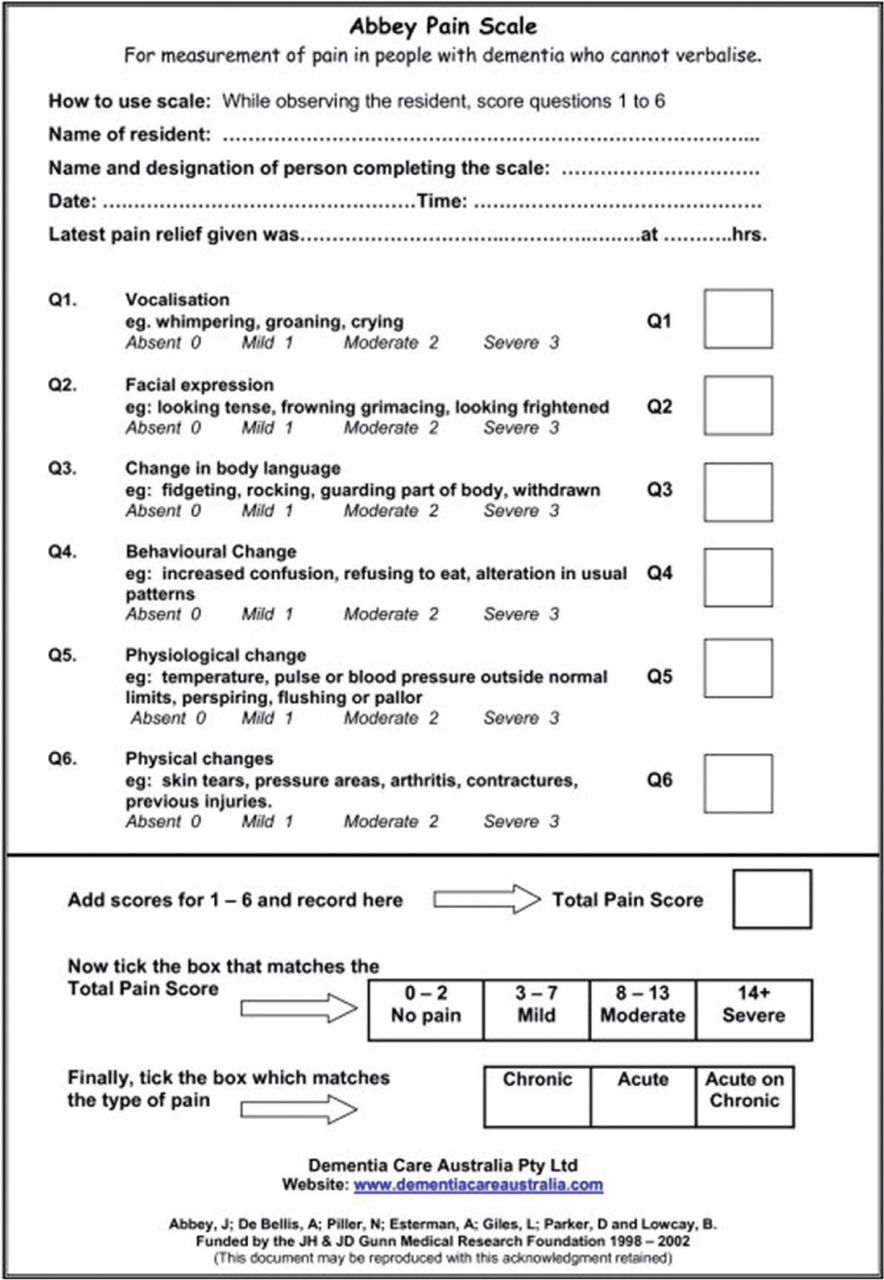
The most valid assessment of pain is self-reported, although this can be influenced by numerous factors (including mood, lethargy and sedating medications).9,10 It is also recognised that documentation of pain during inpatient admissions can be poor and higher pain scores may not necessarily result in the administration of more analgesic medications.11 In older adults, the assessment of pain may be further complicated as a consequence of cognitive impairment (such as dementia or delirium) or communication issues (such as aphasia), which may limit the reporting of pain and reduce the accuracy of these tools. For these patients, pain may be unreported and under-recognised. As a result, observational pain assessment tools have been devised that look at non-verbal behaviour (such as facial expression and changes in body language) combined with physiological changes associated with pain (such as tachycardia) to help elicit the level of pain. An example of such a tool is the Abbey Pain Scale (Fig 1) designed to measure pain in people with dementia who cannot verbalise.12

The Abbey Pain Scale. Designed to assess pain for patients who cannot verbalise their pain. Reproduced with permission from Abbey J, De Bellis A, Piller N et al. Abbey Pain Scale. Funded by the JH & JD Gunn Medical Research Foundation 1998–2002.
Effects of analgesia in the older adult
Older adults may experience the effects of analgesia differently to their younger counterparts for multiple reasons. Firstly, there are a number of age-related metabolic changes that alter the pharmacokinetics of analgesic medications. In the older adult, there is a decrease in total body water, meaning that water soluble medications (such as morphine) will have a smaller volume of distribution. There is also a decrease in lean muscle mass and an increase in body fat meaning that medications will have a smaller muscle volume of distribution and lipid soluble medications will accumulate. Further physiological changes include a reduction in hepatic and renal size, and blood flow, altering the potency, duration and clearance of analgesic medications.
Older adults are also more likely to experience multi-morbidity and polypharmacy. This may alter the impact of medications prescribed for pain due to the increased risk of drug–drug interactions and side effects.13–15 In clinical practice, this necessitates careful drug choice, dose adjustments and close monitoring of the effects of analgesics when they are prescribed for older adults. Specific impacts for the different categories of analgesia are outlined in Table 1.1–3,16,17
Specific impacts for different categories of analgesia
Treatment of pain in older patients
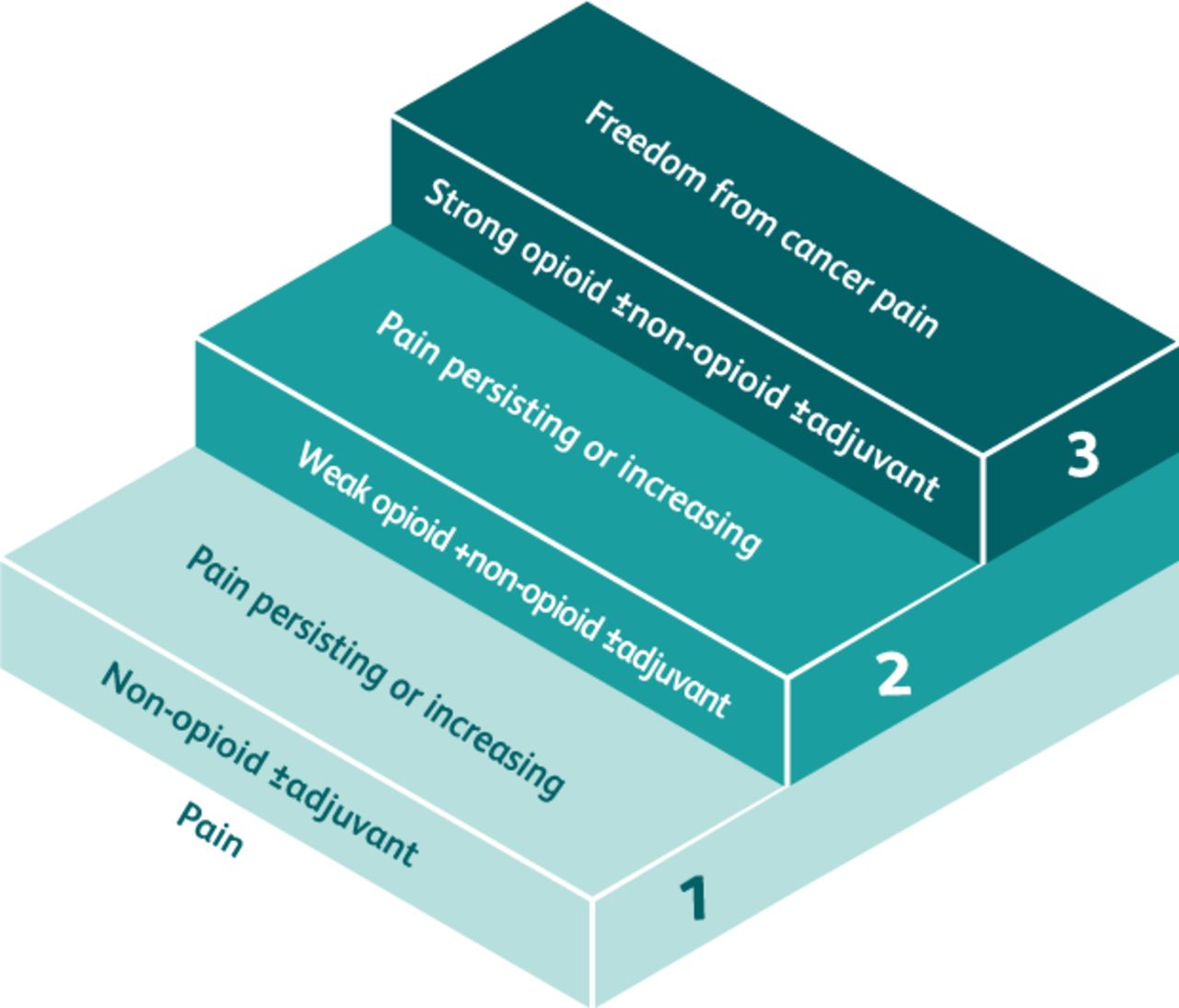
There are many non-pharmacological treatment modalities for acute pain management including the application of heat or ice, massage therapy, physiotherapy, and alternative therapies (such as acupuncture). In view of the issues outlined earlier regarding the challenges that prescribing medications for older adults present, non-pharmacological treatments tend to have fewer side effects and should generally be considered as a first-line therapy. However, these measures may not be sufficient, and so, analgesia often forms the cornerstones of treatment options for pain.2 The selection of analgesia is underpinned by the principles outlined in the World Health Organization (WHO) pain ladder (Fig 2).18
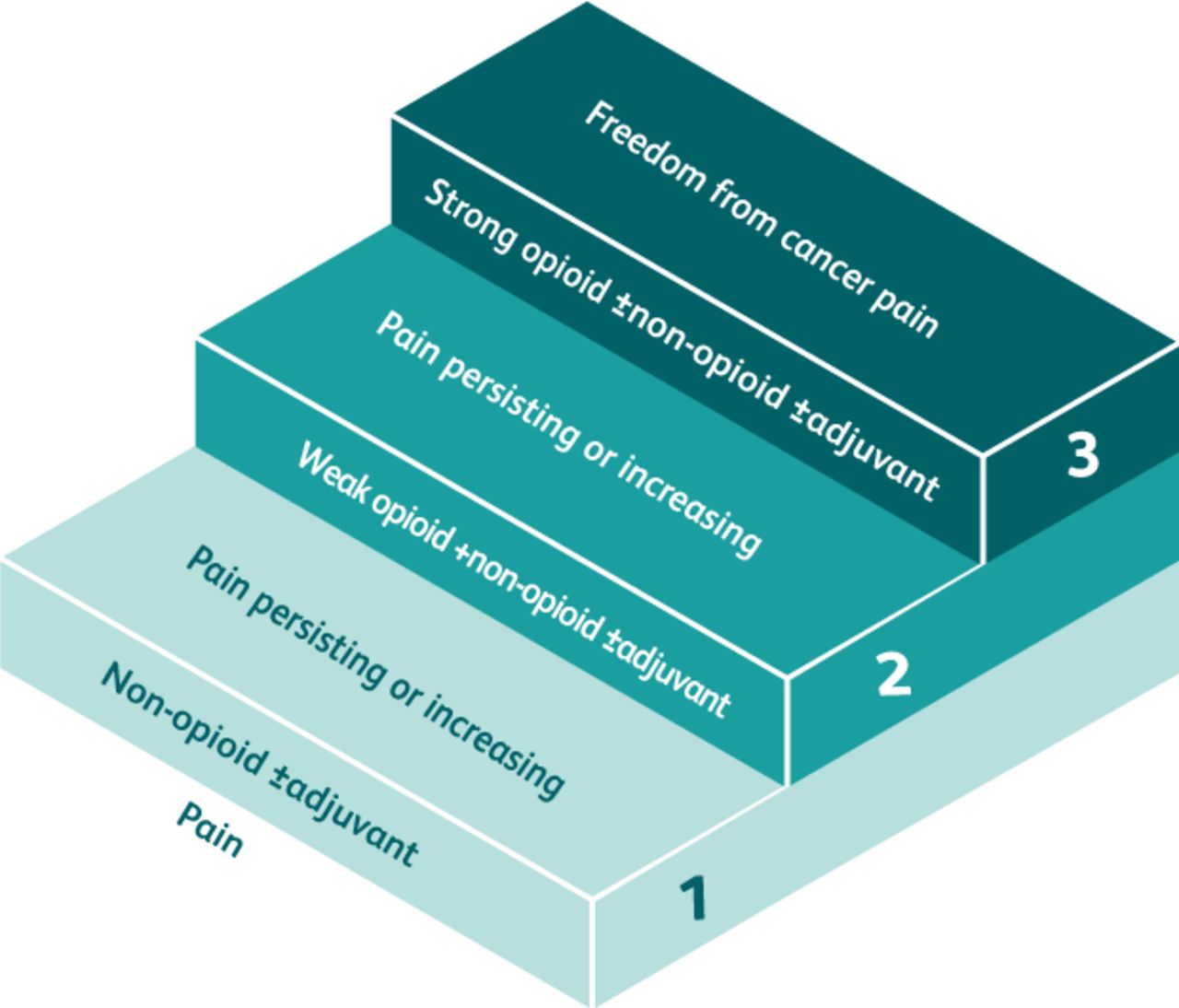
The World Health Organization pain ladder. Adapted with permission from World Health Organization. Cancer pain relief. WHO, 1986:19.
However, there are a number of considerations that are needed when analgesia is prescribed for the older person (Table 1).1–3 Specific regional forms of analgesia may be particularly effective in selective acute settings, such as the use of femoral nerve blocks following a neck of femur fracture. These have the advantage of reducing adverse systemic effects (such as cognitive dysfunction and sedation) but can be more challenging to administer for older adults.1,2 They may also require specialist training to administer and may not always be available.
Conclusion
Providing adequate analgesia for older adults in the acute setting can be challenging as a result of changes to physiology, polypharmacy, multi-morbidity and altered processing of medications combined with under-reporting and under-recognition of pain. Actively asking about pain and incorporating additional methods to accurately assess pain can be important, particularly for those who cannot communicate effectively. Combined with careful selection, titration and monitoring of analgesia, this will allow the analgesic needs of this patient group can be successfully met.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.